
Abstract
Objective:
To quantify through environmental audit the radiation dose that urologists receive during surgery in the lithotomy position, and to quantify the dose reduction achieved by altering exposure techniques and personal protective equipment use.
Materials and Methods:
Simulated surgery in the lithotomy position using an anthropomorphic phantom as a patient and a SimMan® mannequin as the surgeon. Pulsed fluoroscopy, focus-to-skin distance (FSD), collimation, and addition of a lead shield at the table end were individually and collectively introduced after a control study. Scattered X-ray dose rates to the simulated surgeon's eye, thyroid, trunk, external genitalia, and leg were measured with each of the technique adjustments. The absorbed dose in air at the phantom skin was measured throughout. Results were compared to discover surgeon dose rates with technique alteration.
Results:
Increasing FSD leads to a rise in surgeon eye dose, and table end lead protection increases the patient skin dose. Use of all the dose-reduction techniques together reduces the dose to the patient, and a surgeon's trunk dose is decreased by 95%, external genitalia dose by 99%, and leg dose by 97%. Sitting to perform fluoroscopically guided surgery in the lithotomy position increases surgeon dose by a median value of 17%, with the external genitalia dose increased by 78% compared with the standing position.
Conclusions:
This study describes effective methods of dose reduction that are easy to instigate. The resulting reduction in radiation dose during urology procedures meets the requirements of international guidelines and legislation. This change in practice improves patient care and reduces risk to urologists from occupational exposure to radiation. By combining all of the dose-reduction techniques, urologists should never reach the threshold for deterministic radiation effects to their eyes during their career, and they will have a significantly lower chance of stochastic risks such as cancer.
Introduction
T
Occupational doses to surgeons are increasing with increasing patient size and case complexity. 3 Radiation protection techniques are often inferred from other specialties. With the patient in the lithotomy position, the surgeon is closer to the primary beam than colleagues performing cardiology or neuroradiology interventions. Inferences from such data to urology procedures should be with caution, as urologist dose rate may be greater.
Deterministic effects and stochastic effects from radiation exposure are always a concern, though the published data debate the significance and risk of exposure. 1,4 –9 The only consensus is that occupational radiation exposure should be kept as low as reasonable achievable (ALARA) as described in legislation. 10,11 Assessment of surgeon dose in many studies is flawed by the inconsistent use of personal dosimeters and personal protective equipment (PPE). 12 This highlights a need for prospective controlled research on dose to urologists.
It is the responsibility of the employer to take all steps that are necessary to restrict employees' exposure to ionizing radiation and to ensure that doses are monitored. “Medical and Dental Guidance Notes 2002” describes how to integrate the legislation into working practice, with shielding and dose monitoring required when employees are potentially exposed to greater than 3 μSv/hour. 13,14 The aim of monitoring should be to demonstrate that local rules on the use of X-ray equipment and PPE are effective, demonstrating that employees' dose is ALARA. This is the guideline for this audit study.
To our knowledge, these dose-reduction strategies have not been tested together in a controlled setting. The aim of this study is to perform an environmental audit to quantify the radiation dose that urologists receive during surgery in the lithotomy position, and the dose reduction that is achieved by altering exposure techniques and PPE use.
Subjects, Patients, Materials, and Methods
Equipment setup
An anthropomorphic phantom was positioned and fixed on a Maquet® Alphastar Pro operating table with stirrups in a supine position, with the symphysis pubis at the lower margin of the table. The phantom was a lumbar spine, pelvis, and hips of a human skeleton cast in Temex rubber material, and it was of female morphology with a 34 inch waist (model SK250; Pacific Northwest X-Ray, Inc.). A Raysafe® X2 R/F detector was positioned under the phantom to measure the absorbed dose in air as a guide to skin entrance dose in micro Grey per hour. The dose meter position was checked fluoroscopically to ensure that it remained in the primary beam of the imaged locations described next.
A Ziehm Vision® FD flat panel detector image intensifier was positioned over the patient as per Figure 1. The X-ray tube was under the table, as scatter dose from the tube side of the C-arm is significantly greater than the image intensifier side. 13 –15 The table height was set at a low working height that was comfortable for the 1.8 m tall study lead for ureteroscopy or cystoscopy. The X-ray tube focus to skin distance (FSD) was measured with a measuring tape, and the image intensifier height was fixed as low as the table base would allow throughout the study.

