
Abstract
Purpose:
To evaluate the long-term clinical efficacy and safety of double-layered polytetrafluoroethylene membrane-covered self-expandable segmental metallic stents (Uventa) in patients with chronic ureteral obstruction.
Materials and Methods:
In a retrospective study, a total of 50 ureter units (44 patients) with chronic obstructions were included from July 2010 to May 2015. Indications for Uventa placement were primary stenting for malignant ureteral obstruction, failed conventional polymeric Double-J stent (PS), or percutaneous nephrostomy (PCN) technique, with comorbidities or fears limiting PS/PCN changes, or with irritation or pain due to PS/PCN. Patients underwent Uventa stent placement using the antegrade or retrograde approach.
Results:
There were no immediate procedure-related complications, and all stents were placed in the proper sites. During the median follow-up of 30.9 (interquartile range [IQR], 8.1–49.0) months, the primary (no obstruction and no additional intervention) and overall success (no obstruction and no additional intervention except supplementary Uventa) was 30.0% and 34.0%, respectively. Moreover, 14 of 50 ureter units (28.0%) experienced major complications (≥Clavien-Dindo class IIIb), such as ureteroarterial fistula (three cases, 6.0%), ureteroenteric fistula (three, 6.0%), ureterovaginal fistula (one, 2.0%), ureter perforation (one, 2.0%), uncontrollable bleeding (one, 2.0%), and complete obstruction (five, 10.0%). On univariate analysis, major complications were associated with female (odds ratio [OR] = 6.000), cervical cancer (OR = 4.667), ureteral stricture length (≥6.0 cm, OR = 4.583), and placement duration (≥24.0 months, OR = 20.429; all p < 0.05).
Conclusions:
In long-term follow-up, the Uventa stent demonstrated poor treatment outcomes with frequent major complications in patients with chronic ureteral obstructions.
Introduction
U
To address these problems, some types of metallic stents have been designed. 10 –13 Generally, self-expandable segmental metallic stents were expected to have less frequent stent-related complications, such as irritation, compared with full-length type stents. However, segmental stents also had their own problems. The incipient type of bare-formed single-layered segmental metallic stent (Wallstent; Boston Scientific, Miami, FL) showed extremely limited patency rates (31.0%–36.3% during 3.0–12.0 months), 14,15 which are caused by tissue hyperplastic reaction or tumor ingrowth into the stent rumen. To prevent such tissue ingrowth, externally coated single-layered segmental stents (Passager; Boston Scientific, Miami, FL) were used for ureteral obstruction. 16 However, this polytetrafluoroethylene (PTFE) membrane-covered segmental stent caused high rates of stent migration as much as 81.0% because of the lack of firm adhesion of the stent to the adjacent tissue. 16,17
The double-layered PTFE membrane-covered segmental metallic stent (Uventa; Taewoong Medical, Republic of Korea) is designated to minimize these problems. 18 The Uventa is structured with double-layered nitinol alloy self-expandable stents. The outer stent provides a high friction coefficient that prevents stent migration, and the inner stent reinforces overall radial force to maintain stent patency. Between the double-layered structures, the PTFE-membrane layer is covered to prevent tissue ingrowth. 18 In animal models, this novel stent effectively prevented the luminal tissue ingrowth, while no migration was observed. 19 Early reports regarding the Uventa stent in the treatment of malignant ureteral obstruction have shown promising patency rates (81.7%–100.0% during 7.2–10.0 months) without any stent-related severe complications. 18,20
However, despite the promising results of Uventa segmental ureteral stent in short-term follow-up reports, 18,20 the efficacy of the Uventa stent is missing in long-term follow-up and it should be determined. In our institution, we have had patients with Uventa segmental stent-related major complications that required surgical interventions under general anesthesia. Therefore, we investigated the long-term efficacy and safety of that segmental metallic stent for treatment of chronic ureteral obstruction utilizing our consecutive subjects.
Materials and Methods
Patient selection
This retrospective study was approved by our institutional review board. All patients provided informed consent for placement of Uventa. Between July 2010 and May 2015, a total of 44 patients (19 men and 25 women) who had chronic ureteral obstruction underwent Uventa placement. Because six patients had bilateral obstruction, Uventa was placed in a total of 50 ureter units.
