
Abstract
Introduction:
Multifocal and hereditary kidney cancers often require repeated ipsilateral nephron sparing procedures with higher blood loss and complication rates compared to first time renal surgery. Consequently, many surgeons avoid minimally invasive techniques in the setting. We present the characteristics, complications, and short-term renal functional outcomes of patients who underwent a repeat robotic partial nephrectomy (rRPNx).
Materials and Methods:
A database was retrospectively reviewed to identify patients who underwent robotic partial nephrectomies between January 2007 and December 2013. Selection criteria for the rRPNx cohort included patients who had undergone at least two ipsilateral renal surgeries, with the second procedure being an rRPNx. All other patients comprised the initial robotic partial nephrectomy (iRPNx) group.
Results:
One hundred twenty-four patients who underwent robotic partial nephrectomy during the study period were identified. rRPNx constituted 26 (21%) of the total cases. Age of the rRPNx cohort was similar (p = 0.56), but number of tumors resected was two-fold greater in the rRPNx group (p = 0.44). Neither surgery time nor renal clamp time was significantly longer in either group (p = 0.18 and p = 0.65, respectively). Importantly, estimated blood loss (EBL) was significantly larger than in the iRPNx group (p = 0.01). Both groups had similar intravenous pain medication administration durations (p = 0.32), but postsurgical length of stay was greater for the rRPNx patients (p = 0.011). There were no significant differences in clavian complication rates (p = 0.17–0.39), with the exception of urine leak which occurred more frequently in the rRPNx group (p = 0.01). There was no difference in percent change in serum creatinine or estimated glomerular filtration rate (p = 0.89 and p = 0.67, respectively).
Conclusions:
rRPNx is safe and feasible in select patients. EBL, postoperative lengths of stay, and urine leak were the only factors significantly associated with rRPNx compared to iRPNx. Patient 3-month follow-up revealed excellent and comparable outcomes between the two groups.
Introduction
P
Materials and Methods
Study sample and design
We performed a retrospective review of our prospectively maintained database to evaluate patients who had undergone robotic partial nephrectomies on various institutional review board-approved protocols between January 2007 and December 2013 at the National Institutes of Health. One hundred twenty-four consecutive patients who met this inclusion criterion were identified. Patients with a prior history of one or more ipsilateral renal or adrenal surgeries were included in the rRPNx cohort. All other patients comprised initial robotic partial nephrectomy (iRPNx) group.
Study variables
Patient demographics and preoperative renal function data were reviewed. Operative variables included number of tumors resected, surgery time, estimated blood loss (EBL), and use of renal ischemia. Postoperative renal function was assessed using serum creatinine and estimated glomerular filtration rate (eGFR) during the recovery period and at 3-month follow-up. The Chronic Kidney Disease Epidemiology Collaboration equation was used to calculate eGFR. 7 The numbers of days of postoperative intravenous (IV) analgesia were documented, as was postoperative length of hospital stay. Complications were recorded and classified using Clavien classification system.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 21® software (IBM, Chicago, IL). Mann–Whitney U test was used to compare distribution of continuous variables. Pearson Chi square and Fisher's exact tests were used to compare proportions of categorical variables. Statistical significance was defined as p < 0.05.
Results
Perioperative characteristics
One hundred twenty-four patients underwent robotic partial nephrectomy at the National Institutes of Health during the study period. Of those, 98/124 (79%) and 26/124 (21%) underwent iRPNx and rRPNx, respectively. Of those patients in the rRPNx group, 22 were second time cases, while four were third time cases (Fig. 1). Sixteen (62%) patients in the rRPNx cohort had a history of previous open ipsilateral surgery, while 10 had previous minimally invasive ipsilateral procedures, four of which were thermal ablation.

One hundred twenty-four patients who had undergone robotic partial nephrectomy were selected. Ninety-six patients composed the iRPNx group, while 26 composed the rRPNx group. iRPNx, initial robotic partial nephrectomy; rRPNx, repeat robotic partial nephrectomy.
