
Abstract
Introduction:
The lens of the eye is extremely susceptible to radiation and long-term exposure can induce cataract formation. Our objective was to explore the risk of cataract formation for urologists at our institution.
Methods:
A retrospective review of a multisurgeon database of fluoroscopic cases between October 2013 to December 2014 was queried. Procedures were performed by different subspecialties and ranged from stent insertion/ureteroscopy to percutaneous nephrolithotomy. Fluoroscopic parameters were recorded from all cases and the radiation dosimetry was calculated through methods described by the National Council on Radiation Protection. The data were extrapolated to determine the risk of cataract formation. The technical specifications of the GE OEC 990 mobile C-arm unit were used for calculations.
Results:
A total of 780 cases were analyzed, of which 182 were endourology cases. Average fluoroscopic time was 34.86 seconds per case. Average tube potential and current were 86.84 kV and 1.95 mA, respectively. Pediatric urologists utilized fluoroscopy the least, 11.84 seconds per case (p = 0.0022). Endourology trained faculty had fluoroscopy exposure of 68.35 seconds per case (p < 0.0001), whereas others were exposed 26.24 seconds per case (p < 0.0001). For the highest exposed urologist, the estimated dose to the eyes was 5.64 μGy per case. Total estimated cumulative dose over the study timeframe was 997.58 μGy, or 748.19 μGy per year.
Conclusions:
The defined threshold in the absorbed dose for cataract formation is 0.5 Gy. Resident exposure was the highest, at 11% of the annual limit, and the most exposed urologists had an estimated dose of 5% of the annual limit. At current exposure levels, it would not be feasible to reach the stated safety limit during 50 to 60 years of practice. However, changing exposure guidelines could result in stricter safety limits.
Introduction
F
Methods
A retrospective review of a multisurgeon, prospectively maintained database of fluoroscopic cases between October 2013 to December 2014 was queried. A total of 780 fluoroscopic cases were identified. The procedures were performed by different subspecialties of urology and included stent insertion, ureteroscopy (URS), and percutaneous nephrolithotomy (PCNL). A total of 18 urologists were included in the study, with 2 being endourology fellowship trained. The endourologists' scope of practice was evenly distributed between urolithiasis and robotics. Our endourologists routinely obtained their own accesses during PCNLs. A GE OEC 990 mobile C-arm unit was used for the majority of cases. The unit was equipped with a beam-on timer and the kilovoltage and milliampere were recorded from all the cases in the operating room (OR). All OR personnel wore lead aprons with minimal lead thickness of 0.25 mm and a thyroid shield. No urologists utilized any protective eyewear during our study timeframe. This limited the radiation dose exposure and subsequent calculation to areas not covered by the lead apron or shield.
We calculated the radiation dosimetry of urologists through the methods described by the National Council on Radiation Protection (NCRP) for calculating the exposure rate for differing scattering angles at a given radiation output and field size. See Figure 1 for the scattered dose equation. In this Ks represents the scattered exposure rate at dsec, Ku is the incident exposure at 1 m, F is the field area, and dFSD is the X-ray focus-to-surface distance. The constant a is a function of energy and angle of scatter and the difference values can be found in table B-2 of NCRP 49. 6 In addition, the surgeon was assumed to be standing at a distance of 75 cm with a scattering angle of 45° to estimate the radiation dose to the surgeon's eye. We then extrapolated the dose exposure to determine risk of cataract formation.

Exposure rate equation for differing scatter angles at a given radiation output and field size. Ks represents the scattered exposure rate at dsec, Ku is the incident exposure at 1 m, F is the field area, and dFSD is the X-ray focus-to-surface distance. The constant a is a function of energy and angle of scatter.
