
Abstract
Objective:
To improve the safety and efficacy of ureteroscopic lithotripsy for the treatment of ureteral stone, we made a simple modification to the standard ureteral access sheath (mUAS) and developed a novel technique to overcome the deficiencies of the current procedure.
Materials and Methods:
We added an oblique suction-evacuation port with pressure regulating mechanism to the UAS to allow active egress of irrigation fluid and stone fragments. A pressure vent was placed on the egress port. Continuous negative pressure aspiration was connected to the egress port, whereas the continuous irrigation was delivered through the endoscope with a pressure pump. Stone fragmentation was performed using a holmium-YAG laser through a semirigid ureteroscope. Tiny stone fragments were evacuated in the space between the sheath and the scope. When larger fragments came into the sheath that were too large to exit between the scope and the sheath, the scope was withdrawn to just proximal to the bifurcation of the oblique port. This opened up an unimpeded egress channel for the larger fragments. We attempted this procedure in 104 consecutive patients.
Results:
Seventy-four patients had effective insertion of mUAS. Seven patients failed semirigid ureteroscopy despite effective placement of mUAS. Patient with effective semirigid ureteroscopic lithotripsy had 100% immediate stone clearance and no observed stone retropulsion. Patients who failed semirigid ureteroscopy were converted to flexible ureteroscopy. Five patients had completed stone clearance. The overall immediate stone-free rate was 97.3% and 100% at 1-month follow-up. Complications included two fevers and one minor ureteral false passage.
Conclusions:
Our modification of UAS has reduced stone retropulsion, improved stone clearance, improved visual field, and probably reduced the intraluminal pressure.
Introduction
U
To further improve the safety and efficacy of ureteroscopic lithotripsy for the treatment of ureteral stone, we made a simple modification to the UAS (mUAS) and developed a novel technique to overcome the deficiencies of the current procedure. We used the mUAS for the treatment of ureteral stones in 104 consecutive patients in 2 institutions and hereinafter report our preliminary experience.
Materials and Methods
The mUAS
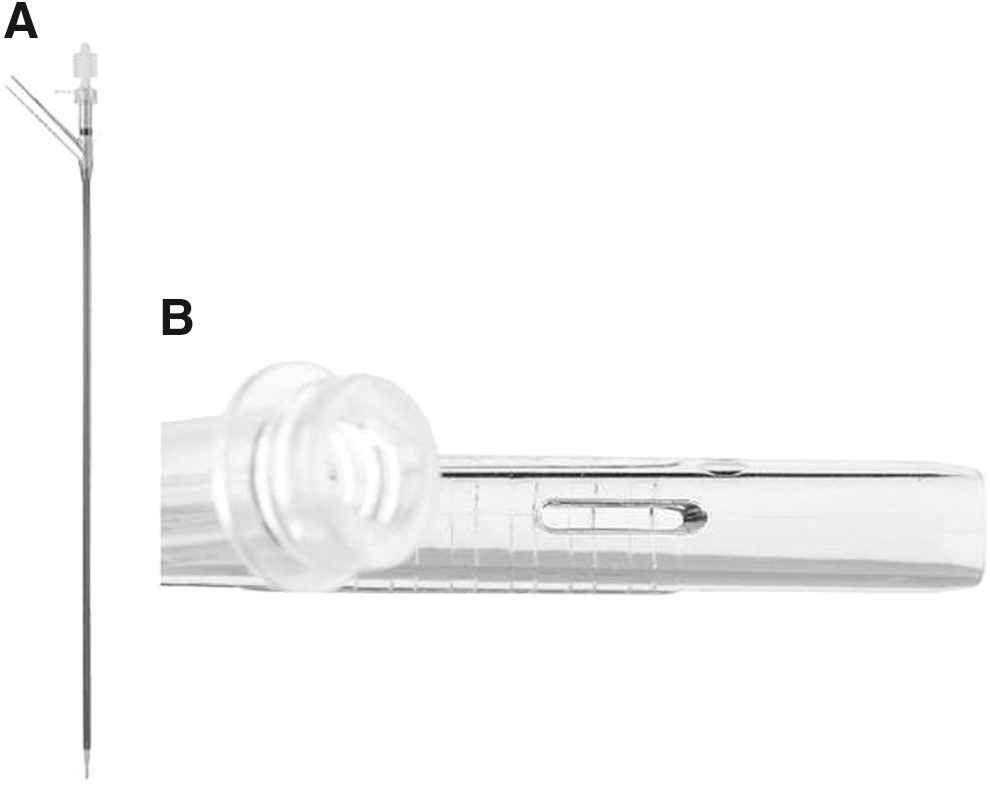
The sheath consists of distal straight and proximal bifurcated segments (Fig. 1A). The distal segment has a 35 cm length version for the upper ureteral stones and a 26 cm length version for the middle and lower ureteral stones. The 35 cm sheath will accommodate a 42 to 43 cm semirigid ureteroscope and the 26 cm sheath is for the 33 to 34 cm scope. The sheath is produced with the same material as the standard UAS. It has a 12F inside diameter and a 14F outside diameter.
Modified ureteral access sheath
The bifurcated proximal segment is constructed of a straight and an oblique tube in 45° angle. Both the distal and the proximal tubes all have the same luminal diameter. A rubber seal with a center aperture is placed at the proximal end of the proximal straight tube. There is a venting slit along the longitudinal axis of the oblique branch for regulating pressure (Fig. 1B). The proximal segment is 5.5 cm in length and is constructed with transparent plastic. This oblique sluice is connected to a negative pressure aspirator through a transparent tubing. A red band is placed just proximal to the bifurcation for demarcation. An obturator is used for the insertion of the sheath and it can be locked in place.
The mUAS was produced by an ISO certified medical device manufacturer (Well Lead Medical Co. Ltd., Guangzhou, China).
The patients
From August 2013 to October 2015, 104 consecutive patients with either ureteral stones or Steinstrasse who were candidates for ureteroscopic holmium-YAG laser lithotripsy were accrued in this study. Ureterovesical junction stones and small stones generally less than 4 mm that were better suited for basket extraction were excluded. This study was approved by the respective institutional ethics committees in both participating institutions. Written informed consent was obtained from each of the patients or their guardians. The sheaths were provided free of charge.
The procedure
The procedure was performed under either general or regional anesthesia. A stiff guidewire with flexible tip was inserted into the affected ureter in the lithotomy position either under fluoroscopic imaging or direct vision through ureteroscope. The flexible portion of the guidewire was passed beyond the impacted stone. The mUAS was passed over the guidewire to just below the stone. The position of the sheath was verified with fluoroscopy. Since we considered the mUAS as an experimental device, it was decided not to perform active ureteral dilation for the insertion of the sheath. If the insertion was unsuccessful after two attempts, this part of the procedure was abandoned. The treatment of ureteral stones proceeded either without the sheath or a Double-J stent was placed. Generally, we had no problem in inserting the mUAS when patient has had prior ureteral stenting.
Once the sheath was in proper placement, the obturator was removed. The rubber seal was placed and the oblique side branch was connected to a negative pressure aspirator. The aspiration pressure was set in the continuous mode and at 150 to 200 mm Hg. It was turned on before insertion of the ureteroscope with continuous pressurized irrigation. Either a 42 cm (Wolf) or 43 or 34 cm (Storz) ureteroscope that was at the least 3F smaller than the inside diameter of the sheath was used for the procedure.
The scope was inserted into the sheath through the seal thus maintaining the negative aspiration pressure. Pressurized irrigation was connected to the scope and the flow was adjusted to 60 to 80 cc per minute. The scope was advanced just beyond the sheath. This effectively created a continuous flow where the irrigation that came out of the sheath was immediately aspirated through the mUAS. This was pretty much the same principle used in the continuous flow resectoscope. The stone could usually be easily visualized. Occasionally the sheath had to be advanced few centimeters upward under direct vision. The distal end of the sheath was placed within 1 cm of the stone.
