
Abstract
Introduction:
To evaluate the efficacy of laparoscopic pyeloplasty (LPP) for lower functioning kidney, we investigated the outcome of this procedure for patients with ureteropelvic junction obstruction with decreased renal function, defined as less than 20% split renal function.
Patients and Methods:
Between October 1998 and June 2015, we performed transperitoneal dismembered LPP in 224 patients. Among them, 15 patients with less than 20% split renal function were included in this study. Patient characteristics, perioperative split renal functions, complications, and surgical outcomes were retrospectively investigated.
Results:
Fourteen of 15 patients had preoperative symptoms, including flank pain in 13 patients and gross hematuria in 1 patient. Preoperative 99mTc-mercaptoacetyltriglycine (MAG3) renogram revealed no response to diuretic injection and median split renal function was 16.5%. Median operative time and blood loss were 170 minutes and 20 mL, respectively. There were no complications during the perioperative period. Postoperative MAG3 renogram at 6 and 12 months after the operation revealed significantly increased split renal function (median: 23.8% and 23.7%, p = 0.001 and 0.008, respectively) and response to diuretic injection in all patients. Preoperative symptoms disappeared and no recurrence was seen during the follow-up period for all patients except for one who experienced flank pain again 4 months after the surgery. He subsequently underwent open pyeloplasty, and flank pain disappeared soon after.
Conclusions:
LPP for patients with low split renal function and flank pain significantly improved symptoms and split renal functions. Although the long-term clinical effects of LPP are unknown, we recommend performing LPP before considering nephrectomy for patients with lower functioning kidney.
Introduction
U
Recently, minimally invasive surgeries, including laparoscopic pyeloplasty (LPP) and robot-assisted LPP, have been gradually favored instead of open procedures. Laparoscopic procedures are reported to be less invasive and equivalent to surgical outcomes compared to open procedures. 4 –7 One of the major indications for pyeloplasty is decreased renal function on the affected side. Although the indication for surgical treatment is based on less than 40% split renal function or more than 5% decrease of affected renal function during follow-up periods using 99mTc-mercaptoacethyltriglycine (MAG3) renogram or 99mTc-diethylenetriaminepentacetate renogram in many reports, there are no substantial reasons for these indications. 8,9
To our knowledge, there are no reports that describe indications for performing LPP in terms of the lower limit of decreased renal function. Because preservation of a severely dysfunctioning kidney would cause hypertension, proteinuria, or chronic urinary tract infections, nephrectomy should be considered in those cases. 10,11 However, it is unclear when physicians need to perform nephrectomy in patients with decreased renal function and when they need to decide to perform LPP, especially in patients with symptoms such as flank pain. To avoid unnecessary nephrectomy, we conducted LPP using the Anderson-Hynes technique in patients with severely decreased and affected renal function defined as split renal function less than 20% on MAG3 renogram. We report improved postoperative functional outcomes.
Patients and Methods
Between October 1998 and June 2015, 224 patients underwent transperitoneal dismembered LPP in our institute. Among them, 15 patients had less than 20% split renal function on the affected side and were included in this study. Function and morphology of the contralateral kidney in these 15 patients were normal when checked by MAG3 renogram and computed tomography. Preoperative symptoms were seen in 14 patients, including flank pain in 13 patients and gross hematuria in 1 patient. That remaining one patient had right hydronephrosis that was incidentally detected during an annual medical examination. Three patients who had severe flank pain preoperatively had a ureteral stent placed before LPP on the affected side.