A Laerdal SimMan® Essential mannikin was dressed in a 0.25 mm Pb equivalent knee-length double-sided Rothband® (Fig. 1) apron and a 0.5 mm Pb equivalent thyroid shield. Double-sided aprons are used routinely, although the academic potential for increased backscatter body dose from the second layer of lead is an unquantified possibility. To simulate a standing surgeon, it was hung from a drip stand; for a seated surgeon, it was placed on the operating chair. The position of the simulated surgeon was marked on the floor to ensure reproducibility. A Thermo Scientific Radeye® B20 survey dose meter was used to measure the simulated surgeon dose in micro sieverts per hour. The positions on the mannikin for dose measurements were marked with tape to ensure reproducibility. Measurements were taken at the glabella, thyroid cartilage, umbilicus (in and out of the lead apron), symphysis pubis (in and out of the lead apron), and leg (at left medial malleolus).
Fluoroscopy was used to locate the areas of radiological interest defined by the study lead (bladder and kidney); a laser cross-guide projected by the image intensifier was used to mark the centering points on the phantom to ensure reproducibility (Fig. 1).
Standardization
Meter calibration was undertaken by an accredited calibration provider (RRPPS—Regional Radiation Protection Service, Birmingham). The initial measurements while imaging the pelvis were performed three times, and each time the same dose rate was measured. Therefore, all subsequent measurements were only performed once. The image intensifier automatic exposure device was used throughout the study. The study's emphasis was on dose to surgeons during clinical practice; hence, the effect of automatic exposure on surgeon dose was more important than standardization of beam energy. Background radiation was measured at 0.05 μSv/hour in all locations and was, therefore, discounted due to its constancy.
Dose-reduction strategies
Table 1 demonstrates the equipment setup for each arm of the study. Pulsed fluoroscopy rates were tested at 8 and 25 frames per second (maximum and minimum on the image intensifier). FSD was increased by elevating the table to a suitable high working height as defined by the study lead. Collimation was tested by reducing the irradiated field by 35% (measured by image area reduction on monitors; Fig. 1) with the intrinsic lead leaves. Lead table end protection was provided by a double-thickness 0.25 mm Pb equivalent apron hung on a luggage strap on the foot end of the operating table between the X-ray tube and the surgeon (Fig. 1). All dose-reduction measures were then tested together.
FSD = focus-to-skin distance.
The initial comparison of scatter dose to a surgeon sitting versus standing found sitting dose was higher for all locations (Fig. 2). Therefore, only dose-reduction techniques for standing were assessed further, as the aim of the study was to find the lowest dose to the surgeon.

Graph to show scatter radiation dose received by surgeon in both sitting and standing positions.
Results
Throughout the study, the kVp (kilo voltage peak) remained constant at 91 for imaging the kidney and 88 over the bladder. Trends in thyroid dose mirrored those of the eye and, hence, are not reported separately.
Figure 2 demonstrates the scatter dose to the surgeon when imaging the bladder when sitting and standing. Doses to the phantom were similar in both setups at 626 and 628 μGy/second, respectively, demonstrating that the quantity of photons that may become scattered to the surgeon were nearly identical for both exposures.
Figures 3 and 4 demonstrate the surgeon's dose compared with control rates with each alteration in technique when imaging the bladder and kidney, respectively. Figure 5 demonstrates how the alteration in techniques affects the skin dose.