Detailed procedures
The stents were placed in a retrograde or antegrade manner considering the individualized conditions. Detailed descriptions of the Uventa stenting have been previously described elsewhere. 18,20 Briefly, retrograde or antegrade pyelography was performed to access the location and length of the obstruction in the ureter. Then, a 0.035-inch Amplatz Super Stiff guidewire (Boston Scientific, Miami, FL) was negotiated through the obstruction to mount the delivery system of the Uventa stent. At the location where the obstruction is present, the stent was deployed. We utilized the Uventa stent with a 7.0 mm diameter that ranged from 6.0 to 12.0 cm in length depending on the stricture length. In long strictures, the stents were placed overlapping by 2.0–3.0 cm. If the stent was not fully expanded after placement, additional ureteral dilation was performed using a 6.0-mm balloon catheter (UroMax Ultra; Boston Scientific, Miami, FL). The procedure was routinely performed under local anesthesia; however, some cases were done under general anesthesia by patient request.
Follow-up and outcome evaluations
Patients were followed up every 3 months for the first 2 years and every 6 months thereafter. At each follow-up, patency of the inserted stent and stent-related complications was assessed. Treatment efficacy was assessed using previously proposed criteria. 20 Briefly, primary success was defined as the maintenance of stent patency without any additional interventions. In some of the primary failure cases, the patency was salvaged by additional Uventa stenting. Those cases were classified as overall success. Patients who died without stent obstruction were regarded as success until the date of death. Complications related to the Uventa stent were assessed using the Clavien-Dindo classification system. 21 A major complication was defined as one that required a surgical, endoscopic, or radiologic intervention under general anesthesia (≥class IIIb). Due to the nature of a retrospective study, the times until the relevant events, such as treatment failure or occurrence of complications related to the Uventa stent, were censored. Therefore, censored survival times might underestimate the true times to event.
Statistical analyses
Descriptive data of all results are presented as the median and its interquartile range (IQR) or number with its percentile. The primary and overall treatment success rates of Uventa placement for ureteral obstruction were estimated using Kaplan–Meier curves. Binary logistic regression was performed for identifying the risk factors for major complications. All statistical tests were two-tailed, with p < 0.05 considered to indicate significance. Statistical analyses were performed using commercially available software (SPSS® 21.0, Chicago, IL).
Results
Baseline characteristics
Out of the 44 patients (19 men and 25 women) who received the Uventa stenting, the median age of all subjects was 60.7 (IQR, 54.2–68.0) years. Out of the 50 ureter units (23 right and 27 left units), malignancy-related obstruction was the most common (41 U, 82.0%), followed by benign causes (8 U, 16.0%) and idiopathic (1 U, 2.0%; Table 1). Failed conventional PS/PCN was the most common reason for Uventa stenting (31 U, 62.0%; Table 1). Median length of stricture lesions was 6.0 (3.9–10.0) cm. Almost procedures were performed under local anesthesia (39 U, 78.0%) in a retrograde manner (44 U, 88.0%). Simultaneous balloon dilation was performed in approximately half of cases (24 U, 48.0%; Table 2).
IQR = interquartile range; PCN = percutaneous nephrostomy; PS = polymeric Double-J stent.
Treatment outcomes of Uventa stents
All Uventa stents were effectively placed at the planned location without any immediate procedure-related complications. In total, median follow-up duration was 30.9 (8.1–49.0) months. During the follow-up period, 16 (36.4%) patients with 19 (38.0%) stents died due to underlying diseases at a median time of 10.2 (4.9–17.9) months after the stenting procedure. The primary success rate was 30.0% (15 of 50 U; Table 3). Of the 35 (70.0%) primary failure cases that occurred at a median duration of 7.5 (3.7–20.1) months, tumor progression beyond the covered stent was the most common cause of failure (9 U, 18.0%), followed by stent migration (7 U, 14.0%; Table 3). Additional Uventa stents were placed in four cases (three cases with tumor progression and one case with stent migration). Of these four cases, two cases maintained patency during the additional follow-up of 4.0 (2.7–4.2) months. Therefore, the overall success rate of our series was 34.0% (15 U with primary success plus two salvaged units; Table 3). The estimated 3-year primary and overall treatment success rates were 26.5% and 27.3%, respectively (Fig. 1).
