
Abstract
Background:
Because minimally invasive surgery can improve postoperative recovery, it became the preferred technique for patients with significant comorbidities. However, steep Trendelenburg position and abdominal CO2-insufflation can lead to a significant increase in upper airway resistance and an alteration of overall lung function. In particular, patients who already suffer from an obstructive airway disease like obstructive sleep apnea syndrome (OSAS) might be at risk for postoperative airway complications. Therefore, we perioperatively performed spirometric tests in patients with OSAS undergoing robotic surgery in steep Trendelenburg position.
Methods:
Twenty patients with OSAS were enrolled in the study. A day before surgery lung function measurements were performed and repeated preoperatively, 40, 120, and 240 minutes and 1 and 5 days postoperatively. We measured vital capacity (VC), forced expiratory volume in 1 second (FEV1), maximal mid expiratory and inspiratory flow (MEF50, MIF50), arterial oxygen saturation, and nasal flow.
Results:
The ratio of MEF50 to MIF50, as an indicator of upper airway resistance, was increased significantly postoperatively and normalized within 24 hours (p < 0.0001), while FEV1 and VC were significantly reduced and recovered only partially as much as the fifth postoperative day (p < 0.0001).
Conclusion:
Airway resistance increased following robotic radical prostatectomy in Trendelenburg position in patients with OSAS. Two separate major effects can be observed. A significant increase of the upper airway resistance, which improved to preoperative conditions within 24 hours, and a reduction in FEV1 and VC, which recovered only partially as much as the fifth postoperative day.
Introduction
R
Based on these reports the question arises, how patients who already suffer from an obstructive airway disease like obstructive sleep apnea syndrome (OSAS) might be at risk for postoperative airway complications. 6 –8 OSAS has become a disease of epidemic character with an assumed high rate of undiagnosed patients and an increased risk of postoperative pulmonary complications and oxygen desaturation. 6,9 –13
To assess the effect of the extreme conditions during surgery on lung function and airway resistance in patients with OSAS, we perioperatively performed spirometric tests to assess upper airway resistance and possible alteration in vital capacity (VC) and the forced expiratory volume in 1 second (FEV1) in patients with OSAS undergoing robotic surgery. With particular interest in the upper airway the primary hypothesis was formulated that there was no change in the ratio of maximal mid expiratory flow (MEF50) over maximal mid inspiratory flow (MIF50) postoperatively compared to baseline.
Methods
Patients
After approval by the local ethics committee (Chamber of Physicians of Nordrhein, Düsseldorf, Germany; Registration-Number 2012306), 20 patients with OSAS were enrolled in this study. No patient had to be excluded from the analysis (Consort flow diagram, Fig. 1).
Consort diagram for the enrolment and analysis of the study population.
All patients were scheduled for robot-assisted radical prostatectomy and lymph node dissection and gave their informed written consent to participate in this study. All of the patients with OSAS had been diagnosed of OSAS, and in all patients OSAS has been confirmed by polysomnography testing before surgery. Eighteen out of twenty patients were using noninvasive ventilator support during sleep before surgery and during the nights after surgery.
Measurements
Lung function measurements were performed with a spirometer (pneumotachograph; VIASIS, Würzburg, Germany). Baseline lung function measurements were done 1 or 2 days before surgery in sitting position according to the recommendations of the American Thoracic Society and European Respiratory Society. 14
VC, FEV1, maximal expiratory flow at 50% of the VC (MEF50), and maximal inspiratory flow at 50% of the VC (MIF50) were analyzed. Besides these standard spirometric measurements, nasal flow and arterial oxygen saturation (without supplemental oxygen) were assessed. 15 –17
On the day of surgery and on all subsequent measurements, measurements were performed in supine position with the upper body tilted upwards by 40°. According to international guidelines, always the best of three measurements was accepted for analysis. 14
Protocol
On the day of surgery measurements were performed in supine position before the patients were brought into the induction room. Subsequently, in the induction room a peripheral intravenous line was placed, electrocardiogram electrodes were placed, noninvasive blood pressure measurement was started, and a finger tip for arterial oxygen saturation was applied. All patients received a low-thoracic epidural catheter at T9/10 or T10/11 thoracic vertebral interspace with loss of resistance technique.