Patient characteristics are summarized in Table 1. Two of the 15 were children. Ten of the 15 patients had high-grade hydronephrosis preoperatively. No one had a response to diuretic injection on preoperative MAG3 renogram, and the median split renal function on the affected side was 16.5% (range: 8.3–19.6%). The median period from developing flank pain to LPP or to preoperative ureteral stenting was 2.5 months (range: 0.2–28 months). LPP was performed according to the procedure described previously by two surgeons. 6 In brief, after careful dissection of the upper ureter and renal pelvis, a stay suture was placed in the medial edge of the renal pelvis just above the stenotic segment. This was pulled out through the abdominal wall using Endo-Close™ (Covidien Japan, Tokyo, Japan) and fixed with appropriate tension (Fig. 1). After insertion of a 6-F double pigtail stent in an antegrade manner, ureteropelvic anastomosis was performed in a running manner using 5–0 monofilament sutures with a one-half curved 13-mm needle. When anterior crossing vessels were seen, they were preserved and the ureter and pelvis were transposed. The double pigtail stent was indwelling for 4 weeks.
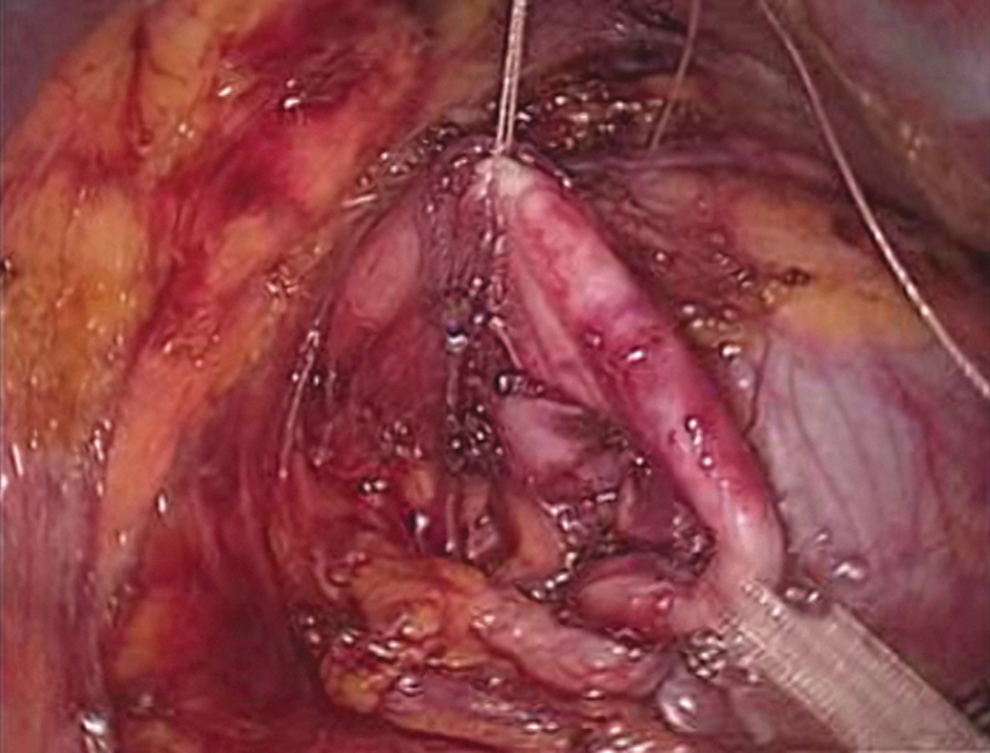
Left UPJ was taped and exposed. Dilated pelvis was pulled up to the abdominal wall by 4–0 absorbable suture.
We reviewed the intraoperative records and hospital charts of all patients to evaluate patient characteristics, intraoperative findings, complications, and surgical outcomes. All patients were subjectively followed up at our patient clinic. Patients were followed up at 1, 3, and 6 months, and then yearly thereafter. Postoperative symptoms were checked at every visit and intravenous pyelography was performed at 3 months after the operation to check the kidney configuration, enhancement, and flowage of contrast agent from pelvis to ureter. Renal ultrasound examination and diuretic renogram were obtained at 6 months and 1 year after the operation. Diuretic renogram was performed by a modified method in which infusion was done for 1 hour at 200 mL/hr before the renogram, and diuretic (furosemide; 20 mg) is given at 15 minutes after the start of the renogram. Success of operation was defined as improvement of symptoms, radiographic evidence of a patent ureteropelvic junction, and stable or improved renal function. 12
Statistical analysis was performed using the Mann–Whitney U test, Paired T test, and Pearson's chi-square test using Ekuseru-Toukei 2010 (Society Survey Research Information Co., Ltd., Tokyo, Japan). A value of p ≤ 0.05 was considered significant.
