
Abstract
Introduction:
The American Urological Association (AUA) guidelines state that continuing anticoagulation and antiplatelet agents in routine ureteroscopy (URS) is safe and without increased risk of complications. However, these recommendations are based on small case series; thus, we sought to analyze bleeding-related complications among patients on antiplatelet therapy (APT).
Materials and Methods:
Overall, 4799 URS procedures performed at our institution between June 2009 and February 2016 were identified. Records were then retrospectively reviewed to confirm APT use and to identify periprocedural complications. Antiplatelet agents evaluated included aspirin (low dose and full dose) and P2Y12 receptor antagonists (clopidogrel, prasugugrel, ticagrelor). Patients were excluded if they were taking a concurrent anticoagulant agent or if additional non-URS procedures were performed.
Results:
Of 4799 URS procedures, 314 (6.5%) were performed on patients taking APT, of which 234 (74.5%) held APT, 63 (20.1%) continued APT, and 17 (5.4%) continued dual APT. The mean age was 70.1 years, and the majority of patients (69.6%) underwent a stone procedure with a stone-free rate of 80.2%. The overall bleeding-related complication rate was 1.9%, whereas the significant bleeding-related event rate was 1.6% and this did not differ among the groups (p = 0.3). The power to detect a 3% difference in bleeding between the groups was 0.95.
Conclusions:
Continuing APT in patients on chronic therapy does not appear to pose an increased risk of bleeding-related complications. Our findings support the current AUA guidelines as they relate to APT.
Introduction
T
In 2014, the American Urological Association (AUA) and the International Consultation on Urological Diseases (ICUD) issued guidelines regarding the use of anticoagulation and APT in urologic practice, stating, “URS can be performed with continuing oral anticoagulation and antiplatelet therapy.” 4 The body of evidence to support this guideline was based on a systemic review of three studies comprising less than 100 total patients on either APT or anticoagulation therapy. 4 –8 As the complication rate for URS is low, historically reported as less than 1%, 6,9 these small studies may be underpowered to detect adverse effects of performing URS in patients on APT. 4 –8 We, therefore, sought to evaluate the impact of APT on bleeding outcomes after URS.
Materials and Methods
After Institutional Review Board approval, we identified 4799 URS procedures performed between June 2009 and February 2016 at our institution. Anticoagulation or APT use was documented within 90 days of the procedure in 528 patients (Fig. 1). APT agents included were aspirin 81 mg, aspirin 325 mg, and P2Y12 receptor antagonists (clopidogrel, prasugugrel, ticagrelor). After chart review, 129 were excluded for concomitant non-URS procedures or no documentation of anticoagulation/APT. We excluded 85 patients for use of an anticoagulation agent (enoxaparin, warfarin, and non-vitamin K oral antagonists such as rivaroxabin). Of note, patients who had attempted URS with an inability to access the stone or proximal ureter with the need for presenting and returning to operating room (OR) for subsequent URS at a later date were included. This left us with a final cohort of 314 procedures performed with patients taking chronic APT without concurrent anticoagulation therapy.

Consort diagram of 4799 ureteroscopies performed between June 2009 and February 2016.
Additional clinical characteristics collected included age, gender, body mass index, Charlson comorbidity index (CCI), and American Society of Anesthesiologists (ASA) classification at the time of the procedure. Procedure information, including operative time, stone size, location, and stent status, was obtained.
Patients were then divided into three groups for analysis: Group I: held APT, Group II: continued single-agent APT, and Group III: continued dual APT. All patients had a preoperative anesthetic evaluation where APT management was addressed. If APT was held for the URS procedure, patients were usually instructed to restart APT once hematuria resolved, although this recommendation was not standardized in our practice.