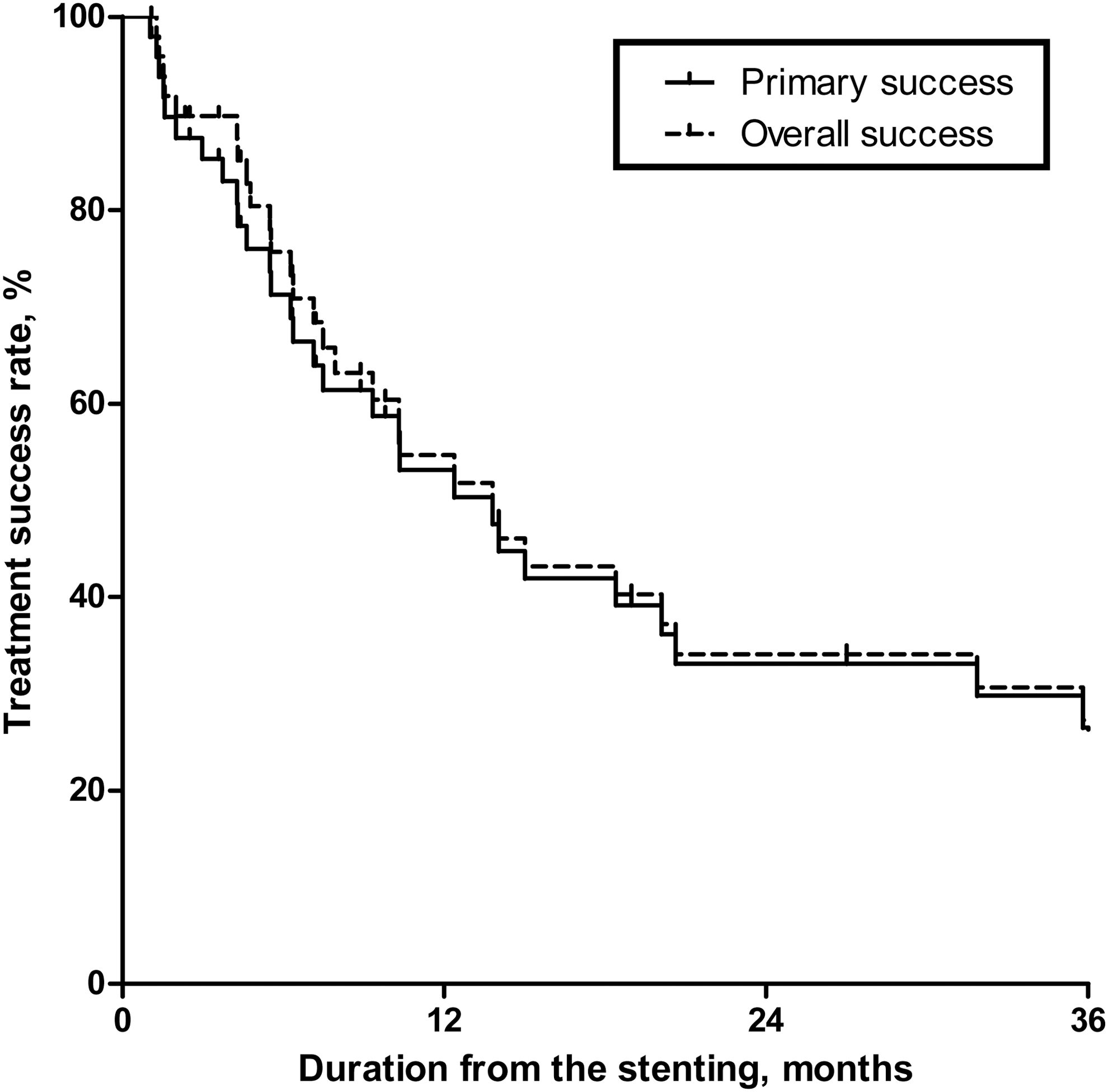
Kaplan–Meier curves for primary and overall treatment success rates of the Uventa segmental stents for ureteral obstruction. The estimated 3-year primary and overall treatment success rates were 26.5% and 27.3%, respectively.
Incidence of complications and their risk factors
Of the 50 ureter units, Clavien-Dindo class II, IIIa, and IIIb complications were observed in 2 (4.0%), 13 (26.0%), and 14 (28.0%) units, respectively. Details of 14 major complications (≥class IIIb) are presented in Table 4. Major complications developed at a median time point of 27.1 (11.9–41.9) months after stent insertion.
Direct ureteral injuries occurred in nine cases (18.0%). Three (6.0%) cases of ureteroarterial fistulas occurred (Case 7, 12 [left], and 13 in Table 4). These lesions were confirmed by CT scan (Fig. 2A) and femoral arteriography (Fig. 2B). Those were resolved by primary endovascular stenting with delayed open surgery. Three cases (6.0%) of ureteroenteric fistulas confirmed by CT scan or retrograde pyelography (Fig. 2C, D) were developed (Case 8, 11, and 12 [right] in Table 4). One woman complained of watery discharge through the vagina and was found to have ureterovaginal fistula by cystoscopy and antegrade pyelography (Case 5 in Table 4 and Fig. 2E, F). One case of ureter perforation without formation of a fistula also occurred and was resolved by nephroureterectomy (Case 1 in Table 4). One woman with a long segment stricture suffered from uncontrollable bleeding without evidence of ureter perforation, and she received an ileal ureter to resolve that problem (Case 9 in Table 4).
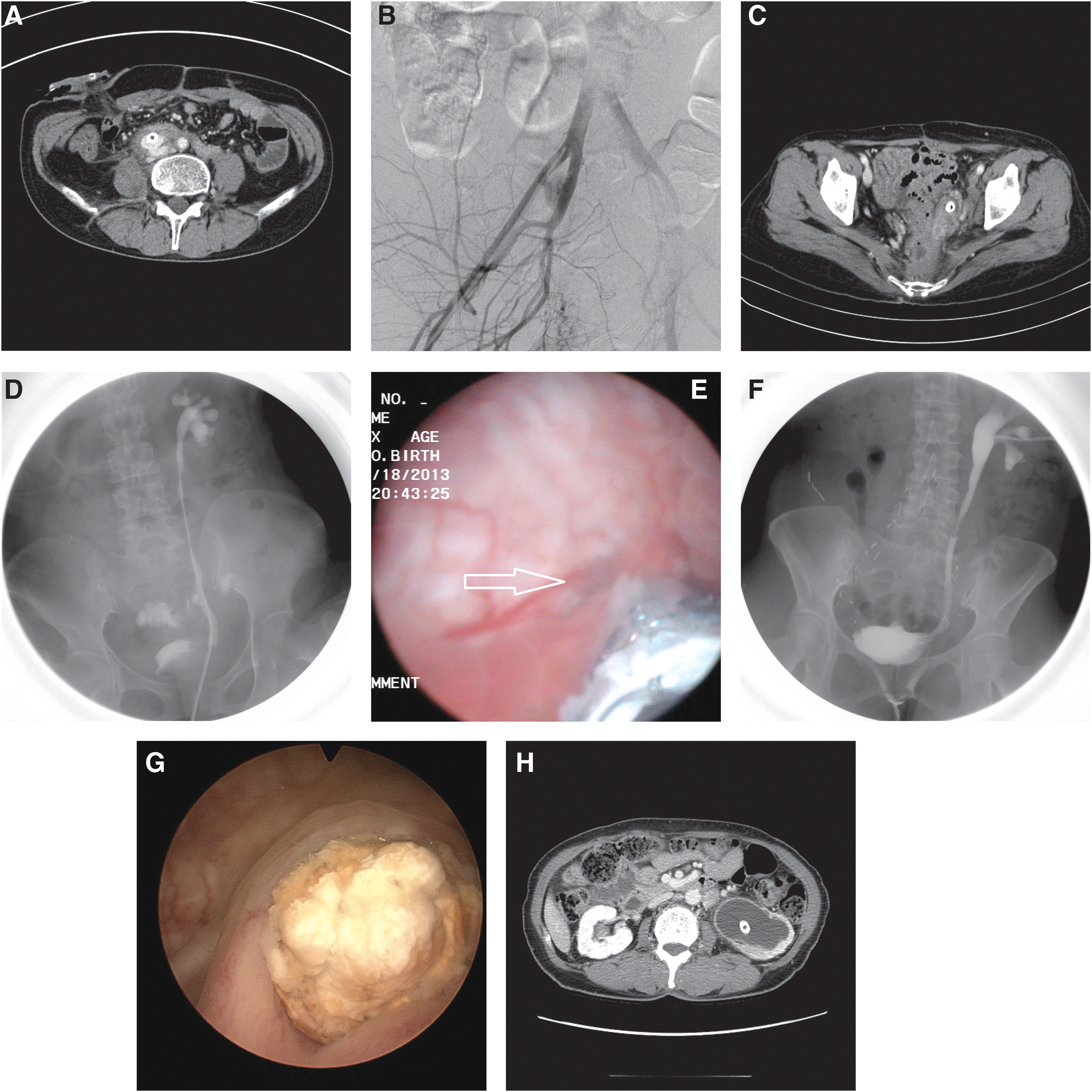
Representative pictures of major complications associated with metallic stenting. Ureteroarterial fistula:
Five cases (10.0%) of complete stent obstructions occurred. Two obstructions were caused by stone encrustation (Case 2 and 6 in Table 4 and Fig. 2G), two were due to functional failure (Case 3 and 4 in Table 4), and one was due to stent migration to the renal pelvis (Case 10 in Table 4 and Fig. 2F). Stent removals by endoscopic procedures were tried, but in all the cases, the stent could not be removed because of insufficient handholds to grasp the stent and firm adhesion of the stent to surrounding tissue. Therefore, all cases were recommended the open surgery to resolve the related problems (Table 4).
Major complications were associated with gender (female, odds ratio [OR] = 6.000; p = 0.032), cervical cancer (OR = 4.667; p = 0.022), ureteral stricture length (≥6.0 cm, OR = 4.583; p = 0.038), and stent placement duration (≥24.0 months, OR = 20.429; p = 0.006; Table 5). Patients with a history of radiation therapy were more likely to experience major complications (OR = 3.030), but this failed to reach the statistical significance level (p = 0.088).
CI = confidence interval.
Discussion
Outcome of Uventa stents: comparisons with previous studies
A double-pigtail, full-length, spiral coiled metallic stent (Resonance; Cook Medical, Bloomington, IN), which has a similar shape to the conventional PS, demonstrated good short-term outcomes in intractable ureteral obstruction (70.0%–87.0% during the 8.5–13.0 months of median follow-up). 10,11 However, treatment outcomes were considerably compromised in cases of irradiated ureters (27.0%–50.0% during the 5.0–9.0 months of follow-up), 12,13 and they needed frequent stent changing and caused frequent irritation (as much as 56.5%) due to tailed tip in the bladder. 10 –13
Generally, self-expendable, segmental ureteral stents can be expected to have less frequent stent-related complications, such as irritation, compared with full-length stents. Kim and colleagues first reported their initial experience with the Uventa stent, and they mentioned that the patency rate was 100.0% (20 of 20 U) during a median follow-up of 7.3 months. 18 However, de novo ureteral obstruction occurred in four ureter units (20.0%) during that period, 18 which were considered as treatment failure in the studies of Chung and colleagues 20 and ours. Chung and colleagues adopted similar inclusion criteria and definition of treatment success to our study. 20 They reported that the primary and overall success rates were 64.8% (46 of 71 U) and 81.7% (58 of 71 U), respectively, at the median follow-up time point of 10.0 months. 20 Moreover, they reported that the incidence of failure tended to stabilize, because almost all primary failures occurred within 6 months of stent placement (80.0%, 20 of 25 failures). 20 Our overall success rate of Uventa stent at short-term follow-up (57.5% at postoperative 10 months; Fig. 1) was consistent with the outcome from the study by Chung and colleagues (64.8% at 10 months). 20
However, our long-term (median 30.9 months) observation of the Uventa stent is different. The primary (30.0%, 15 of 50 U) and overall success (34.0%, 17 of 50 U) rates were much lower than in previous studies (Table 3). Unlike the study by Chung and colleagues, the occurrence of primary failure did not stabilize within 6 months after stent placement; more than half of failures occurred later than 6 months (60.0%, 21 of 35 failures). This finding implies that failure risk is time dependent. Although almost all our patients (35 patients with 41 ureter units) had malignancy-related ureteral obstructions, approximately two-thirds of them (63.6%, 28 of 44 patients) survived during the follow-up period. This means that the durability of Uventa stent is not guaranteed for the life expectancy of patients, even if they had advanced malignancy causing ureteral obstruction.