Results
Clinical outcomes are shown in Table 2. All patients underwent laparoscopic surgery. There was no open conversion. Median operative time was 170 minutes, and median blood loss was 20 mL. Crossing vessels causing UPJO were seen in four patients, and all of them were able to be preserved. In the remaining patients, intrinsic fibrosis of a ureteral segment caused UPJO. There was no complication during the perioperative period.
The median improved rate was 24.0% (range: −4.8 to 246.9%) at 6 months and 38.3% (range: −13.5 to 279.5%) at 12 months after surgery (Fig. 2). Renal scintigraphy at 6 and 12 months after surgery revealed significantly increased split renal function compared to preoperative one (median: 23.8% and 23.7%, p = 0.001 and 0.008, respectively). However, there is no statistical difference between 6 and 12 months after surgery (p = 0.06). We performed subgroup analysis to identify those most likely to benefit in terms of postoperative renal function. There is no statistical difference in terms of preoperative grade of hydronephrosis (Grade 4 or less than Grade 3, p = 0.08), preoperative ureteral stenting (p = 0.18), pediatric patients or adult patients (p = 0.07), and presence of crossing vessels (p = 0.19). Responses to diuretic injection were shown in all patients. At the last visit, three patients had high-grade hydronephrosis postoperatively, but their postoperative split renal function and kidney configurations were improved compared to those before surgery. Only one patient had high-grade hydronephrosis persistent, despite treatment. This patient had grade 4 hydronephrosis postoperatively and showed disappearance of preoperative symptoms and improvement of split renal function. Preoperative symptoms disappeared within 1 month after the operation, and no recurrence was seen during the follow-up in 14 of 15 patients; therefore, the success rate was 93.3%. One patient had flank pain 4 months after surgery. Intravenous pyelography in the standing and decubitus positions showed a floating kidney on the operated side. We subsequently performed an open redo pyeloplasty by excision of redundant ureter and detachments of renal fixation at 6 months after initial operation. His flank pain immediately disappeared after the second surgery.