Complications, including readmissions and emergency department (ED) visits within 30 days of the procedure, were identified by review of the medical record. The following were considered significant bleeding-related complications: (1) procedure termination explicitly due to bleeding and difficult visualization resulting in a second operative intervention; (2) unplanned, immediate postoperative admission for bleeding; (3) ED visit for hematuria; (4) subsequent hospital admission for hematuria management * ; and (5) unplanned return to the OR for evaluation of ongoing bleeding. Patient phone calls related to hematuria were also recorded and included in the overall bleeding-related event rate, but they were not considered significant complications. Finally, all-cause hospital readmissions within 30 days of the procedure were also recorded.
All procedures are performed under a general anesthetic. The use of paralytic agents is at the discretion of the surgeon and typically depends on the size and location of stone burden. It is most commonly used when there is a large volume of distal ureteral stone requiring lithotripsy. Multiple surgeons performed URS using standard techniques. All flexible URS was performed using 7.5F Karl Storz™ 11278 AUA1 Flex-X™, 8.7F ACMI™ DUR-8 Elite, 6.9F Olympus™ URF-P3, or Wolf™ 7325.071 Viper flexible ureteroscopes. Semi-rigid ureteroscopy for distal ureteral stones was performed using Gyrus ACMI™ MR6 or Wolf™ 8702.518 ureteroscopes. For diagnostic procedures, selective cytology, brush biopsy, and tissue biopsy were obtained using either the 3F Boston Scientific™ Piranha biopsy forceps or 2.4F Cook™ BIGopsy ® forceps. In our practice, an access sheath with pressurized irrigant was used when performing flexible ureteroscopy and all stone fragments greater than 1 mm were removed using a 1.9F nitinol basket. If the ureter was too tight to allow access sheath placement, ureteral dilatation with sequential dilators was performed. Holmium:YAG laser lithotripsy was performed using a 200 μm laser fiber set at 0.8 J and 8 Hertz for stones and 1.2 J and 8 Hertz for fulguration of lesions.
Patients returned 4–6 weeks after the procedure with a plain abdominal x-ray (KUB) and a renal ultrasound to evaluate for early stricture and to rule out significant retained fragments. Stone free was defined as stone clearance in a single procedure with no identifiable fragments on postoperative imaging.
Continuous variables were summarized with medians/interquartile ranges and compared using t-test or ANOVA. Categorical variables were summarized using frequencies/percentages and were compared using Fisher's exact test and chi-square tests. A power calculation for equivalence between groups and an analysis for possible confounders were performed. All tests were two sided, with p ≤ 0.05 considered statistically significant. Statistical analysis was performed using SPSS software package (V.22 IBM: Aramonk, NY).
Results
Of 4799 URS between June 2009 and February 2016, 314 (6.5%) were performed on APT. In this group, 234 (74.5%) held APT, 63 (20.1%) continued single APT, and 17 (5.4%) continued dual APT. Clinical features, stratified by APT status, are presented in Table 1. The mean age at the time of the procedure was 70.1 years, and the majority of patients were men (73.2%). More than two-thirds (69.6%) of patients underwent URS for stone treatment, whereas 30.4% underwent diagnostic URS.
Means compared using ANOVA, proportions with Pearson chi-square.
ASA = American Society of Anesthesiologists; CCI = Charlson comorbidity index.
At the time of surgery, patients who continued APT were more likely to undergo a stone procedure and had a smaller stone burden. Specifically, patients who continued single or dual APT underwent stone removal 84.1% and 94.1% of the time, respectively, compared with only 63.9% of those who held antiplatelet therapy (p = 0.001). Total stone size was the smallest in those who continued on dual APT at 7.2 mm compared with 8.1 mm for those who continued on single APT and 10.6 mm for those who held APT. The overall stone-free rate was 80.2%. Age, gender, CCI, and operative time did not differ between the groups.
Perioperative complications were stratified by APT (Fig. 2). The overall bleeding-related complication rate was 1.9% (6/314), whereas the significant bleeding-related event rate was 1.6% (5/314). No patient required a blood transfusion. Bleeding-related events did not differ significantly between the groups (p = 0.3). However, patients who were on dual APT were more likely to be readmitted to the hospital for any reason in the 30 days after URS compared with those who held APT or were on single APT (12% vs 0%, p ≤ 0.001).