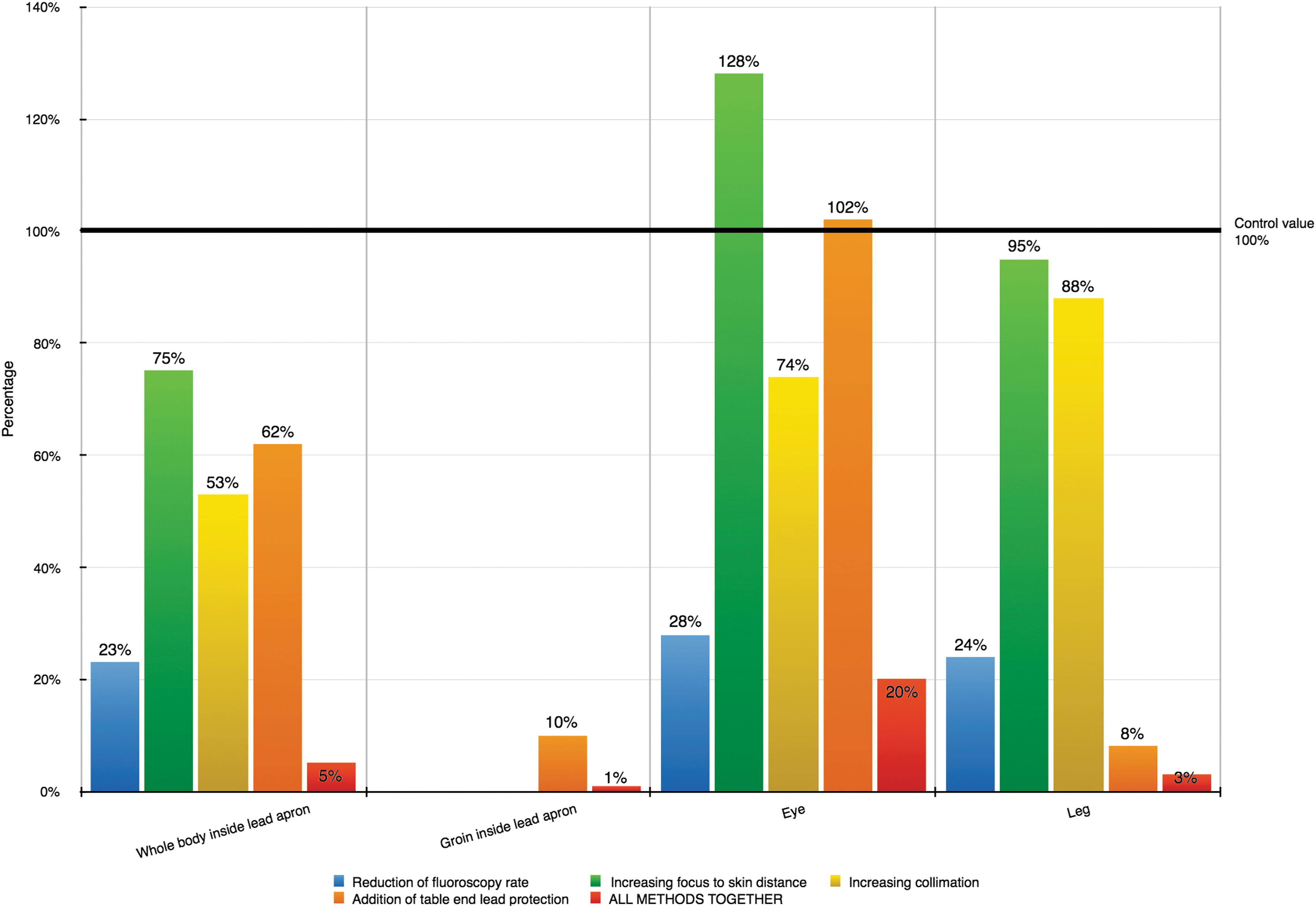
Graph to show surgeon dose rates with alteration of imaging technique for fluoroscopy over the bladder.

Graph to show surgeon dose rates with alteration of imaging technique for fluoroscopy over the kidney.
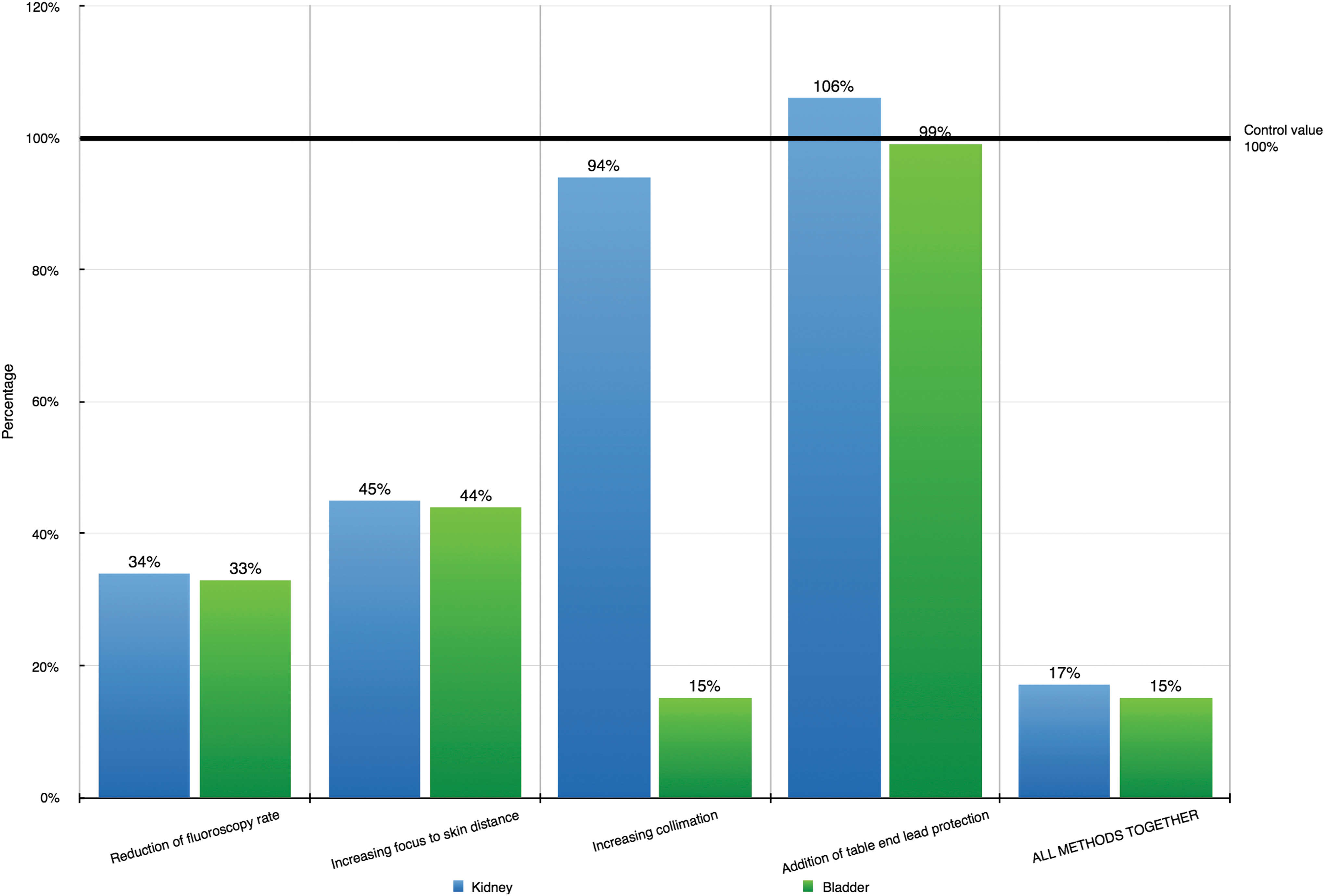
Graph to show the alteration in absorbed dose in air at the phantom skin with imaging technique alteration.
Discussion
An assessment of the surgeon's radiation doses demonstrates that sitting to perform fluoroscopically guided surgery results in higher occupational doses. The median dose increase was 17%, with the largest dose increase to the external genitalia. Sitting increased this dose by 78% from standing, despite the external apron dose changing by only 4%.
The doubling of distance from a radiation source reduces dose fourfold, as described by the inverse square law. 10,15 Compared with standing, surgeons are closer to the patient when sitting; therefore, surgeons receive higher doses of X-ray scatter from the patient.
Genitalia were not significantly closer to the radiation source when seated; therefore, higher observed doses when seated were unexpected. An explanation for this is that lead aprons may be elevated by a sitting surgeon's knees, forming an air gap and thus providing less protection. Without further assessment on dose-reduction techniques while sitting, it is advised that surgeons should stand to perform fluoroscopically guided procedures in the lithotomy position.
All international radiation protection organizations state that pulsed fluoroscopy must be used where possible. 14,16 –18 The use of pulsed fluoroscopy in this study reduced surgeon dose by 67% to 77% across all measured sites, similar to other published results. Cadaveric dosimetry studies of pulsed fluoroscopy demonstrated a decreased patient skin dose of 64% and a reduction in patient dose from 130 to 45 μSv/second, although they do not describe the pulse rates of the differing apparatus. 8,19 Both studies demonstrated adequate diagnostic image quality when using slower exposure rates. This study has made no assessment of image quality. Other reductions can be achieved by reporting fluoroscopy times to surgeons after ureteroscopy, resulting in a 24% reduction in subsequent cases, and tactile feedback instead of imaging for guidewire placement, reducing time by 82% or 100% in fluoroscopy-free procedures. 14,17,20
This study demonstrates that increasing the patient focus-to-skin distance (FSD), that is, the patient is further from the X-ray tube, decreases doses to the surgeon's body and leg by 5% to 25%. This was expected, as increasing the FSD reduces patient dose, as proved in this study. This is most likely explained by the surgeon's body being further from the source of the scattered photons, though the physics of scattered photons at 150° from the site of interaction could, in theory, be increasing the leg and genitalia dose when the table is higher.