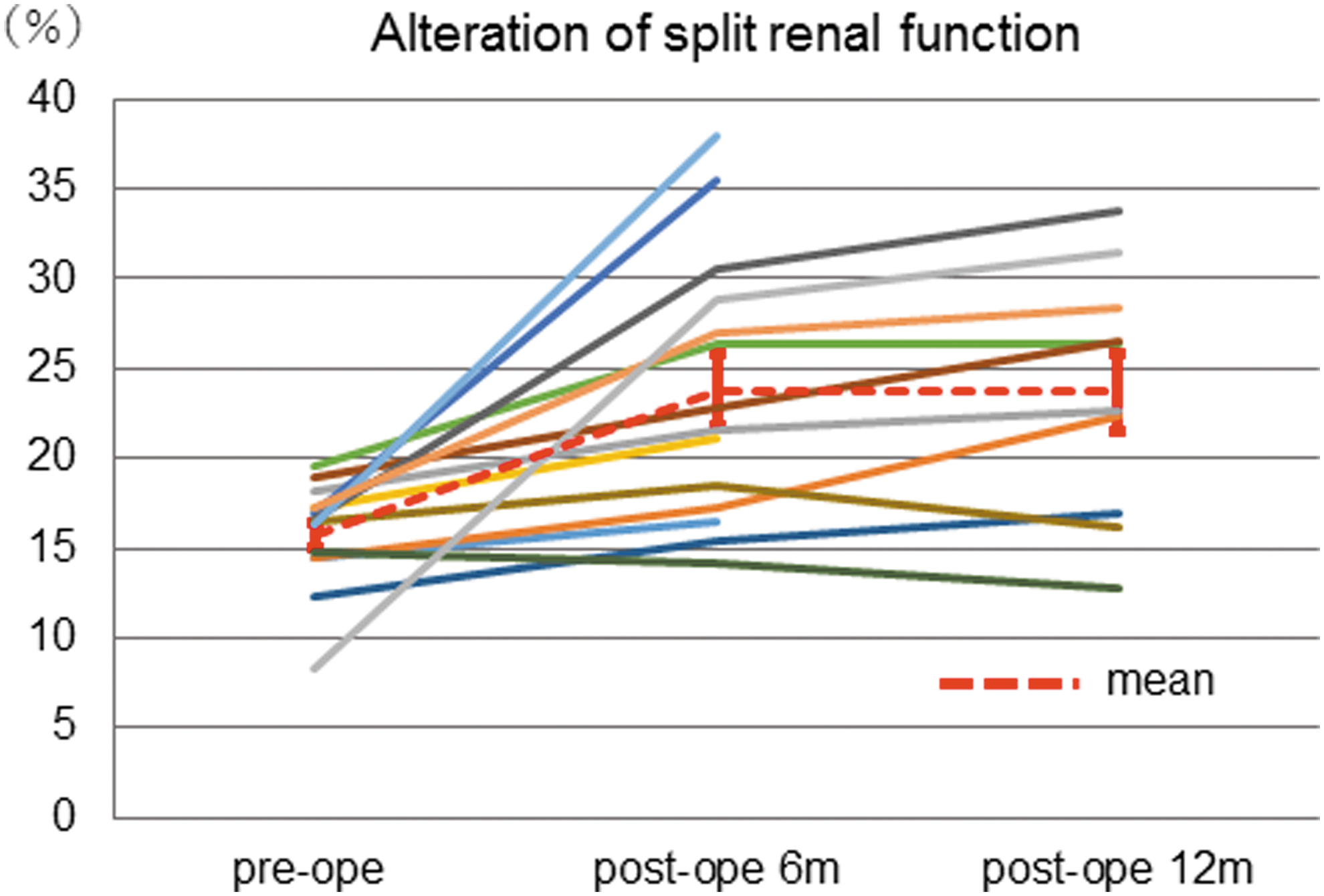
Split renal functions on the affected side were improved after 6 and 12 months after LPP. Median improvement rates were 24.0% and 38.3%, respectively. LPP = laparoscopic pyeloplasty.
Discussion
UPJO is the most common congenital abnormality of the upper urinary tract; it causes flank pain, gross hematuria, urinary tract infection, and deterioration of renal function. Because open pyeloplasty is traditionally performed, 1 –3 and because its success rate has been reported to be more than 95%, it is the gold standard of treatment for UPJO. However, as a result of newly developed medical appliances, less invasive therapies such as laparoscopic and robotic surgery have now become substitutes for open procedures. LPP was first introduced in 1993 by Schuessler and coworkers. 4 This procedure has emerged as an alternative first-line option with success rates similar to those of the open approach because of less usage of analgesic drugs, short hospital stays, and early return to societies. 4 –7 A randomized controlled trial, including 28 patients who underwent laparoscopy and 34 patients who underwent open surgery, was reported by Bansal and coworkers. 5 Although mean operative time in the laparoscopic group was longer than that in the open group (244 vs 122 minutes), patients treated with laparoscopic surgery showed significantly less need for diclofenac postoperatively and shorter hospital stays than those treated with open surgery. Autorino and coworkers reported a meta-analysis that showed no difference in terms of success and complication rates between the laparoscopic or robotic group and the open group. 13 According to the previous report, LPP is less invasive and has equal effect compared to the open procedure.