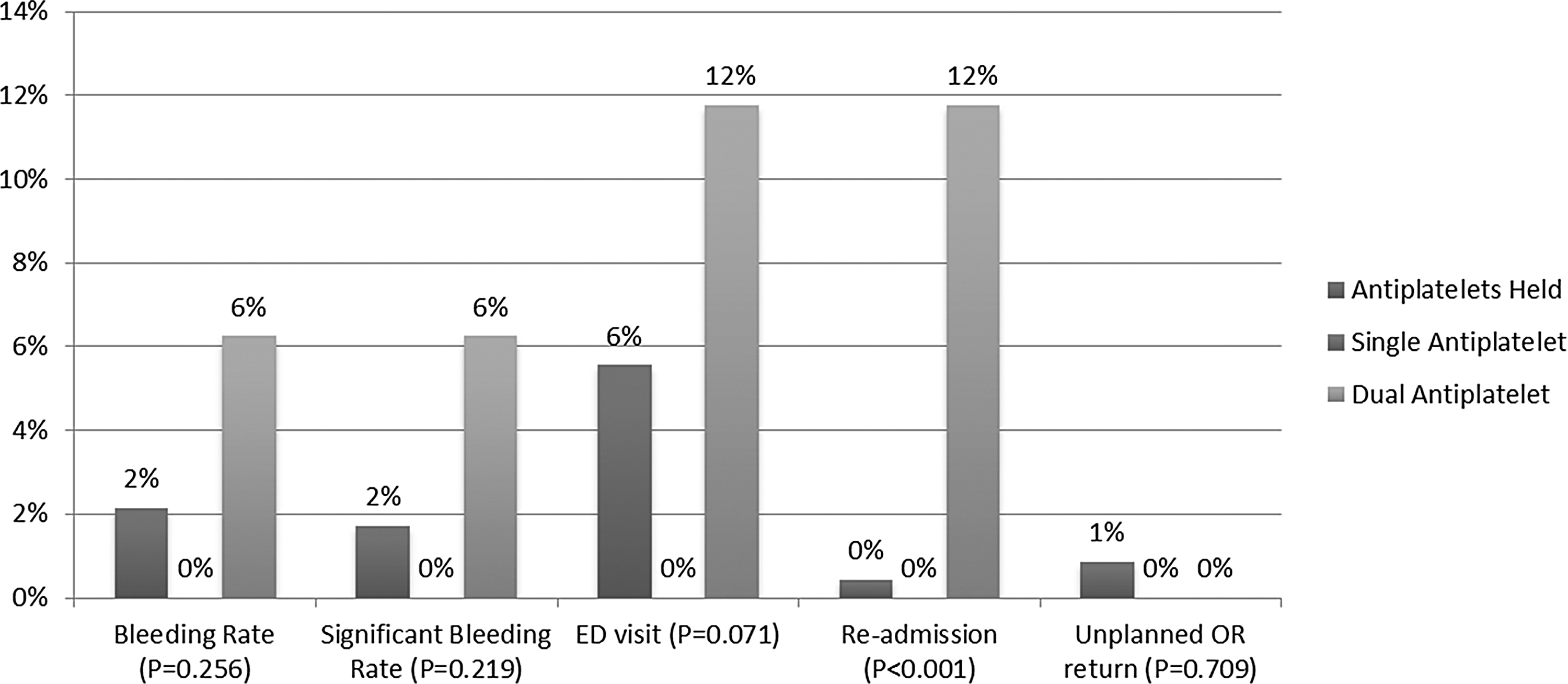
Comparison of complication rates based on number of antiplatelet agents.
Specific antiplatelet agents continued are shown in Table 2. Complications were then compared by type of APT used (Fig. 3). No intraoperative complications such as ureteral perforation were recorded. Patients who continued P2Y12 receptor antagonists, with or without aspirin, were the most likely to be readmitted to the hospital within 30 days of the procedure (p < 0.001). Two of the three patients readmitted had fever and/or bacteremia, whereas the third patient had abdominal pain, nausea, and vomiting. Again, there was no difference in overall or significant bleeding-related events between the groups (p = 0.6 and p = 0.5, respectively). Among those who held APT, no adverse effects were identified within 30 days of the procedure.