The increased FSD resulted in increased doses to the eye and thyroid by 20% to 28%, due to their closer proximity to the phantom and scattered photons. Increasing the FSD, hence reducing the patient-to-detector distance, should improve image quality, reduce patient dose, and, as proved, reduce surgeons' trunk dose. Patients' skin dose should be acceptable if the X-ray source to skin distance is at least 30 cm but preferably 45 cm. 13,16,17 Decreasing the air gap between the patient and the image intensifier results in less attenuation of useful radiation (image-forming radiation), as it exits the patient. Dose to all should, therefore, reduce, as less X-rays need to transmit through the patient to result in the same quantity of photons at the receptor.
In this study, the use of collimation reduces dose to the surgeon by 12% to 47%. Collimation of the primary beam is advised by this and other studies to reduce radiation dose. 13,16,21 Collimation is seldom used, despite being regarded as good practice in guidelines. 13,21 Its use depends on a surgeon clearly identifying the area of interest and communicating this to the operator. Experienced operators will develop knowledge of procedures and be able to provide dynamic collimation spontaneously. Therefore, it is suggested that endourology fluoroscopy operators should be senior staff as in other areas of radiology practice where a high dose is likely.
Using lead protection at the table end was found to reduce surgeon leg and external genitalia dose by 90% to 94%, and 34% to 38% to the trunk. Interestingly, the additional lead protection increases the surgeon's eye dose by 2% to 6%. When the differences in skin dose are accounted for, it appears that there is no difference in eye dose. Table mounted lead shielding is seldom used in urology to reduce dose to the lower body and legs. 10,14 A prospective interventional radiology study over 8 weeks found that similar protection reduced operator dose by 64%. 22 Similar studies in urology during percutaneous nephrolithotomy resulted in a surgeon dose reduction of 96% to 98%. 23,24 As in other areas of radiology, the use of additional table end lead protection should become routine.
This study demonstrates a summative decrease in surgeon dose when pulsed fluoroscopy, increased FSD, beam collimation, and table end lead protection are used together. Trunk dose is decreased by 95%, external genitalia dose by 99%, and leg dose by 97%. The dose reduction of the eye and the thyroid is not as profound at 77% to 80% for imaging over the bladder and at 82% to 85% over the kidney. As these profound dose reductions fit clearly with the ALARA concept, the demonstrated techniques should become routine during all endourology cases.
All the technique alterations reduce the patient dose except for the additional lead table protection. This dose increase observed was small and may have been related to inconsistent exposure and is unlikely to be of significance. When fluoroscopy of the bladder was performed with collimation, there was an irregular reduction in dose. The collimation was probably shielding the detector from the primary beam, meaning that this and the dose registered with all protection methods in place are anomalous. Allowing for this, all dose-reduction methods result in a cumulative patient dose reduction of 83% to 85% and, therefore, should be used routinely as per the ALARA principle. Any small increase in patient one-off dose with the lead table protection is compensated for by other dose-reduction techniques and the profound summative reduction in surgeon dose.
There is a legal obligation for employers to provide PPE and for employees to use it when indicated by risk assessment.
25
Lead aprons should be at least a 0.25 mm Pb equivalent for photon energies below 100 kV and a 0.35 mm Pb equivalent when energy is greater than 100 kV.
13,14
Lead aprons should attenuate 90% or more of scattered X-rays, dependent on photon energy and lead equivalence.
10,15
Thyroid shields can reduce effective whole body dose more than thicker lead aprons.
13,15
A 0.35 mm Pb equivalent apron is reported to reduce effective body dose by 93% and addition of a thyroid shield increases this to 96%, though other data find that aprons may underperform by 20%.
26,27
Assessment of lead apron attenuation was made by comparing the dose rate per second inside and outside of the lead apron. This study found that the attenuation at trunk level when standing was 61% and 80%, and when sitting it was 54% and 58% for bladder and kidney, respectively. Formulae developed from Monte Carlo dose simulations calculate the estimated whole body effective radiation dose from the trunk and thyroid-level dosemeters.