During surgery the epidural catheter was used and dosed with 0.375% bupivacaine. After the placement of the epidural catheter general anesthesia was induced with propofol, remifentanil, and mivacurium. The dose of the agents was administered according to the discretion of the attending anesthesiologist. Mechanical ventilation was initiated with a tidal volume of 6–8 mL/kg ideal body weight and an end-expiratory pressure of 7 cm H2O and further on adjusted to achieve normoventilation (end-expiratory CO2 of <38 mm Hg). During robotic surgery patients were positioned in a steep Trendelenburg position of 40° head down.
Intravenous fluid administration was limited to 2000 mL of crystalloid solution until the urethral anastomosis was completed. Thereafter, fluid infusion was increased to stimulate postoperative diuresis and stabilize arterial blood pressure.
Because all patients had received an epidural catheter that was dosed with a high concentration of bupivacaine, no additional doses of systemic muscle relaxing agents were administered. Still, the train of four was controlled at the end of surgery, and the patients were extubated when the train of four showed a recovery to more than 95% from baseline.
Forty minutes after extubation, the first lung function and nasal flow measurements were performed. Subsequently, measurements were repeated after 120 and 240 minutes and on the first and fifth postoperative day. Before the lung function measurements, pain score (Numerical Rating Score, with 0 for no pain and 10 for worst imaginable pain) was assessed. Forty minutes after surgery the presence of chemosis was assessed and scored as 0 for no sign and 1 for presence of chemosis according to the ophthalmic score with 0 for score grade 1 and 2 and 1 for score grade 3 and 4. 18
Furthermore, characteristics of the patients and their disease, as well as duration of surgery, estimated blood loss (EBL), perioperative complications, intravenous fluid administration, and days of hospitalization, were assessed.
Data analysis
Sample size calculation was based on the primary hypothesis that there is no significant difference in the ratio of MEF50/MIF50 when pre- and postoperative measurements were compared, with a difference to detect of minimal 0.10, an α error of 0.05, a β error of 0.8, and standard deviation of 0.15. The result was a minimal number of 19 patients. We rounded the number to 20.
Patients' characteristics and disease stage were compared to our whole patient population, who underwent robot-assisted radical prostatectomy (n = 1914).
Secondary hypotheses
First, hypothesis was that there is no difference in VC when pre- and postoperative measurements were compared.
Second, hypothesis was that there is no difference in FEV1 when pre- and postoperative measurements were compared.
Third, hypothesis was that there is no difference in nasal flow when pre- and postoperative values were compared.
In addition, in an explorative approach, correlations between extend of chemosis and change in the ratio of MEF50/MIF50 were tested. The same correlations were calculated for nasal flow.
The primary hypothesis was tested by analysis of variance for repeated measurements followed by a post hoc test with Bonferroni correction for multiple testing. Null hypotheses were rejected and significant differences assumed with p < 0.05. Data are presented as mean confidence interval (CI).
Results
Characteristics of the patients
Detailed characteristics of each patient and his disease (tumor lymph nodes metastasis [TNM] status, Gleason score, and prostate specific antigen [PSA] values) are presented in Table 1. Duration of surgery, EBL, amount of intravenous fluids, chemosis formation, perioperative complications, and days of hospitalization are presented in Table 2.
Age, weight, height, body mass index (BMI), PSA, TNM status, Gleason score, comorbidities besides OSAS, apnoe-hypopnoe index (AHI), FEV1 (in percent of the predicted values), and VC (in percent of the predicted values) (mean; 95% confidence interval, CI) are presented in Table 1.
N = results of regional lymph node dissection: 0 = no lymph node metastasis, 1 = lymph node metastasis, X = no lymph nodes assessed.