Results
The average fluoroscopic time was 34.86 seconds per case. The average tube potential and tube current was 86.84 kV and 1.95 mA, respectively. The surgeon and case characteristics of the rest of the cases are shown in Table 1. Pediatric urologists used the least amount of fluoroscopic time, 11.84 seconds per case (p = 0.0022). Endourology fellowship trained urologists utilized the longest time of fluoroscopy, 68.35 seconds per case (p < 0.0001) (Fig. 2). In contrast, nonendourologists utilized only 26.24 seconds per case (p < 0.0001). The tube potential and current for endourology cases were recorded as 90.84 kV (p = 0.07) and 1.87 mA (p = 0.138). The total number of cases by endourologists over the past year was 182. A large proportion of their cases involved fluoroscopy-intensive procedures: URS (49.5%), PCNL (18.7%), and stent insertion/exchange (16.5%). In contrast, our other urologists performed URS, PCNL, and stent procedures at 28.9%, 4.7%, and 23.4% of their cases, respectively. In addition, because of the complexity, the operative times tended to be longer for the endourologists' procedures: URS (85.6 minutes vs 60.3 minutes), PCNL (218.9 minutes vs 162.0 minutes), and stent insertion/exchange (29.5 minutes vs 23.9 minutes). Given the more substantial fluoroscopic time and high volume of cases, we identified the endourology fellowship trained urologists as the most susceptible to cataract formation. For the calculated dosimetry, the surgeon was assumed to be standing 75 cm from the source and an angle of 45° was used to estimate a dose for the head. An X-ray beam-to-focus distance of 75 cm was used for all calculations (Fig. 3). Using the average exposure data and these parameters, we then calculated the estimated radiation dose to the eyes for our most highly exposed