2,26
T = 0.02 with a thyroid shield and 0.06 without. This results in the whole body effective dose rates demonstrated in Table 2. When the dose rate from outside the lead apron was used to calculate the unprotected surgeon dose and then compared with the dose rates from Table 2, the whole body effective dose reduction is calculated. This was 80% to 81% for the 0.25 mm lead equivalent apron used in this study, and it is at the lower end of the published values of 80% to 93%. 26,27 Increased photon transmission may be due to apron damage. Future lead apron audit may need to include measurement of attenuation and not just visual and fluoroscopic assessment. A further controlled assessment of whole body effective dose reduction with garments of varying lead equivalence is required along with ergonomic assessment.
Cumulative dose to urologists is of concern due to deterministic and stochastic effects. Stochastic effects of radiation are random, are usually regarded as having no threshold dose, and include induction of cancer and hereditary genetic mutations. The literature debates the quantity of X-ray photons that is significant for cancer induction based on data from atomic bomb survivors, nuclear disaster victims, and long-term follow-up of radiation workers. 9,16 It is unclear whether these data can be extrapolated down to lower doses as a linear no-threshold model; however, studies on mice and humans found similar rates of fatal cancer with 1 Sv exposure as those with no exposure. 1,9 The BEIR study looked at the long-term effects of radiation, and it concluded that tumor development is a response to error-prone DNA damage responses and mutagenesis. 1 Logically, there will never be a threshold for this failure (with the exception of thymus, ovarian, and leukemia neoplasia), and as data from nuclear disasters have a very wide confidence interval, the concept of a threshold dose requires cautious interpretation. 1 British medical radiation workers registered before 1954 had a 41% excess rate of cancer mortality, but after 1954, there was no elevated risk. 28 That may be due to improved technology, radiation protection techniques, or not enough lag time for tumourgenesis. 28 Published rates of fatal cancer induction are currently 5% per Sievert−1 with an average background radiation dose in the United Kingdom of 2.7 mSv/year, and when compared with a recent publication on urologists' annual dose measured over 12 days in a clinical setting, the annual occupational dose of 0.3 mSv is low. 1,8,29,30 Current thinking suggests that there is risk of stochastic effects with any radiation exposure, and, hence, occupational radiation exposure should be kept ALARA.
A single surgeon in a recent publication performed 60 ureteroscopies a year with a median fluoroscopy time of 36 seconds. 21 Obesity can increase intra-operative radiation dose to three times that of non-obese patients. 3 These data were used to calculate the urologist's approximate whole body effective dose per year based on this study's control dose rates, finding 0.05 mSv/year for kidney fluoroscopy and 0.15 mSv/year for bladder fluoroscopy. For bladder fluoroscopy alone, it would, therefore, take greater than 6000 years of working to reach the 5% risk of extra fatal cancer gained from receiving 1 Sv of radiation. With obese patients, significantly longer fluoroscopy times per case and a larger caseload than this 5% risk may be reached in a career. If all of this study's radiation protection factors are utilized, then the annual whole body effective dose drops by 95%. Therefore, even with larger patients, increased caseload, and increased fluoroscopy time, it would be unlikely that a urologist reaches the 5% additional risk in their career. However, the risk remains random and, hence, protection must be used as per the ALARA principle.
Deterministic dose to the lens of the eye is a subject of controversy in the published literature. The previously published dosimetry studies on urologists found that eye dose was likely to be 0.3 to 11 mSv annually for an average caseload endourologist, fitting with this study's control data. 8 Using this study's maximum dose-reduction techniques, annual eye dose would be 0.05 mSv. A deterministic effect requires a threshold dose before the change is apparent, for example, cataracts and skin burns. The International Committee on Radiation Protection recently reduced the cataract threshold dose to 20 mSv. 5,31 Using the same caseload data as for stochastic effects and using this study's control arm equipment setup on obese patients, the 20 mSv threshold could be reached within 23 years. Eye protection in the form of leaded glasses or ceiling mounted screens would be recommended to reduce eye dose by as much as 95%. 14,32 By using all the radiation protection techniques demonstrated in this study, the threshold for cataract formation will never be met in a urologist's career and wearing leaded glasses may not be absolutely required.
UK legislation on fluoroscopy radiation exposure includes the Ionising Radiation Regulations 1999 (IRR99) and Ionising Radiation (Medical Exposures) Regulations 2000 (IR(ME)R). 11,25 The former concentrates on the use of equipment, quality assurance, and occupational protection, whereas the latter allocates the responsibilities for patient exposures. