
Abstract
Purpose:
Diuretic renography (DRG) is commonly used to diagnose ureteropelvic junction obstruction (UPJO) and to evaluate the success of surgical repair (pyeloplasty). Duration, frequency, and interpretation of renographic follow-ups are still under dispute.
Methods:
We retrospectively reviewed 94 consecutive patients diagnosed with UPJO who underwent a minimally invasive, robotically assisted laparoscopic pyeloplasty at our institution between January 2009 and September 2015. DRG was carried out preoperatively and again routinely 4 to 6 weeks postoperatively the day after stent removal (early DRG). Patients were scheduled for repeat (late) DRG and follow-up examinations, including clinical status and ultrasonography.
Results:
Nineteen patients with missing preoperative DRG were excluded from the study; the remaining 75 patients were eligible for statistical evaluation. At follow-up, 98.7% reported no or only very mild and rare symptoms. On early DRG, 52.5% had T1/2 ≤ 10 min (unobstructed), 39.3% had T1/2 between 10 and 20 minutes (equivocal), and 8.2% had T1/2 ≤ 20 minutes (obstructed). At late follow-up, the DRG results had improved to 80.8% unobstructed with 19.2% remaining equivocal, and no patients were obstructed; thus, the overall success rate was 80.8%. There was only one patient who worsened from unobstructed to equivocal from early to late DRG assessment.
Conclusion:
In case of complete symptom resolution, a nonobstructive diuretic half-time of ≤10 minutes on early DRG following stent removal suggests that further routine renographic follow-up is unnecessary. Patients with an equivocal early DRG (T1/2 between 10 and 20 minutes) require further scintigraphic follow-up, as they have a 42.1% chance of staying equivocal.
Introduction
O
Contemporary series show success rates of over 90% for RALP, 2 –4 which are identical to those of the former gold standard of open Anderson–Hynes dismembered pyeloplasty. 5 However, there still exists great variability among different studies in terms of criteria used to define success. 6 In general, DRG (diuretic renography) is widely recognized as the best noninvasive technique to objectively assess upper urinary tract obstruction. Following the Radionuclides in Nephrourology Group—Consensus Committee on Diuresis Renography, 7 recent series and reviews 6,8,9 define their overall success rate by a clearance half-time of ≤10 minutes following intravenous furosemide administration (T1/2) on DRG. Consistently, a recent study of 61 RALPs suggested that if this strict radiographic definition, together with symptomatic relief using a validated pain analog score, was applied, short-term cure rates would translate into durable success rates. 8 Analysis of cure rates is important because several series reported late failures beyond 2 years. 10,11
In this context, our study examined the prognostic value of these scintigraphic criteria for a definitive cure, comparing early vs late DRG and symptom scores in 75 consecutive patients after RALP. To our knowledge, this is the largest single-center cohort study evaluating the postoperative course of renographic parameters following RALP.
Materials and Methods
We retrospectively reviewed 94 consecutive patients diagnosed with UPJO who underwent RALP at our institution between January 2009 and September 2015. The indication for surgery was symptomatic UPJO with hydronephrosis, based on clinical symptoms and standard imaging studies, including ultrasonography, intravenous urography, retrograde ureteropyelography, and DRG. Local ethics committee approval was obtained, and participating patients signed informed consent forms (Ethikkommission der Universität Witten-Herdecke). Patient demographics as well as clinical and radiographic outcomes were documented in our patient database and analyzed for perioperative morbidity, complications, and long-term functional outcomes.
Preoperatively, renal ultrasonography, retrograde ureteropyelography, clinical status, and DRG with technetium 99m mercaptoacetyltriglycine (99mTc-MAG3) were performed. A robotic Anderson–Hynes dismembered pyeloplasty technique was performed as described elsewhere. 12 A standard 3-arm technique was used with an additional assistant port. All procedures were performed transperitoneally. If not already indwelling, a ureteral stent was placed intraoperatively. Continuous bladder drainage via Foley catheter was maintained for 24 to 48 hours. Patients were discharged from the hospital with an indwelling Double-J stent.