Median age for the rRPNx and iRPNx group was 47.0 (range: 28–75) and 47.5 (19–83) years, respectively (p = 0.56). There were no significant differences in the clinical characteristics between patients when comparing the rRPNx and the iRPNx cohorts (Table 1).
The only statistically significantly different variables between the two groups were EBL and LOS (p = 0.01 and p = 0.01, respectively).
rRPNx = repeat robotic partial nephrectomy; iRPNx = initial robotic partial nephrectomy; AA = African American; BMI = body mass index; Cr = creatinine; eGFR = estimated glomerular filtration rate; EBL = estimated blood loss; IV = intravenous; LOS = length of stay.
Median surgical time was comparable between the rRPNx and iRPNx groups (359.5 minutes vs 317.0, respectively; p = 0.18). Median number of tumors resected in the rRPNx group was 3 (1–29), while it was 1.5 (1–52) in the iRPNx group (p = 0.44) (Table 1). EBL was significantly higher (p = 0.01) for the rRPNx group compared to iRPNx (900.0 vs 500.0 mL, respectively) (Table 1). Renal hilar clamping was used in 44.4% of all patients with the median clamp time of 28.0 minutes (14–120). No differences in proportion of patients in each group clamped or in clamp times were found (p = 0.52 and p = 0.65, respectively). No cold ischemia was used (Table 2).
No statistically significant differences exist between the iRPNx and rRPNx group.
Patients undergoing rRPNx required IV pain medications for a similar number of days as the iRPNx group (median 2.0 days for each rRPNx and iRPNx groups, p = 0.32). In terms of length of hospital stay, it was significantly longer for the rRPNx group; 10.0 days vs 8.0 for the iRPNx group (p = 0.01) (Table 1).
Genetic characteristics
Of all the patients, 57.3% (71/124) were found to have a germline mutation, while 42.7% (53/124) were sporadic cases (p = 0.35). Of patients in the iRPNx group, 46.9% (46/98) had hereditary disease, while 73.1% (19/26) of the rRPNx group had identifiable hereditary disease (p = 0.07). No significant differences in the proportion of patients within each group that presented with a specific familial syndrome existed (p = 0.07–0.70) (Table 3). Of patients in the iRPNx group, 32.7% had a single tumor removed where no germline alteration was identified, while only 15.4% of patients in the rRPNx group had a solitary mass resected with no identifiable germline mutation (p = 0.06) (Table 4). Genetic analysis of tumor tissue found that 46.2% of the rRPNx group had ≥3 tumors excised secondary to an identifiable germline alteration. Conversely, only 28.6% in the iRPNx group had ≥3 tumors removed secondary to an identifiable germline alteration (p = 0.14).
Further substratification in those with germline alterations by familial syndrome.
No statistically significant differences between the iRPNx and rRPNx group were found, although the proportion of rRPNx patients with germline alterations and the proportion of patients with VHL approach significance in comparison to the iRPNx group.
VHL = Von Hippel–Lindau; BHD = Birt–Hogg–Dube; HPRC = hereditary papillary renal cell; HLRCC = hereditary leiomyomatosis renal-cell carcinoma.
No differences between the iRPNx and rRPNx group were found, although the proportion of patients with no germline alteration identified and only one tumor resected in the iRPNx group compared to the rRPNx group approached significance.
Complications
Overall rate of complications using Clavien classification system was 57.7% (15/26) in the rRPNx group vs 37.8% (37/98) for the iRPNx (p = 0.07) (Table 5). There were no Clavien IV or V complications and no loss of renal units reported for either group. Of those patients who underwent rRPNx, 5/26 (19.2%) developed urine leak vs 3/98 (3.1%) in the iRPNx group (p = 0.01) (Fig. 2). Two out of three (66.67%) patients with urine leak in the iRPNx group required stent placement (Clavien III) vs 3/5 (60%) in the rRPNx group. Transfusion rate was 15.3% for iRPNx vs 19.2% for rRPNx patients (p = 0.76) (Table 5).