urologists to be 5.64 μGy per case. For the study timeframe, the total estimated cumulative dose would then be 997.58 μGy, or 748.19 μGy per year. Resident participation was also ubiquitous throughout these cases and represents another susceptible individual to radiation exposure. If a single resident were to assist and perform all the endoscopic urology cases, the annual dose would be calculated at 1.71 mGy.
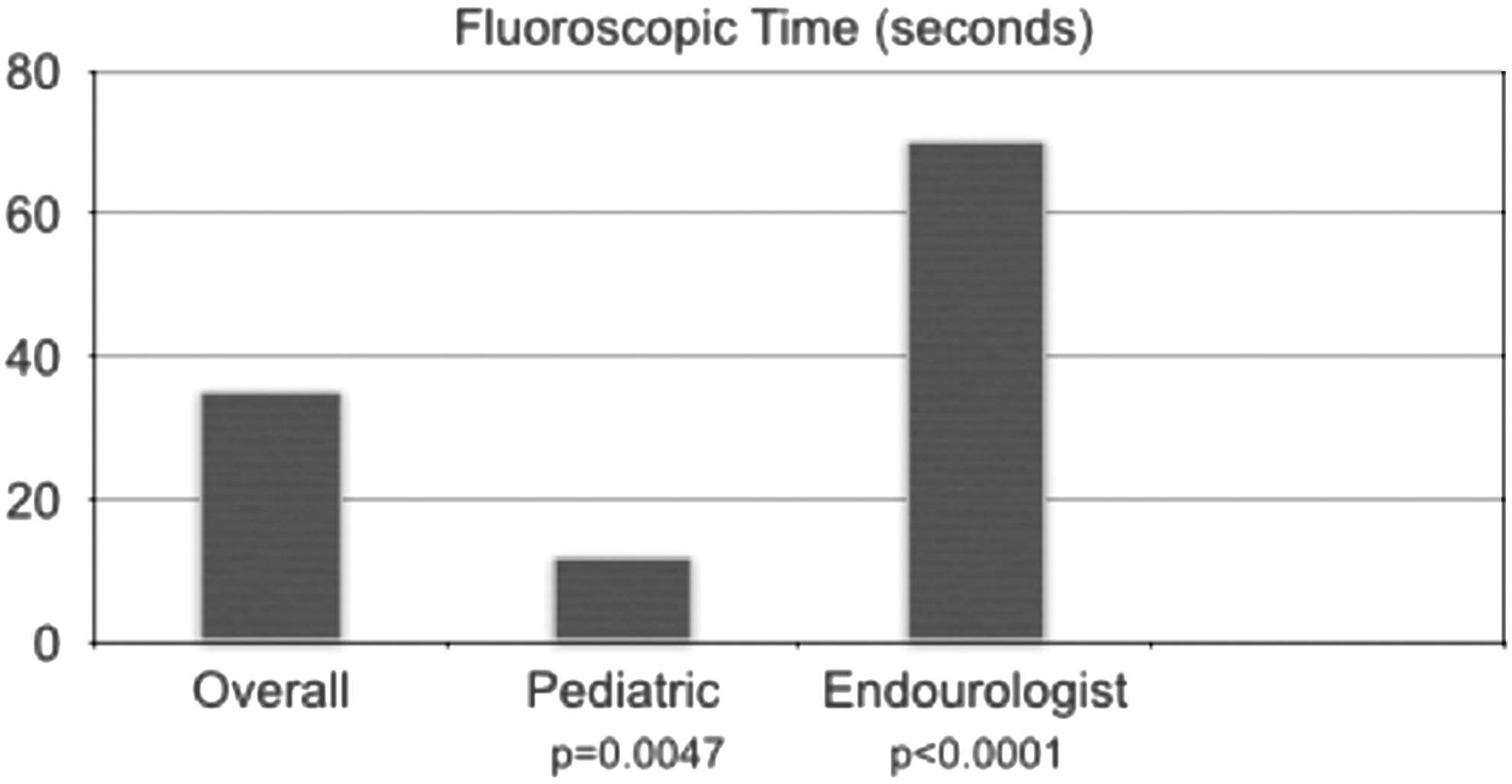
The average fluoroscopic time for a case dependent on urologic subspecialty.
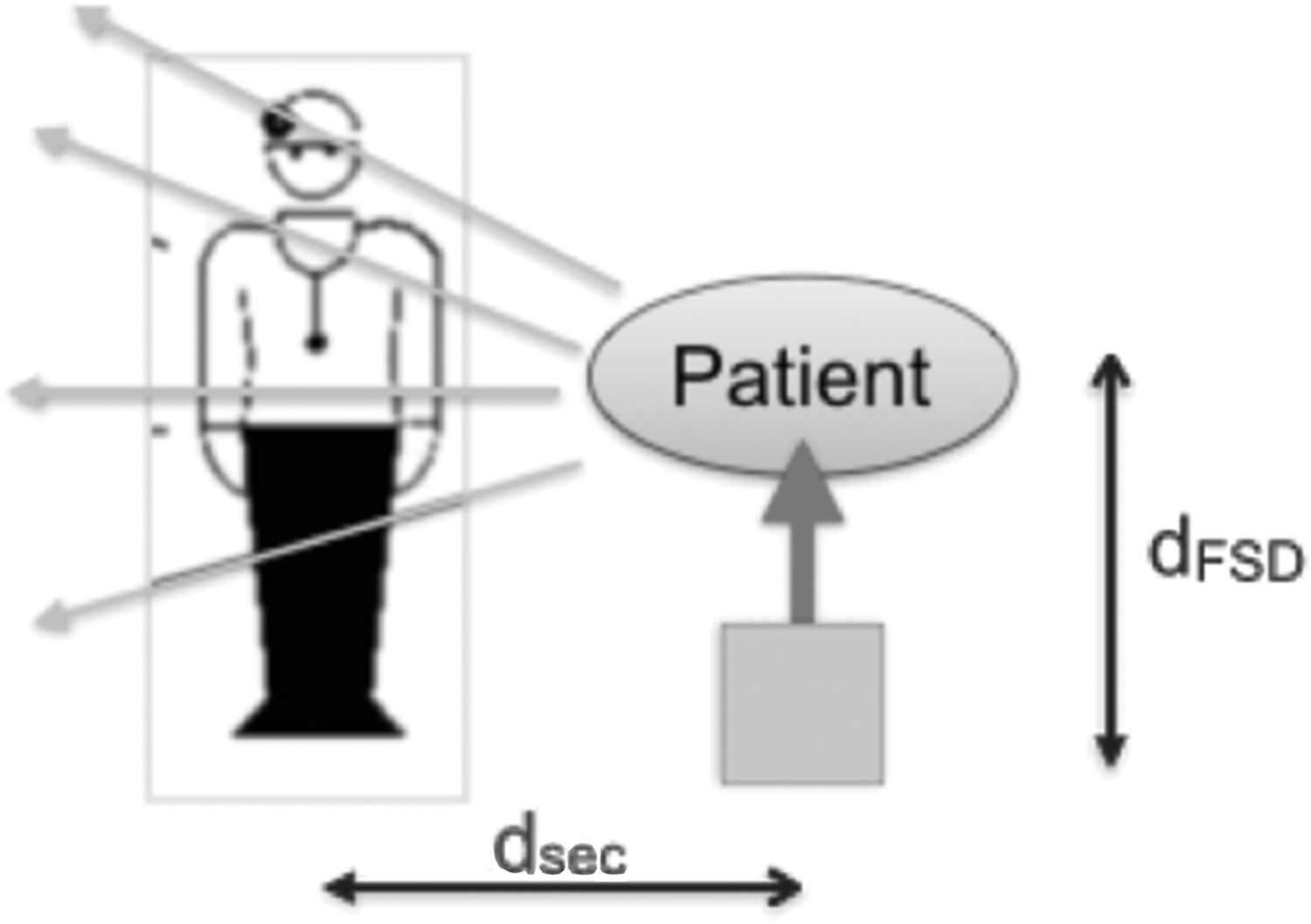
Schematic of surgeon location for calculation of exposed dosimetry. The surgeon was assumed to be standing 75 cm from the source and an angle of 45° was used to estimate a dose for the head. The X-ray beam-to-focus distance was 75 cm.
Discussion
When evaluating radiation exposure through fluoroscopy, it is important to first recognize that the vast majority of our urologic procedures during this timeframe were performed with the GE OEC 990 C-arm. Procedures that were incorporated within our study ranged from stent insertion/exchange, URS with laser lithotripsy to PCNL. It has been noted that with advances in ureteroscopic and minimally invasive technology, urologists have become more aggressive with their instrumentation approach for treatment of upper tract pathology analysis as time has gone on. 7 Cohen et al. demonstrated that URS alone represented 47% of fluoroscopy cases that one surgeon performed. 8 It is evident that ureteroscopic procedures are becoming the major contributor to radiation exposure for the urologist, and for that reason, the timing of our study provides a more accurate look at radiation exposure of the urologist in today's practicing environment. It is also important to note that practice patterns observed here might not be representative of urologists who do not perform many URS procedures or who do not treat advanced stone disease.