Patients were routinely scheduled for stent removal and early follow-up, including DRG 4 to 6 weeks postoperatively. Renal ultrasonography and DRG (“early DRG”) were performed the day after stent removal. Further follow-up by their referring urologist or general practitioner, including DRG, was advised. Alternatively, patients were followed up at our institution.
Overall success was based on DRG results and symptomatic improvement. Symptomatic improvement was measured based on the Verbal Pain Intensity Scale: none [0], mild [1], moderate [2], severe [3], very severe [4], worst possible [5]. Patients were considered cured only when no or mild symptoms were reported at follow-up. If the pain level remained the same or increased, we recorded this as a failed procedure. To assess DRG results, patients were subdivided into three categories: unobstructed—T1/2 ≤10 minutes, equivocal—T1/2 between 10 and 20 minutes, and obstructed—T1/2 greater than 20 minutes.
In addition, ultrasonographic parameters, serum creatinine levels, and estimated glomerular filtration rate (eGFR) were recorded.
The data are expressed as the mean, and differences were assessed using a t-test, with statistical significance of differences indicated at 0.05.
Results
A total of 94 patients underwent RALP at our center. Of these, 19 patients without preoperative DRG were excluded from the study. Of the remaining 75, robotic RALP was performed on 35 (46.7%) for right UPJO and 40 (53.3%) for left UPJO, and 1 (1.3%) was performed on a patient with a solitary kidney.
Most patients presented with clinical symptoms such as recurrent flank pain (84%), febrile urinary tract infection (13%), or stone formation (11%). Thirteen percent had been incidental, and 78.7% showed sonographic high-grade (II° or III°) hydronephrosis. The mean age at the time of surgery was 43.9 years (Table 1).
F = female; L = left; M = male; R = right; UPJO = ureteropelvic junction obstruction.
At preoperative DRG, 51.8% had T1/2 between 10 and 20 minutes (equivocal), 21.4% had T1/2 ≤10 minutes (nonobstructed), and 26.8% had T1/2 greater than 20 minutes (obstructed) (Figure 1). The mean preoperative DRF at the affected site was 45.8% ± 9.6% and GFR was 110 ± 34 mL/min. All procedures were performed exclusively by two experienced robotic surgeons (B.U. and M.H.). No case was converted to open surgery.