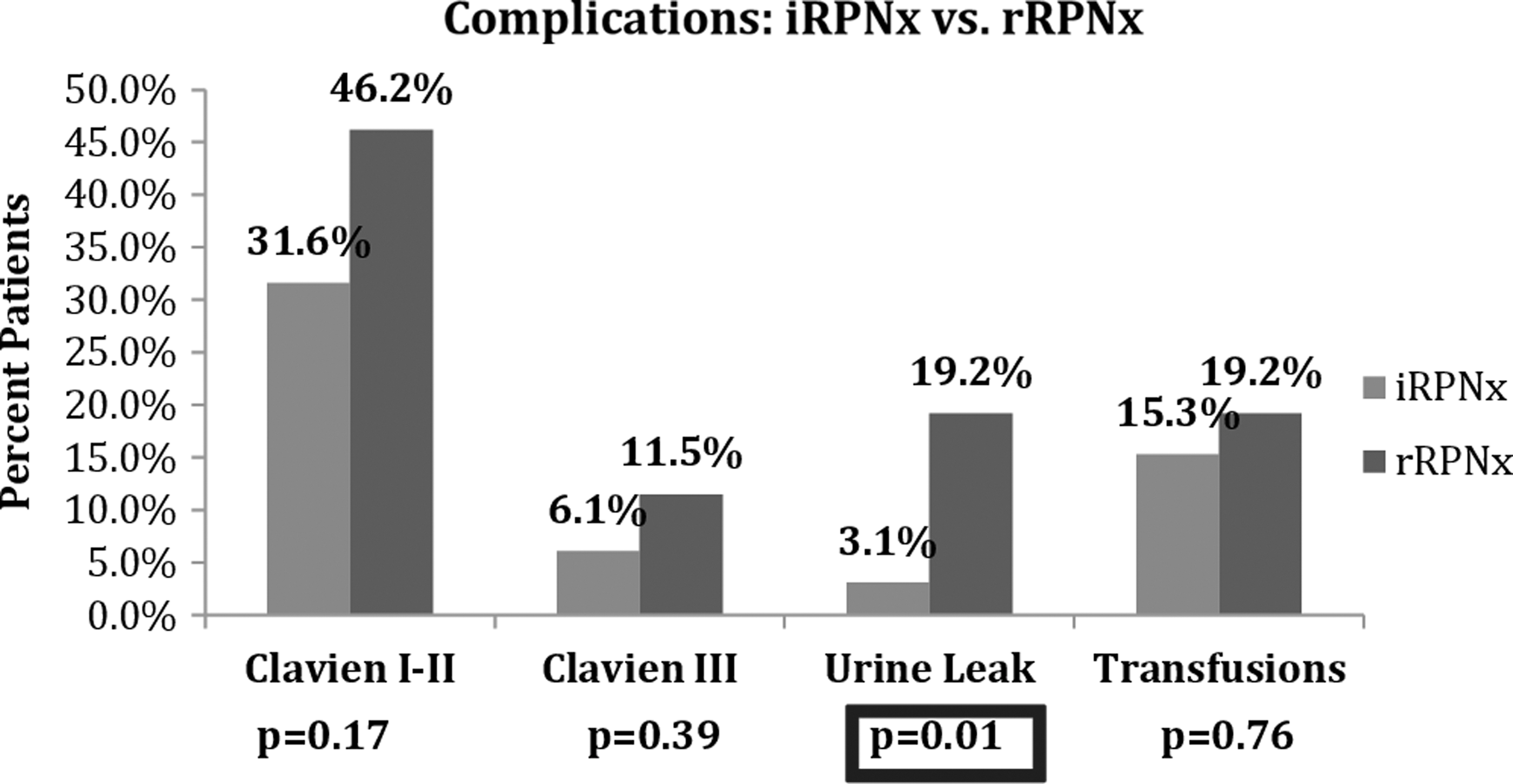
Comparing complications between the iRPNx and rRPNx groups. No statistically significant differences were found between Clavien complications; however, urine leak was statistically higher in the rRPNx group (p = 0.01).