Stone fragmentation was accomplished using holmium-YAG laser. Higher frequency, 30 to 35 Hz, and lower energy, 0.5 to 0.6 J, settings were generally selected for the fragmentation. The tiny pulverized stone fragments would pass around the scope and exit through the oblique sluice. When the larger stone fragments that were too large to pass around the scope came into the sheath, the scope was withdrawn slowly to just proximal to the bifurcation (the red band). An unobstructed channel was thus created for the evacuation of the larger fragments. A specimen bottle could be added between the sheath and the suction device to facilitate stone fragment collection. (Supplementary Videos S1 and S2; Supplementary Data are available online at
After the procedure, a Double-J stent was placed and it was removed 3 to 7 days later. Patients were generally discharged home on the first postoperative day. Patients were routinely followed in 1 month with a kidney, ureter, and bladder radiograph (KUB). Stone-free status (SFS) was assessed both visually and fluoroscopically at the end of the procedure and with KUB on the first postoperative day. SFS was defined as no stone fragment evident visually, on the fluoroscopy, and on the KUB.
Data collected included patients' and stones' characteristics, operative time, failure of sheath insertion rate, and complications. Operative time was measured from the time of insertion of mUAS to the completion of lithotripsy. Stone surface area was calculated using the formula: length × width × π × 0.25. Sum was used for multiple stones. Statistical analyses were performed using means, ranges, and percentages.
Results
One hundred four patients with ureteral stones or Steinstrasse were accrued into this study. There were 52 upper, 19 middle, and 32 lower ureteral stones for a total of 103 stones in 91 patients. Two patients had bilateral ureteral stones. In addition, 13 patients had Steinstrasse. Seventy-four patients, 43 males and 31 females, had effective sheath placement, giving a success rate of 77.1%. This included 35 upper, 14 middle, and 16 lower ureteral stones in 63 patients and 11 Steinstrasse. The success rate for sheath insertion was 64.2% for males and 83.8% for females. Patients who failed mUAS either underwent ureteroscopic laser lithotripsy without access sheath or had Double-J stent placed for passive ureteral dilation. These patients were not analyzed further. Patients' demographics and stone characteristics are shown in Table 1.
mUAS = modification to the standard UAS; PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
The mean operative time was 27.3 minutes. Sixty-seven patients had properly placed mUAS and underwent semirigid ureteroscopic laser lithotripsy. All these patients had the stones completely removed with no observed stone retropulsion. Seven patients failed semirigid ureteroscopy. Five failures were caused by an inability to reach the stone with the scope (the sheath and the scope were too short), and two were caused by an excessive kink of ureter just below the impacted stone. These seven patients were converted to flexible ureteroscopy. They all had some degree of retropulsion. Five patients had adjunctive basket extraction to render them stone free.
The immediate postoperative stone-free rate (SFR) was 97.3%. SFR after 1 month was 100%. Complications were few. Two patients had fevers, which resolved with conservative therapy. One patient had a false passage at the distal ureter. The false passage was recognized, the true lumen was identified, and the procedure completed. This patient had the Double-J stent left in place for 4 weeks. Due to the financial considerations, only 15 patients chose to have their stone analyzed. Calcium oxalate was the most common stone composition. Operative parameters are shown in Table 2.
Discussion
Ureteral stone is a common condition encountered in the urologic practice. When intervention is indicated, ureteroscopic laser lithotripsy is the preferred treatment. This procedure is highly effective for both adults and children with minimum morbidity. The success rate has been reported from 80% to 97%. 5 –9 Most of the SFRs reported were not immediate SFRs, but the SFRs at the 30 days or more follow-up.
Currently there are two techniques for the ureteroscopic laser lithotripsy. 2 The first technique is to break up the stone into smaller fragments and remove the fragments using a stone basket or forceps. The second technique is to pulverize the stone into tiny fragments and allow the patient to pass the fragments during the postoperative period. Some surgeons prefer to use a combination of the two techniques. The former technique has a higher immediate SFR, but the disadvantage of needing to repeatedly pass the ureteroscope and the auxiliary instruments in and out of the ureter. This can increase the risk of ureteral injury. UAS is often used to reduce the potential of injury. The latter technique depends on the patient to spontaneously pass the stone fragments. It may not always be effective, may cause significant interim ureteral colic, and may result in Steinstrasse. Currently there is no effective technique to treat the Steinstrasse.
There are other shortcomings as well. Retropulsion of the ureteral stone, especially the upper ureteral stone, back into the kidney is a major concern. It was reported to occur in as much as 40%. 10 –12 Other issues include high intraluminal pressure caused by the irrigation fluid and potential for ureteral injury when visualization is compromised. Many devices are currently on the market to prevent the retropulsion. These devices either take the form of a back stop 14,15 or a self-dissolvable gel 16 that traps the stone fragments. All these devices have a few common flaws. They have to be placed above the stone and have to be removed with trapped stone fragments in place. The back stops also have an attached wire that could reduce the space within the ureteral lumen.
We modified the standard UAS by applying the similar principles used in the continuous flow resectoscope and the common suction device to address the deficiencies in the ureteroscopic lithotripsy. We added an oblique conduit through a handle to a straight UAS that was then connected to a negative pressure aspirator to allow active egress of irrigation fluid and stone fragments. We also put a pressure regulating vent in the form of a slit on this oblique sluice to allow adjustment of the suction pressure. In an in vitro experiment, we noted that this irrigation-suction scheme created a vortex extending only about 1 to 2 cm. No pressure was transmitted beyond that point. Furthermore, with the continuous suction, the shattered stones tended to aggregate at the opening of the mUAS.
The tiny fragments would simply pass around the ureteroscope and exit through the oblique sluice. The fragments that were too big to pass between the sheath and the scope could be evacuated by our novel technique: first, increasing the negative pressure by occluding the pressure vent, and second, withdrawing the scope to just proximal to the bifurcation of the mUAS to open up unobstructed egress channel. There are some important features of our mUAS that should be noted.
First, the mechanical requirements: The lumens of the oblique conduit, as well as the tubing connected to the aspirator, have to be the same size or larger than the distal segment of the sheath to allow for unimpeded passage of stone fragments. The handle should be constructed of transparent materials so that the stone fragments can be seen coming through the side branch and so that the scope can be seen when it is withdrawn proximally to the bifurcation. There needs to be an adequately-sized irrigation channel in the ureteroscope to allow for sufficient flow of irrigation fluid at 60 to 80 cc per minute, which will create the vortex and enhance the active egress of stone fragments.
Second, the techniques: The scope should be withdrawn slowly to allow the stone fragments to follow the scope to the oblique sluice. Both the negative pressure aspirator and the pressurized irrigation should be set on the continuous mode to be effective.
Finally, this device is placed distal to the stone and the use of suction evacuation has the advantage of removing all the stone fragments without the need of stone basket or forceps.
We are pleased with our initial results. We had only seven patients that failed the semirigid ureteroscopic lithotripsy. These failures were either caused by the length of the scope or a severe kink in the ureter. However, since the mUAS was already in place, these patients could be easily converted to flexible ureteroscopy and were able to complete the intended surgery. We achieved 97.3% immediate SFR and 100% SFR in 1 month in all the patients, including those with Steinstrasse, with the minimum use of stone basket.
We also identified other advantages. Using the continuous suction and irrigation throughout the procedure, the field of vision was clearer; the dust storm caused by laser pulverization of the stone and the minor bleeding from the ureteral mucosa would no longer cloud the vision. Based on our in vitro experiment, we believe the intraluminal pressure in our technique should be lower than the other ureteroscopic laser lithotripsy procedures. It should therefore improve the safety of the surgery. Our device required no additional training and no other special equipment.
The main objective of this report is to present a novel concept and technique for a mUAS and laser lithotripsy. There are some deficiencies in this study. We have a relatively short follow-up; therefore, we do not know if any of our patients developed ureteral stricture secondary to the mUAS. However, based on the historical data, 17 –19 this should not be a significant issue. This is not a prospective and randomized study; thus it cannot be a fair comparison to the current techniques or the UAS.
Conclusion
We made a simple modification to the common UAS and developed a novel technique for its use. Our device appeared to provide safe and effective treatment for the majority of the ureteral stones, as well as the Steinstrasse (Supplementary Videos S1 and S3). It likely reduced the risk of retropulsion of the stone fragments and improved the immediate SFR. With the continuous irrigation and aspiration, we also noticed clearer visualization throughout the procedure and possibly significantly reduced the intraluminal pressure. The mUAS has a minimal learning curve. Other than the sheath, there is no special equipment required. We are encouraged by our results and intend to routinely use this device.
Footnotes
Acknowledgment
This research was supported by the Well Lead Medical Co. Ltd., Guangzhou, Guangdong, China.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.