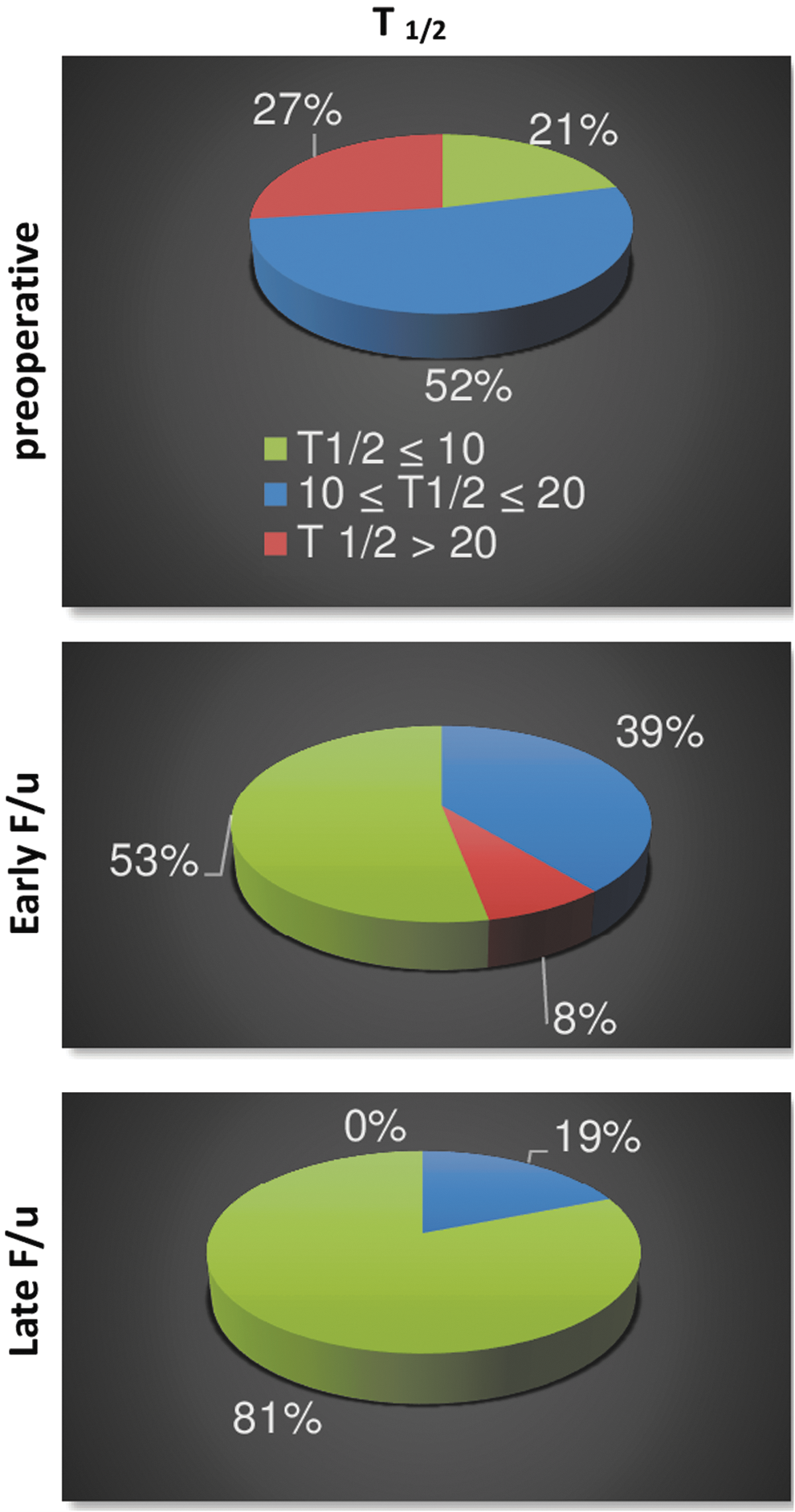
Percentage of nonobstructive (T1/2 ≤ 10 min), equivocal (10 min ≤ T1/2 ≤ 20 min), and obstructive (T1/2 > 20 min) diuretic half-time after i.v. furosemide administration on preoperative, early postoperative, and late postoperative diuretic renography.
Of note, 21.4% of preoperative renograms showed a T1/2 of ≤10 minutes despite symptomatic, sonographic, and radiographic confirmation of UPJO. We hypothesize that, in these patients, UPJO has a dynamic component and occurs periodically (as do the symptoms) and that the nonobstructed DRG reflects a temporarily undisturbed urine flow.
Four to six weeks after RALP, all eligible patients returned for removal of their Double-J stents. Early follow-up and DRG were performed the day after stent removal. Perioperative complications were classified according to Clavien–Dindo and amounted to 21.3% (16/75) (CD I-II-III). These complications were mainly minor and Double-J stent related (Table 2).
The mean time to late follow-up was 19.9 months; it could be obtained in 56 patients. 98.7% (74/75) reported no or only very mild and rare symptoms (patient pain analog score was 0 or 1) at their last follow-up, while 92% showed no or only mild hydronephrosis of the operated kidney on ultrasound. No patients had pyelonephritis or renal colic after RALP, and all patients appreciated the individual cosmetic outcome of RALP.
Postoperatively, no patient was obstructed on the late follow-up DRG (T1/2 ≤ 20 minutes), while five patients (8.2%) still showed obstruction on early DRG the day after stent removal.
DRG results were equivocal (10 < T1/2 ≤ 20 minutes) in 19.2% of patients at late follow-up, while at early follow-up, DRG was still equivocal in 39.3%. Thus, our overall success rate was 80.8% based on the strict criteria we applied to postoperative DRG and symptom score (Figure 1).
The increase in the rate of nonobstructed DRGs from 21.4% to 80.8% was mirrored by a decrease of high-grade hydronephrosis (II° or III°) from initially 78.7% to 8% at late follow-up.
Equivocal early DRG (10 < T1/2 ≤ 20 minutes) improved to unobstructed late DRG (T1/2 ≤ 10 minutes) in 57.9% of the cases and stayed equivocal in 42.1%. However, there was no deterioration to obstruction on late DRG.
Most notably, nonobstructed early postoperative DRG stayed nonobstructed at late follow-up in 95.7% of the cases. Only one DRG worsened to equivocal. However, this patient was symptom free and showed no sonographic signs of obstruction.
Of the five patients who had an obstructed early DRG, one showed a nonobstructed DRG, another one an equivocal DRG on late follow-up. Both patients were symptom free. Unfortunately, the other three patients were lost to late follow-up; however, all had complete symptom resolution and were unobstructed on ultrasound at early follow-up.
There was no statistically significant change in GFR (+0.13%) or serum creatinine levels (−10.1%) between preoperative and late follow-up, while T1/2 improved significantly (p = 0.014) by 45.8% ± 29.4%.
Discussion
The goals of pyeloplasty are to reconstitute nonobstructed transport of urine from the renal pelvis to the upper ureter to prevent further renal parenchymal damage and relieve patient symptoms. The introduction of robotic technology for complex reconstructive surgery has helped decrease some limitations associated with laparoscopy by providing a magnified three-dimensional view, eliminating tremor, enhancing surgeon comfort, and using instruments that mimic genuine hand and wrist movements. RALP can be performed safely with a low rate of significant complications, even in complex cases. There are several retrospective single-center series with patient numbers between 50 and 134 and a mean follow-up between 11.7 and 39.1 months that report excellent success rates of above 90%. 2 –4,13 The average operative time and complication rates in our series were similar to recently published studies. We used the Clavien classification for complications, thereby enabling future investigators to properly contrast their complication rates with our rates.
In general, the definition of success and adequate follow-up for robotic pyeloplasty is still being debated. In fact, some currently published pyeloplasty success rates for UPJO may be confounded by both insufficient follow-up and an inappropriate definition of success.
In our study, we based the definition of overall success on DRG with T1/2 ≤ 10 minutes plus symptomatic relief with a validated pain analog score of 0 or 1. Thus, we calculated our success rate as 80.8% which is lower than success rates that have been previously reported, 2 –4,13 probably due to the use of a strict definition of success.
There is substantial variation in the literature concerning the definition of success based on DRG. Some studies define surgical success as an improvement of DRF, while others rely solely on unspecific criteria, such as “a faster tracer washout,” without the use of defined diuretic half-time (T1/2) thresholds. 2 –4
On DRG, the diuretic half-time T1/2 (time at which the time–activity curve decreases to half of its activity at the time of lasix administration) following furosemide administration is widely recognized as the most sensitive and specific parameter to detect obstruction of the collecting system. T1/2 is best measured from the point of response to furosemide. The response to intravenous furosemide administration usually begins 1 to 2 minutes after injection, but maximum diuresis in some patients may not be reached until 15 minutes. There is a general consensus that promptly clearing the tracer from the renal collecting system after i.v. administration of furosemide with a T1/2 not over 10 minutes excludes obstruction. 14 According to the Radionuclides in Nephrourology Group—Consensus Committee on Diuresis Renography, 7 T1/2 greater than 20 minutes is abnormal and is associated with high-grade obstruction. Clearance half-times between 10 and 20 minutes are considered equivocal or indeterminate, and the patient should be followed closely. In many cases, the half-time may remain in the equivocal range for at least 6 months after pyeloplasty. 14 However, a prolonged T1/2 should not be the sole criterion upon which a determination of obstruction is based; information regarding pain resolution provided by patients should be considered. Therefore, recent publications advocate that an overall success rate be based on diuretic renogram with T1/2 ≤10 minutes plus symptomatic relief with a validated pain analog score.
Pouliot and colleagues were the first to apply similar criteria after laparoscopic pyeloplasty and defined scintigraphic success as strict (T1/2 < 10 minutes), nonobstructive (T1/2 < 20 minutes), and technical success (improved T1/2). 9 While clinical success (absence of symptoms) was achieved in 95% of cases, strict and nonobstructive successes were obtained in only 61% and 86%, respectively, showing a poor correlation between symptoms and obstruction. Similarly, Madi and colleagues reported 35 laparoscopic pyeloplasties with at least 1-year radiographic follow-up. 11 DRG was obtained at 3 weeks and interpreted as nonobstructed with a T1/2 < 15 minutes and obstructed with a T1/2 > 20 minutes. In equivocal cases, DRG was repeated after 3 months, 1 year, and variably thereafter. While seven patients had early failure (T1/2 > 20 minutes), only three patients progressed to failure thereafter (2, 2.5, and 6 years).
Etafy and colleagues reported 61 RALP patients with a mean follow-up time of 19 months 8 and were the first to use a strict definition of success with a T1/2 < 10 minutes and complete symptomatic relief using a validated pain analog score. Four cases failed by 3 months (T1/2 > 20 minutes). Seven cases failed from 18 months onward. These cases were initially considered only improved and not cured (T1/2 between 10 and 20 minutes, i.e., equivocal) because they did not meet the strict success criteria from the start. The authors suggested that a 3-month cure rate would be similar to the rate at 3 years or longer only when reproducible, stringent criteria for success are used.
With respect to these recent studies, we applied the criteria for effective postoperative renographic control as suggested by the Consensus Committee on Diuresis Renography and report a success rate of 80.8% comparable to Etafy and colleagues (81%).
With the definition of success being absence of symptoms and T1/2 not over 10 minutes on DRG, it remains unclear when DRG can reasonably be performed and repeated in patients after robotic pyeloplasty. This question is relevant with respect to radiation exposure and healthcare costs.
The average radiation exposure of a DRG with 99m-technetium is 5 mSv, compared with an average yearly exposure to natural background radiation of 3.1 mSv in the United States. The cost of a DRG may vary due to regional differences but is usually in the range between 500 and 900 U.S. dollars. However, in addition to cost and radiation exposure, patient compliance with follow-up protocols may be a problem.
In a recent review, Hsi and colleagues showed that the use of imaging for follow-up decreased dramatically beyond 1 year after pyeloplasty in published series. Approximately half of patients did not undergo radiographic follow-up after the first postoperative year. 6 DRG was not commonly used in patients who continued follow-up after 1 year. The authors concluded that although reported success rates in the literature were high, true success rates may be overestimated because of short follow-ups and underdiagnosis of asymptomatic failure based on imaging. In fact, late failures beyond 2 years have been reported. Dimarco and colleagues reported long-term laparoscopic pyeloplasty success rates of 80% and 75% at 5 and 10 years, respectively. 10 They concluded that laparoscopic pyeloplasty failure could continue to develop even after 5 and 12 years postoperatively. 10 In that series, initial success rates were 95% but dropped to 80% when examined 5 years postoperatively.
In light of these recent studies, we felt it appropriate to apply the strong criteria for effective postoperative renographic control as suggested by the Consensus Committee on Diuresis Renography and to perform a reassessment at a later stage. Based on our results, it may be feasible to perform an early DRG the day after stent removal when patient motivation is still high and early failure detection is important. All but one patient with an unobstructed early DRG also had a nonobstructive late DRG, and only one changed to equivocal. The majority of equivocal early DRGs usually improved to unobstructed on late DRG, but 42.1% remained equivocal.
We concluded that given complete symptom resolution, a nonobstructive diuretic clearance of ≤10 minutes on early DRG immediately following stent removal renders further renographic follow-up unnecessary, and monitoring by other means is sufficient. By contrast, patients with an equivocal early DRG require a further renographic follow-up.
However, due to losses in follow-up, we cannot give recommendations as to how to proceed with patients with an obstructed early DRG. Of note, the two patients who could be followed improved to nonobstructed and equivocal at late follow-up.
Limitations of this study are that data were collected retrospectively and that the mean time to late follow-up was 19.9 months although late failures beyond 2 years have been described in the literature. In fact, patients in this study are still under surveillance and will be monitored if ever possible.
Conclusion
In case of complete symptom resolution, a nonobstructive diuretic half-time of ≤10 minutes on early DRG the day after stent removal renders further renographic follow-up unnecessary. By contrast, patients with an equivocal early DRG (T1/2 between 10 and 20 minutes) require further scintigraphic follow-up until nonobstruction is reached.
Footnotes
Author Disclosure Statement
No competing financial interests exist.