The only statistically significant variable between the two groups was urine leak (p = 0.01).
SVT = supraventricular tachycardia; SOB = shortness of breath; JP = Jackson-Pratt drain.
Patients with Clavien II or greater complications had longer surgery time (414.22 vs 306.10 minutes, p = 0.001), higher blood loss (1454.44 vs 716.48 mL, p = 0.001), but lower median number of tumors resected at time of repeat procedure (36 vs 88, p = 0.001).
Overall conversion rate to open nephrectomy was 8.9% (10/124); 15.4% (4/26) for those undergoing rRPNx vs 7.1% (7/98) in the iRPNx group (p = 0.19).
Renal function outcomes
There was no significant difference between median serum creatinine levels at preop and at 3-month follow-up (p = 0.27) (Table 6). Median percent increase of creatinine levels in rRPNx patients was 5.0% (−28% to 94%), while the iRPNx patient's creatinine also increased 5.0% (−42% to 65%) (p = 0.89). Furthermore, median percent change between the rRPNx cohort's preop and 3-months follow-up eGFR was −5.21% (−39.50% to 24.66%), while it was −4.7% (−49.9% to 57.41%) in the iRPNx group (p = 0.41).
There were no statistically significant differences in variables between the two groups.
F/U = follow-up.
Discussion
Nephron sparing surgery is now recommended as the gold standard for the treatment of small renal masses and has expanded to include larger renal tumors according to expert panels. 8 –10 However, one of the challenges lies in managing patients who, due to the multifocality and bilateral nature of the disease, will present with recurrent masses or de novo tumor formation. This accounts for as much as 17% of patients undergoing partial nephrectomy. 11,12
Several treatment options are available for these patients, including radical nephrectomy, ablation, repeat open partial nephrectomy, and rRPNx. Repeat partial nephrectomy allows maximum preservation of renal function and can help avoid dialysis, while maintaining comparable oncological outcomes as radical nephrectomy and open partial nephrectomy. 12 –15 However, these repeat procedures are often more challenging due to the presence of fibrosis and scarring of the normal tissue planes. For these reasons, even in experienced hands, the procedures are often prolonged depending on the number of tumors resected. 3,16
Individuals differ tremendously in how kidneys respond to prior surgical intervention. As such it is difficult to predict the degree of intraperitoneal adhesions and peri-renal scarring a priori. This significantly contributes to the wide range of lengthy operating times seen in this series. Previous data from our institution and others have shown that “severe fibrosis” is commonly encountered during repeat surgery after thermal ablation. 17,18 Similar surgical challenges have previously been reported for open and laparoscopic surgery following previous renal surgery. 2,3,6 In our experience, the robotic approach to these challenges is similar, if not identical, to that of open surgical techniques used to address dense scarring around the kidney and vasculature. For example, isolation of individual vessels at the renal hilum is often eschewed in favor of en bloc mobilization and en bloc clamping of the hilum if indicated. In addition, the use of sharp dissection around the vasculature and cautery elsewhere to manage dense scar tissue may be performed, as would be done during open surgery.
Surgical times were 40 minutes longer in the rRPNx group compared to the iRPNx group (p = 0.18). More generally, we acknowledge that even for iRPNx for a solitary tumor our reported surgical times are longer than other series in the literature. 19 There are several factors which dictate operative time such as extent of adhesions, complexity of tumors, fellow/resident involvement, disease process, clamping, and other patient specific factors such as previous nonrenal abdominal surgeries and obesity. All these factors might have contributed toward the longer operative times in our cohorts. We did not analyze our operative times as a function of learning curve because the numbers in the study are small. However, previously published data from our institution do demonstrate the effect of the learning curve on conversion rate from robotic to open and number of tumors resected. 20 Larger patient cohorts will permit such an analysis in the future. However, the longer operative time in the rRPNx group is likely to be a reflection of the higher number of tumors removed in that group.
Twice the number of tumors were removed from the rRPNx group compared to the iRPNx group (3 vs 1.5, respectively, p = 0.44). This may be explained by the relative proportions of patients in each group with familial cancer (Table 3). Over 73% of the patients in the rRPNx group had identifiable hereditary disease compared to less than half of patients in the iRPNx group. For instance, the proportion of rRPNx patients presenting with Von Hippel–Lindau was 61.5% compared to 33.7% of those in the iRPNx group (p = 0.08). As such, the relatively high proportion of hereditary disease in the rRPNx group may account for the greater median number of tumors removed in the rRPNx group compared to the iRPNx group. Indeed, half the proportion of patients in the rRPNx group had a single tumor with no germline alteration identified compared to the iRPNx group (p = 0.06) (Table 4). Conversely, almost double the number of patients in the rRPNx group had ≥3 tumors with an identifiable germline alteration compared to the iRPNx group (p = 0.14). It has been suggested that the application of the unique features of robotic technology may provide the surgeon with better resources to address many of the challenging issues associated with these repeat procedures. Autorino and associates reported their experience with nine rRPNx patients. 21 They demonstrated feasibility of the rRPNx with no intraoperative complications. Furthermore, they reported only two Clavien I postoperative complications and showed only a 7% decrease in eGFR from preoperative level in their patients. 21 Furthermore, both Kowalczyk and coworkers and Johnson and coworkers report postoperative complication rates of 50% and 43.2%, respectively, in their series of open repeat partial nephrectomies (oRPNx). 2,17 The overall complication rate for this series is comparable to the repeat open series previously reported.
Our series presents 26 patients who underwent rRPNx, which demonstrates the feasibility of the procedure in experienced hands with comparable complication rates compared to open series. While the complication rate in rRPNx was higher than iRPNx in our cohort, it did not reach statistical significance (37.8% vs 57.7%, respectively, p = 0.07) (Table 5). In addition, most of the complications reported were Clavien I–II (not requiring any surgical interventions). The most frequent complication seen in our study was urine leak, which occurred in 19.2% (5/26) patients in the rRPNx group, and was the only complication to be significantly higher in the rRPNx group (p = 0.01) (Fig. 2). Of these, three required stent placement. This is also comparable to the oRPNx series in which urine leak rates reported ranged from 15% to 20%. 3,22 Furthermore, a recent retrospective analysis of 1082 patients found that an increasing number of ipsilateral mass excisions were associated with a higher overall complication rate. 23 On multivariable analysis, number of excisions independently predicted complications (OR 3.1, 95% confidence interval 1.03, 9.33, p = 0.041). A median number of 1.5 and 3.0 masses were removed from the iRPNx and rRPNx group, respectively. The increased number of masses removed may have influenced our complication rate.
The second most common complication for the rRPNx group was transfusion with a rate of 19.2% (5/26) (Table 5). EBL in the rRPNx group was almost double that of the iRPNx group (900.0 mL vs 500.0 mL, respectively, p = 0.01) (Table 1). The increased EBL can be explained by the complexity of the procedures and the off-clamp technique. Repeat surgeries are often performed on fibrotic and scarred tissue. The amount of scarring experienced in these cases is highly variable. Some cases may have minimal adhesions allowing for the dissection to proceed at a pace of initial surgery, while in other cases the scarring is intense, resulting in significant time spent in mobilizing colon and kidney. Typically, hilar dissection is more complex, resulting in longer times spent in isolating the renal vessels. Therefore, a more convoluted tissue dissection results in tearing of the microvasculature. In addition, a recent study showed that patients with previous abdominal surgery lost 50% more blood during robot-assisted partial nephrectomy than those patients who did not have a prior abdominal surgery (p = 0.039). 24 As such the iRPNx experienced by those patients in the rRPNx group may, in part, contribute to the greater EBL. Furthermore, approximately half of the rRPNx cases were performed without any hilar clamping, which may account for the increased EBL and, thus, higher transfusion rates. However, in the repeat open series by Johnson and coworkers, the overall EBL of 2400 mL and transfusion rate of 64.7% were substantially higher than the 145 mL and 19.2% transfusion rate in our series. 2 Furthermore, the series reported by Bratslavsky and associates had an average EBL of 1200 mL greater than ours. 6
No significant differences were found in median clamp time between the two groups (p = 0.65) (Table 2). However, the median initial iRPNx clamp time (30.0 minutes) may be skewed compared to the rRPNx clamp time (21.5 minutes) due to an unusual and unfortunate clinical situation. The 120-minute clamp time was a result of an unrecognized, unclamped ischemic time secondary to a disrupted renal artery plaque. This ultimately required an intraoperative renal artery endarterectomy once the ischemia was identified. One hundred twenty minutes was an estimate of the elapsed time between the initial hilar renal occlusion and the completion of the endarterectomy. Clearly this is not a reflection of our normal operative technique. It is an outlier which is nearly twice as long as the next longest recorded time. In addition, this was one of the few cases that were converted from robotic to open. This patient's most recent creatinine was 0.95, with 30% function in that renal moiety on nuclear renography, 3 months postoperatively.