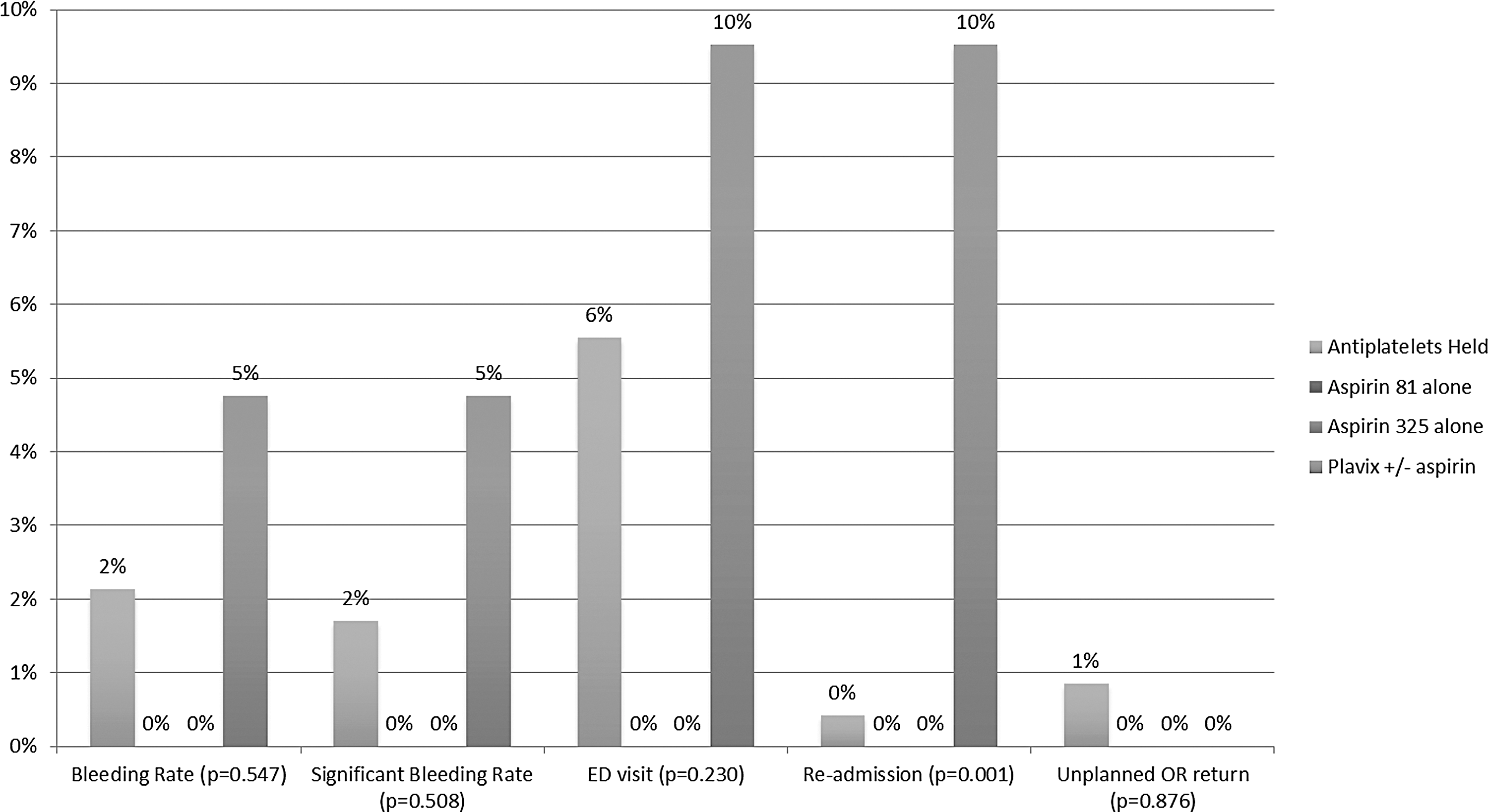
Complication rate by type of antiplatelet agent continued at time of ureteroscopy.
Interestingly, 8.1% (8/91) of patients who were on P2Y12 receptor antagonists at the time of their initial urologic consultation had the medication permanently discontinued after preoperative medical evaluation due to unnecessary use. Likewise, 8.6% (27/314) of patients had self-started a full-dose aspirin for prophylaxis. These patients also had their APT permanently discontinued or were recommended to resume a baby aspirin only after their procedure.
Given the low event rate, regression analysis could not be performed. Therefore, we analyzed additional co-variates (i.e., stone size, stent placement before procedure, CCI, operative time) that may have confounded our results (not shown). None of the potential confounders differed significantly between patients who did and those who did not experience specific complications.
Finally, we performed a power calculation for equivalence between the held APT and continued APT groups (234 vs 80 patients). Our power to detect a 3% difference in bleeding between the groups was 0.95. To detect a 2% and 1% difference in bleeding rates, our power was 0.71 and 0.30, respectively.
Discussion
We examined the outcomes of patients on APT undergoing URS. Patients who continued single or dual APT therapy were more likely to undergo a stone procedure and tended to have a smaller overall stone burden. Perhaps most notably, there was no difference in bleeding-related complications between groups, although those on dual APT were more likely to be readmitted to the hospital within 30 days of their procedure compared with those on single APT or those holding APT altogether. Finally, nearly 10% of patients on chronic APT were found to not need the medication and it was discontinued at the time of their preoperative medical evaluation.
Our significant bleeding-related complication rate of 1.6% is slightly higher than the overall complication rate for URS, which is historically reported as less than 1%. 6,9 However, recently, Giusti et al. noted a 29% complication rate among 314 patients undergoing URS between 2014 and 2015, 10 although only 2.2% were Clavien grade III or IV and none was attributed to bleeding. 10 In addition, Daels et al. analyzed URS outcomes among nearly 12,000 patients worldwide and found that postoperative bleeding was higher in patients who were on anticoagulation (including aspirin) compared with those who were not (1.1% vs 0.4%; p < 0.01). 11
Historically, APT has been discontinued before endoscopic urologic surgery; 5 however, current AUA/ICUD guidelines state that perioperative use of APT is safe and does not pose additional bleeding risks. 4 The AUA/ICUD recommendations are based on retrospective series combining multiple medication classes. 5 –8 Unlike previous studies combining multiple antithrombotic classes, in our study, we examined only those on APT, excluding all patients on concurrent anticoagulation. For example, in a retrospective matched-pair analysis of 692 patients, Turna et al. identified 37 patients (5.2%) on chronic antithrombotics (warfarin, clopidogrel, and aspirin). 7 They found no difference in intraoperative or postoperative complications, and no procedure was prematurely ended due to bleeding. 7 Meanwhile, Toepfer et al. analyzed 676 procedures and found that 176 patients were on aspirin, clopidogrel, or warfarin. 12 They analyzed each agent and likewise found no difference in post-operative bleeding rates or overall complications. 12 Similar to the prior studies, we found that continuation of APT during URS does not pose additional bleeding-related risks. However, dual APT was associated with a higher all-cause 30 day readmission rate. This likely reflects the higher CCI of these patients as opposed to being a direct effect of dual APT. No adverse effects from discontinuation of APT were identified.
For patients taking aspirin for secondary prevention of heart attack or stroke, an interruption in aspirin is associated with a three-fold increased risk of cardiovascular and/or cerebrovascular events. 13,14 Notably, 70% of these events occur within 7–10 days of the interruption. 13,14 A randomized control trial found that among patients on low-dose aspirin for secondary prevention, use of a placebo in the perioperative period (−7 to +3 days) was associated with a 9% major cardiac event rate compared with only 1.8% in the group continuing aspirin (p = 0.02). 15 Notably, no difference in bleeding was seen in the two groups. 15 Based on these findings, the British Society of Gastroenterology and the European Society of Gastroenterological 2016 Guidelines recommend that aspirin be continued in all patients, with the exception of a few select very high-risk procedures for bleeding (i.e., tumor resection >2 cm, ampullectomy). 16 Our data similarly support the AUA/ICUD position that aspirin should be continued during URS, posing minimal risk to the patient and it does not compromise surgical outcomes.