Our data showing tumor progression beyond the stent as the most common cause of primary failure (18.0%, 9 of 50 U) are in accordance with a previous study (25.3%, 18 of 71 U). 20 However, failures were caused by many other reasons in our subjects (74.3%, 26 of 35 failures; Table 3), while tumor progression was the only dominant cause of primary failure in the study of Chung and colleagues (72.0%, 18 of 25 failures). 20 This difference reveals some important clinical implications. First, underlying diseases, such as malignancies, were well controlled in a substantial portion of patients, and they experienced relatively long survival times. Therefore, failures tended to be caused by reasons other than tumor progression during the long-term follow-up period. In these cases, the durability of the Uventa stent was not sufficient considering the life expectancies of the patients, even if stenting was performed in a palliative setting. Second, there may be fewer chances to place additional Uventa stents in late-onset primary failures, because they were not primarily caused by tumor progression. In a previous study, additional Uventa stents were placed and primary failures could be rescued in 12 cases (nine tumor progressions and three mucosal hyperplasia cases), therefore the overall success rate was much improved (64.8%–81.7%). 20 However, in our present study, only four patients could receive additional Uventa stents, and two of these patients were overall failures due to further progression of the obstruction; therefore, the overall success rate was not much improved (30.0%–34.0%; Table 3).
Major complications
More importantly, major complications occurred in 14 cases (28.0%; Table 4), whereas previous studies have reported no severe stent-related complications. 18,20 The short-term follow-up durations of previous studies (median 7.3 and 10.0 months) are probably the cause of this discrepancy. 18,20 In our series, 14 major complications occurred at a median 27.1 months after stent placement (Table 4).
The most common major complications were direct ureteral injury with (or without) fistula formation to adjacent organs (18.0%, 9 of 50 U). We presume that the double-layered structure of the Uventa stent, which is designed to provide radial force to maintain patency, consistently compressed the ureter and encouraged mucosal ischemia that eventually caused those direct ureteral injuries. Ureteroarterial fistulas, which are potentially life-threatening complications due to bleeding, occurred in three cases. That rate (6.0%) is extremely high considering that a previous review of this complication identified less than 100 patients in the literature. 22,23 Fortunately, all three cases could be managed by primary endovascular stenting and delayed elective open surgery. All three patients developed gross hematuria as an initial manifestation. In these patients, a high level of suspicion and prompt evaluation was important.
Complete obstruction occurred in five patients (10.0%; Table 4). As mentioned, the Uventa stent is designated to endure the tissue ingrowth and stent migration. Nevertheless, stone formations or functional failure was inevitable in the long-term follow-up. Moreover, 11 stents (22.0%) migrated and 7 migrations (14.0%) caused stent failure (Table 3). Stent migration was not associated with concomitant balloon dilation during stent placement (OR = 1.140; 95% confidence interval, 0.298, 4.365). All these completely obstructed stents could not be removed with endoscopic procedures, unlike previous studies reporting that two Uventa stents could be removed with ureteroscopy. 20
Patients who developed major complications after Uventa placement were stereotypical middle-aged women with a history of gynecologic cancer and previous radiotherapy, but whose underlying cancer was well controlled (Tables 4 and 5). Of the five patients who needed concomitant small bowel surgeries (Case 3, 5, 8, 9, and 12 [bilateral] in Table 4), four patients (80.0%) had a history of radiation therapy. In those cases, the surgical corrections were technically challenging because the irradiated small bowels were unhealthy and fragile. However, the underlying causes in all patients with major complications were well controlled and their acceptable life expectancy rationalized the open surgery. On these grounds, we believe that the Uventa placement, even if it is performed in a palliative setting, should be reconsidered.
Limitations
The results of the current study are limited by its retrospective nature and small number of subjects. However, we believe that our small but long-term experiences are sufficient to draw attention to the lack of long-term safety of metallic stenting placement. Although multivariate risk analysis could not be performed because of the high collinearities among risk factors (e.g., female, cervical cancer, radiation history), we could identify a type of patient who has a higher risk of major complications after stent placement. Finally, assessment to measure the HRQoL of patient could not be performed due to the retrospective nature of this study.
Conclusions
In long-term follow-up, the treatment outcome of Uventa stent placement for chronic ureteral obstruction was poorer than those of previous studies. Moreover, major complications that required surgical interventions under general anesthesia were not uncommon and they were sometimes life threatening. Considering the acceptable life expectancies of indicated patients, placement of a Uventa stent should be reconsidered and technical improvements of metallic stents are necessary.
Footnotes
Author Disclosure Statement
No competing financial interests exist.