Overall complication rates tend to be higher for repeat procedures, and indeed, our series found that rRPNx patients had increased length of stay (LOS) compared to iRPNx patients (Table 1). Autorino and associates reported a median LOS of 3 days (3–5) for their rRPNx group (16). 21 Our median LOS was 10.4 days for the rRPNx and 8.7 days for the iRPNx group (p = 0.04). This extended LOS is a result of two factors unique to our institution. First, the patient population of the National Institutes of Health has a large population of patients with hereditary and multifocal renal-cell carcinoma; thus the complexity of the surgeries is increased as evidenced by the greater number of tumors removed per case compared to Autorino and coworkers (median 3 vs 1 tumor). 21 Furthermore, a majority of patients travel to our institution from outside the immediate area, so our conservative postoperative care and discharge planning result in a substantially longer hospital stay compared to institutions with a local patient catchment area. The slightly longer LOS for our rRPNx patients compared to the iRPNx group is expected considering that these are challenging procedures with higher rate of postoperative complications.
In terms of renal functional outcomes, our series reported good preservation of renal function at 3-month follow-up for the rRPNx group (Table 6). Median percent change in creatinine at 3-month follow-up was 5.0% (−28% to 94%), while median percent decline in eGFR was 5.2% (39.50% to 24.66%), neither of which was significantly different from the iRPNx group. Of note, there were no loss of renal units and no need for dialysis in our rRPNx group. These results are comparable to Autorino and coworkers' published rRPNx series in which they report a 7% decrease in eGFR postoperatively, no loss of renal units, and no patients requiring hemodialysis. 21 However, we report on the renal functional outcomes on over double the number of patients as they do. Furthermore, in Johnson and coworkers' open repeat series, the decrease in eGFR appears to favor our rRPNx series (5.2% vs 10.7%) as does the rise in creatinine (0.03 vs 0.19 mg/dL) and rate of patients requiring hemodialysis (0% vs 5.9%). 2 These differences between open and robotic repeat procedures may reflect a selection bias that could be confirmed in a prospective randomized trial.
Limitations of this study include the inherent bias associated with the retrospective nature of the study. Furthermore, this study represents our initial experience with rRPNx and, thus, contains a relatively small sample size so statistical power is limited. For example, although the total patient complication rate is higher in the rRPNx group compared to the iRPNx group, the difference between these two did not reach statistical significance. Another limitation of this study is its broader applicability given the unique patient population from our institution. Nevertheless, these findings provide important information on safety and feasibility of rRPNx in patients with solitary or multiple renal tumors.
Conclusions
rRPNx is a safe and feasible procedure when performed by experienced robotic surgeons in highly selected patients. Compared to our iRPNx group, LOS is longer and complications rates tend to be higher for rRPNx, but most are Clavien I–II. At 3-month follow-up, renal function preservation is excellent with respect to preoperative levels and is comparable to iRPNx patients.
Footnotes
Acknowledgment
This research was supported by the Intramural Research Program of the NIH, National Cancer Institute, Center for Cancer Research.
Author Disclosure Statement
No competing financial interests exist.