Dual APT is indicated for both patients with stable angina and those with unstable coronary syndrome who undergo coronary artery drug-eluting stent placement. Similar to single-agent APT, dual APT (with prasugrel or ticagrel) is also continued for a minimum of 12 months. 17 For stable angina, clopidogrel is given; whereas prasugugrel or ticagrelor is used for unstable coronary syndrome. In either case, the current recommendations are a minimum of 12 months of dual APT to prevent in-stent thrombosis, with more recent studies reporting that patients may potentially benefit for as much as 30 months after stent placement. 18 The mortality rate for in-stent thrombosis is ∼40% and increases substantially after holding dual APT for more than 5 days. Conversely, dual APT is associated with an increased risk of both spontaneous and procedural bleeding compared with single-agent APT. 19 –21 Based on these findings, European guidelines recommend that risk stratification be performed for patients on dual APT undergoing high-risk bleeding. 16 For those at high risk of a thrombotic event, the guidelines panel recommends consultation with a cardiologist to determine what is in the patient's best interest. 16
We found not only increased risk of bleeding in patients who continued APT but also that almost 10% of patients did not have an indication for either full-dose aspirin or clopidogrel. This finding of inappropriate APT use is similar to the findings by Cadiou et al., in which 17% of 219 patients on APT (clopidogrel and/or aspirin) did not have an indication for the medication. 22 Ultimately, 28.8% of patients had their medication discontinued due to a bleeding event or absence of indication for the medication. 22 Conversely, in the series by Cadiou, they noted a significantly higher rate of bleeding-related events, with nearly a quarter of the 219 patients reporting an event. 22 This finding is in line with a prior study by Choudhry et al., who found that among 4977 patients on newly prescribed clopidogrel in 2003, only 39% had a documented Food and Drug Association–approved indication for the medication. 23 The direct economic costs associated with APT overuse were estimated at 1.5 billion dollars. 23 Such studies exemplify the vital role of the urologist in ensuring that patients have the appropriate pre-operative evaluation and work-up, as well as the benefits of multidisciplinary collaboration.
To our knowledge, here, we provide one of the largest studies to date that evaluates bleeding-related complications in patients on chronic APT. Our large sample size allowed us to group patients by both number and type of APT. The study demonstrates that continuation of APT during URS appears safe. Although our overall sample size is larger than that in previous studies, the event rate is still low. We were adequately powered to detect a 3% difference between those holding and those continuing APT; however, we must acknowledge that we are underpowered to detect a potentially significant difference in bleeding-related events below this level. Additionally, nearly all patients who were continued on APT underwent a stone procedure; these findings may not be applicable to diagnostic procedures for evaluation of upper tract urothelial carcinoma or treatment of ureteral stricture.
We recognize that out study was limited by its retrospective design. Patients may have been readmitted outside our healthcare system without notifying our clinic, which would lead to an underestimation of the true complication rate. However, with a standardized 6 week return visit, we anticipate that the number of unidentified outside admissions would be low. Thus, based on our findings, we believe that the risks and benefits of proceeding with URS on APT must be weighed carefully and that in the majority of cases APT therapy does not compromise outcomes of URS. For some patients, the risk of discontinuing APT may be prohibitively high. In such cases, informed decision making is important.
Conclusion
Performing URS in patients who are on chronic APT does not appear to pose additional bleeding-related risks, supporting current AUA/ICUD guidelines on APT in URS. However, further studies with larger sample sizes are needed to confirm this finding. Pending external validation, this information may be used for pre-operative patient counseling.
Footnotes
Author Disclosure Statement
No competing financial interests exist.