AV-Bl = av node block; Art. hyper. = arterial hypertension; Atr. fib. = atrial fibrillation; CAD = coronary artery disease; FEV1 = forced expiratory volume in 1 second; NIDDM = noninsulin dependent diabetes mellitus; OSAS = obstructive sleep apnea syndrome; Park. = Parkinson's disease; PE = pulmonary embolism; PM = pacemaker; PSA = prostate specific antigen; TNM = tumor lymph nodes metastasis; VC = vital capacity.
Duration of surgery, EBL, intravenous fluids, chemosis, hospitalization, and complications are presented in Table 2.
Anast. leak = anastomosis leak; EBL = estimated blood loss; paralyt. ileus = paralytic ileus; y/n = yes/no.
Primary outcome measure
As the primary outcome measurement the ratio of MEF50 divided by MIF50 was assessed. There was a significant difference over time (p < 0.0001; Fig. 2). The ratio improved over the first 4 hours and returned to baseline after 24 hours (Fig. 2).
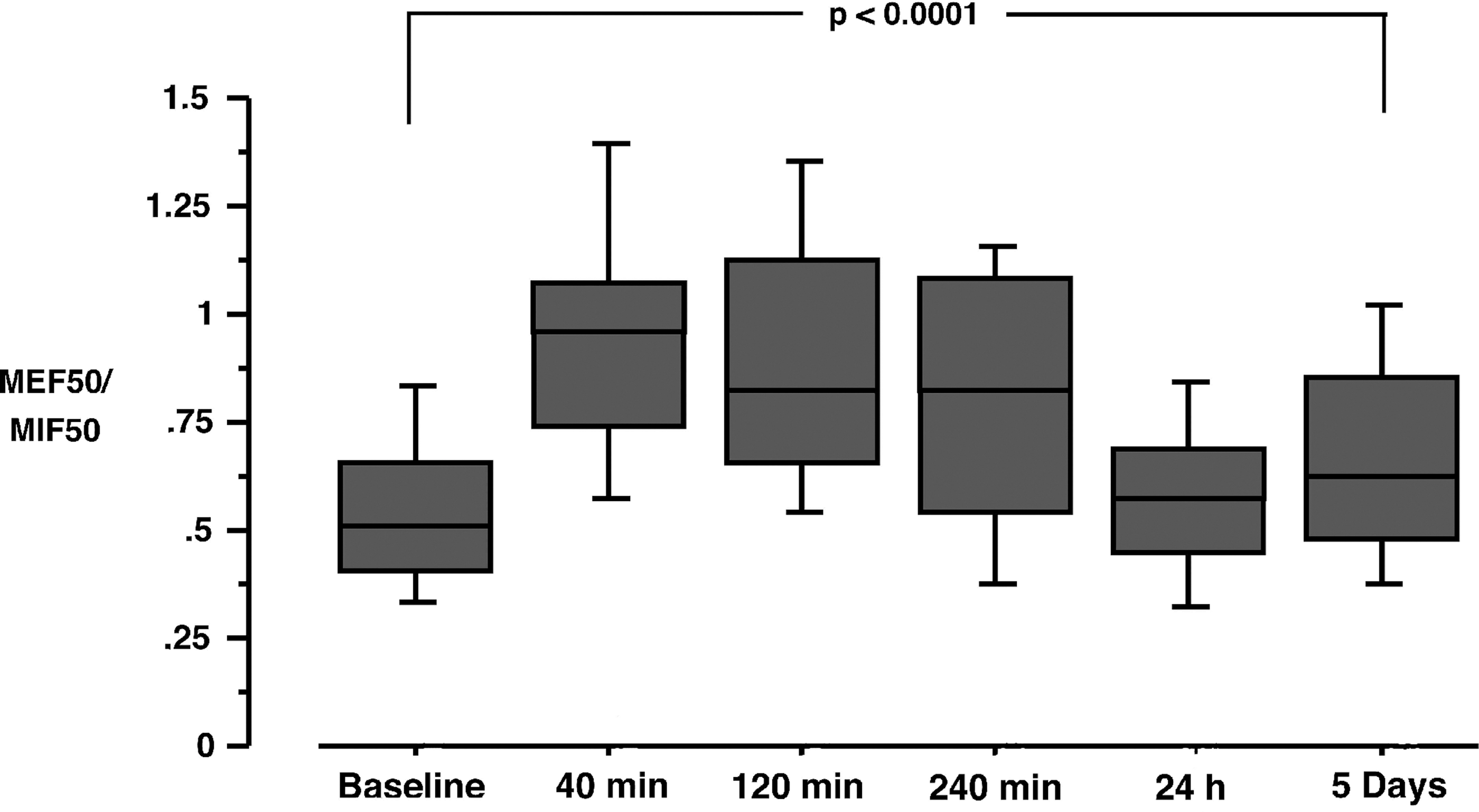
Box plot of the perioperative MEF50/MIF50 ratio. Boxes represent the measurements of 20 patients with obstructive sleep apnea syndrome. The MEF50/MIF50 ratio is a measure of upper airway resistance, increased significantly after surgery and returned to baseline within 24 hours. MEF50 = maximal mid expiratory flow; MIF50 = maximal mid inspiratory flow.