Frequent fluoroscopy use and radiation standards have prompted new standardized and optional protective measures to reduce radiation exposure rates. Standard measures at our institution include a lead-lined apron that drapes over the chest and pelvis, and thyroid shields. Other protective measures include dosimeters, lead-impregnated glasses, and gloves, none of which were consistently used at our institution. This highlights the importance of compliance with protective equipment as having an effect on radiation exposure. A recent survey sent to the Endourological Society demonstrated that compliance with chest and pelvic shields was largely ubiquitous, at 97%. In stark contrast, the use of other protective instruments was much lower: thyroid shields, dosimeters, lead-impregnated glasses, and glove compliance rates were only 68%, 34.3%, 17.2%, and 9.7%, respectively. 9 The low utilization of eye protection by the practicing urologist is of concern because of the fact that the human eye is particularly sensitive to ionizing radiation. After exposure, changes consisting of small dots and vacuoles occur to the lens. Over time, these aggregate to form large opacities and form cataracts. These changes have been seen in bomb survivors and early cyclotron workers. 10,11
Early studies into cataract formation showed a dose–effect relationship. However, more recent studies have also shown that a chronic exposure will also lead to cataract formation. 12 –15 Because of these and many other studies, the ICRP has imposed ocular radiation exposure guidelines in hopes of reducing cataract formation rates in those people exposed to radiation on a common basis.
The ICRP guidelines on ocular radiation have recently undergone a significant change in their recommendations for exposure limits. Before 2011, the ICRP held that the human threshold value for radiation cataract genesis was 2 Gy in a single exposure and 5 Gy for fractionated or protracted exposure, and thus recommended occupational lens exposure limits of 150 mSV/year. 15,16 These old guidelines were strongly influenced by >60 years of studying the lens changes of atomic bomb survivors. These studies helped influence the previous guideline recommendations by suggesting that the threshold for radiation-induced cataracts was ∼1.5 Gy. 5,15,17,18 More recent studies, however, evaluated radiation exposure in populations with lower radiation doses than those at Hiroshima and have shown that significantly lower radiation dose exposures are associated with lens opacification. 12,15,19 These studies lead to a reevaluation of the ocular radiation guidelines by the ICRP. In 2011, the ICRP changed its guidelines by reducing the radiation cataracts threshold to 0.5 Gy/year and the occupational lens exposure limit to 20 mSv/year for 5 years with no single year exceeding 50 mSv, regardless of exposure in an acute, protracted, or chronic setting. 20
For our study, the most exposed urologist had an effective annual dose of 748.19 μGy. If we assume that exposure results in complete absorption to the lens, which represents the worst case scenario, then this absorbed dose would result in ∼5% of the yearly limit. To put this in perspective, ambient radiation leads to an effective dose of 6.2 mSv for the average individual in the United States and a CT scan of the head results in a dose of 2 mSv, comprising ∼40% and 13.33% of the yearly limit. 21 Worst case scenario for resident exposure theoretically led to an annual dose of 1.71 mGy, representing 11% of the annual limit. The resident exposure calculation did not need any change to our model because of the fact that they were performing the endoscopic case and routinely were closest to the radiation source. Although a busy urology practice or residency will result in increased radiation exposure, when comparing with ambient radiation and other exposures, the additional radiation load is well within currently defined radiation standards. It is important to note, however, that if the workload of endoscopic or fluoroscopy-intensive procedures increases, then the risk of cataract formation also increases accordingly.
Although our urologic surgeons and residents may be exposed to minimal doses compared with yearly limits, these exposure metrics may not be applicable to a generalized population. One potential reason is that our low fluoroscopy times are from a strict adherence to the as low as reasonably achievable (ALARA) principle. In fact, quoted rates in the literature have shown a wider range and increased variability in fluoroscopic times. Average time for URS has varied from 37 to 189 seconds, with fluoroscopy time for PCNL showing a range of 200 to 679 seconds. 22,23
Our study did have other limitations also. The urologists at our institution did not utilize dosimeters on a regular basis and thus we were unable to read exact exposure rates. Without exact measurements, we relied on calculations to estimate the radiation exposure rates of our urologists. Furthermore, the radiation dose to the lens of the eye is a function of absorbed dose at a different depth than what traditional thermoluminescent dosimeters would measure. In addition, a few cases at the end of the year were performed using a cystoscopy table with the fluoroscopic emitter on the top rather than at the bottom as seen on mobile C-arm units. Therefore, we would expect an increase in absorbed and exposed dosages to the surgeon lens. We also must acknowledge that other factors can put urologists at risk for cataracts, including increasing age, heredity, smoking, excessive UV-B exposure, diabetes, and steroidal treatment. 24 It is hard to accurately assess the direct influence of radiation exposure on increasing the risk of cataracts within our urologist population.
Conclusion
Yearly eye exposure limits are currently defined at 15 mSv by the IRCP. Resident exposure was the highest, at 11% of the annual limit, and the most exposed urologists had an estimated dose of 5% of the annual limit. At current exposure levels, it would not be feasible to reach the stated safety limit during 50 to 60 years of practice. We conclude that fluoroscopy is a safe modality. Also, with the use of newer technologies and sensible radiation principles, the risk of cataract formation to the surgeon is diminishing. However, changing safety guidelines could further restrict allowable limits of exposure in the future.
Footnotes
Acknowledgments
This work was previously presented at the American Urological Association meeting in 2015 and published as a conference abstract. The full abstract can be found at
Author Disclosure Statement
No competing financial interests exist.