However, there were a few reports of pyeloplasty for patients with poorly functioning kidneys. Wagner and coworkers studied the results of pyeloplasty in 32 patients younger than 3 years. Four of the 32 patients had less than 10% split renal function preoperatively, and there was significant improvement of split renal function after the 1-year follow-up. 14 Bansal and coworkers reported long-term results of pyeloplasty in poorly functioning kidneys in pediatric patients. A total of 39 patients with less than 30% split renal function were included in that study, and patients were separated into two groups: group I (10–30%: mean 24.7%) and group II (<10%: mean 5.1%). The mean postoperative split renal function increased in 38.9% of patients in group I and 19% of patients in group II. They concluded that pyeloplasty provided good results for poorly functioning kidneys in the pediatric age group. 15 Ortapamuk and coworkers analyzed the factors responsible for improvement in postoperative renal function in the adult population. The recovery of postoperative split renal function depended on the preoperative level of split renal function, that is, patients with more than 30% split renal function; however, the length of time from first symptoms to operation was not described. 16 Regarding the recovery of the split renal function, this could be more likely in the pediatric population because of the flexibility of renal pelvic tissues, leading to the maintenance of low pressure in the pelvis. In addition, this could be in correlation with the duration from the first symptoms, most of which were flank pain. In this study, which included 13 adult patients, all postoperative split renal functions were statistically improved (p = 0.001). Twelve of the 13 adult patients had flank pain, and median duration from initial symptoms to operation in this study was 2.5 months. This short duration plays an important role in the improvement of postoperative split renal function, especially in the adult population. The patient with decrease in function by 4.8% at 6 months and 13.5% at 12 months after surgery was a 7-year-old child, and underwent MAG3 test in previous hospital at 5 months before surgery. The reasons for decrease in function postoperatively would be an already decreased function at surgery. In addition, preoperative large hydronephrosis diminished in size and the radio isotopes in background could not be included in postoperative region of interest.
Some reports described unilateral poorly functioning or nonfunctioning kidneys as a cause of hypertension. Schlomer and coworkers reported the outcomes of pediatric patients with unilateral renal parenchymal disease who underwent nephrectomy for hypertension. Fourteen of the 21 patients had resolution of hypertension, and they concluded that nephrectomy was a logical option of care that could be offered to patients with informed knowledge of the potential for cure. In their reports, only two patients had UPJO diagnosed. 10 To our knowledge, there is no report regarding how much worse renal function is if brought on by hypertension, and subsequent nephrectomy should be considered for patients with hydronephrosis. In our study, none of the patients had hypertension preoperatively and no one developed hypertension postoperatively during the follow-up periods. Our results suggest that patients with less than 20% UPJO and symptoms of flank pain should be initially treated with pyeloplasty, because these patients may have possible favorable outcomes. In addition, we recommend laparoscopic surgery because of its less invasiveness and same success and complication rates compared to the open procedure.
There are several limitations in this report. First, sample size was small and some of the data were missing. The postoperative follow-up period was ∼2 years, which is too short to investigate the incidence of hypertension and recurrence of symptoms. Second, the length of time from first symptoms to operation was not accurate and some selection bias existed because of the retrospective nature of this study. Two patients in similar clinical situations underwent nephrectomy during this time frame. However, those patients had asymptomatic hydronephrosis with single-digit severe decreased split function and strongly hoped to undergo nephrectomy. Finally, it is not clear how much the residual renal function, which was preserved by operation, affected patients' health. Although the answers to these questions need to be found with long-term follow-up, LPP could be one useful treatment option to consider before nephrectomy for patients with symptoms and a severe decrease in renal function. Because developments in minimally invasive surgery will lead to new choices for treatment, further studies are warranted.
Conclusions
LPP for patients with less than 20% split renal function and flank pain significantly improved symptoms without worsening split renal functions and any postoperative complications. Although the long-term clinical effects of LPP for the patients with lower functioning hydronephrosis are unknown, we recommend performing LPP before considering nephrectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.