Secondary outcome measures
VC and FEV1 changed significantly with change in posture from sitting to supine (p = 0.0011 and p = 0.0192). Postoperatively, VC and FEV1 decreased significantly with a nadir at 24 hours (p < 0.0001; Fig. 3). Although not statistically significant with respect to repeated measurements, VC and FEV1 were still reduced at the fifth day by 8% (VC) and 6% (FEV1), respectively.

Box plot of the VC (dark gray) and the FEV1 (light gray) of 20 patients with obstructive sleep apnea syndrome. VC and FEV1 were significantly reduced postoperatively. Following early improvements within the first hours and a nadir after 24 hours, VC and FEV1 improved to more than 90% of baseline as much as the fifth postoperative day. VC = vital capacity; FEV1 = forced expiratory volume in 1 second.
Nasal flow was significantly decreased after surgery and improved within 24 hours (p < 0.0007; Fig. 4). There was a trend of reduction in nasal flow with the occurrence of chemosis directly after surgery.
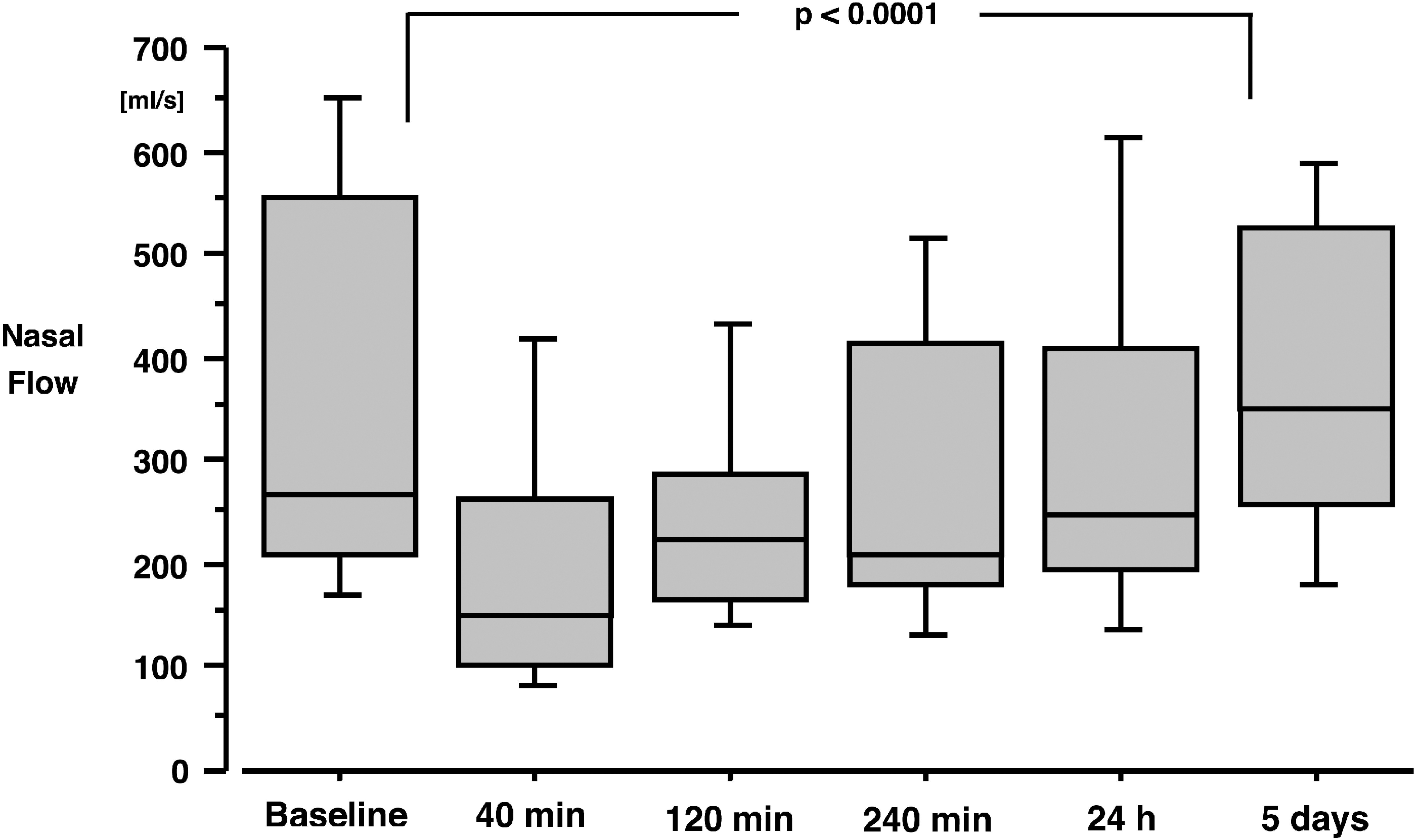
Box plot of the nasal flow of 20 patients with obstructive sleep apnea syndrome. Nasal flow, as an indicator of the most upper part of the airway, was significantly reduced following surgery, improved after 4 hours postoperatively, and returned to baseline within 5 days.
Pain score
Pain level of the patients was evaluated before each lung function measurement. In two patients additional pain medicine had to be administered to achieve a pain score of 2 or less.
Oxygen saturation
At the beginning of the measurements before forced respiratory maneuvers, the arterial oxygen saturation was measured. The oxygen saturation decreased significantly from baseline 96% (CI 95, 97) to postoperatively 93% (CI 92, 94; p < 0.0001) with the lowest values directly after surgery. Oxygen saturation was still reduced after 24 hours (94%; CI 93, 95) and recovered to baseline after 5 days.
Chemosis and fluid administration
Chemosis was described in 13 out of 20 patients. Chemosis resolved in all patients within 24 hours postsurgery. Although a trend toward higher MEF50/MIF50 ratio and lower nasal flow for patients with chemosis was observed, there was no significant difference between patients with or without chemosis. During the total duration of surgery, patients received 2355 mL (CI 2141, 2569) of crystalloid solution intravenously (Table 2).
Discussion
In patients with OSAS steep Trendelenburg position for robot-assisted prostatectomy resulted in an increase of upper airway resistance and a decrease of nasal flow. These changes improved over 4 hours and resolved to baseline within 1 day, while VC and FEV1 were significantly reduced with a nadir at 24 hours and an improvement over the following days with still some residual reduction of the capacity present after 5 days.
The American Society of Anesthesiologists (ASA) practice guidelines for the perioperative care of patients with OSAS state that most of their recommendations are not based on scientific evidence, but on expert opinion. 9,11 Key points of these recommendations are the avoidance of perioperative administration of opioids, benzodiazepines, and the limitation of muscle relaxant drugs. Furthermore, the use of epidural anesthesia and the control of the full recovery from muscle relaxation are recommended. 9,11,19,20 In accordance with these recommendations, we did not use benzodiazepines as a premedication and used epidural anesthesia in each of the patients to avoid intraoperative muscle relaxant agents and the administration of opioids for postoperative analgesia. However, the effects of extreme head down positioning and CO2-insufflation on patients with OSAS are unknown and might lead to relevant aggravation of their upper airway obstruction as implied by several reports of postoperative hypoxemic events in patients with OSAS. 6,9,10
In a previous study in patients free of pulmonary and upper airway disease, as well as patients with COPD, we evaluated the effect of these perioperative conditions on lung function and upper airway resistance. 5 We could demonstrate an increase in upper airway resistance with the resolution within 1 day and residual effects on pulmonary function in patients with COPD. Nevertheless, because of the fast recovery of the patients following minimally invasive robotic surgery and the same reduction in pulmonary function following open surgery, robotic surgery seems still to be a preferable technique. Because fast recovery with early mobilization is also desirable in patients with OSAS, this surgical technique might be also important for OSAS patients.
To evaluate the effect of the extreme intraoperative conditions, we performed measurements of upper airway resistance and pulmonary function. We measured the ratio of MEF50/MIF50 as an indicator of extra thoracic airways, nasal flow as the upper most part of the airways, and assessed VC and FEV1 as representative parameters of pulmonary function and intrathoracic airway resistance. 10,15 –17,21
There have been several studies of postoperative lung function describing minor decreases of VC and FEV1 after open lower abdominal surgery within the range of our results. 22,23 In particular the occurrence of a nadir at 24 hours has been observed before. 24,25 While in our previous study patients, free of pulmonary disease, regained their baseline VC and FEV1 within 5 days, we still have a reduction in OSAS patients, similar to effects in patients with COPD, for more than 5 days, which might be due to the significant reduction of lung compliance following robot-assisted prostatectomies. 26,27
Because we were concerned about the early postoperative effects on the upper airway in patients with OSAS, we prolonged our observation on the first day for 4 hours postoperatively. Although positioning of the patients in a 40° head up position directly after surgery for 4 hours, we still found a significant increased upper airway resistance, but with a constant improvement over this time period and no subjective dyspnea after 4 hours.
Hence this effect also occurred in control patients; this development seems to be independent of preexisting pulmonary disease and OSAS and shows some correlation with the expression of chemosis and intraoperative fluid management. In patients with OSAS, we could find a tendency of a relationship between increased MEF50/MIF50 ratio and a decreased nasal flow with the occurrence of chemosis, but it missed statistical significance.
Studies on early postoperative lung function can be influenced and limited by several factors. Lung function measurements depend on the vigilance and ability to perform the tests, that is, reduced vigilance, residual muscle relaxation, and pain that can alter the results. 28,29
First, based on our previous studies and several studies on the same topic, we felt confident that patients, who were able to follow commands after extubation will be able to perform lung function maneuvers 40 minutes later. 5,28,30 All patients received a combination of general and thoracic epidural anesthesia and received no systemic muscle relaxation after the initial dose of a short acting muscle relaxant for tracheal intubation. To exclude any prolonged effects of this initial dose, we tested muscle activity by acceleromanometry at the end of surgery and found a train of four with an average percentage of 99%.
Third, concerning the effect of postoperative pain on lung function measurements, the measurements were performed when the patients described their pain with a pain score of <3 on a numeric rating scale following a deep breath.
Fourth, patients with OSAS might differ from the complete population of patients undergoing robot-assisted radical prostatectomy. Therefore, we statistically compared the disease stage (Gleason score, TNM status, and PSA values) of these patients with our complete database of patients (n = 1914) and found no difference. Furthermore, it could be hypothesized that in patients with OSAS duration of surgery and/or EBL would be different because of the habitus of the patients, but again there was no statistical difference to be found. To exclude the possible influence of an absence in experience, anesthesia was always provided by anesthesiologists experienced in these procedures at the level of a fully boarded anesthesiologist.
In conclusion, in patients with OSAS, who underwent robot-assisted prostatectomy in steep Trendelenburg position, we found an increase of upper airway resistance directly after surgery that improved over the initial 4 hours and resolved after 24 hours. Moreover, a significant reduction of VC and FEV1 was found and still detectable after 5 days. Overall, despite the advantages of minimally invasive surgery, alterations of upper airway resistance and lung function occur and deserve attention during the postoperative care.
Funding
The study was financed by departmental resources. No external funding exists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.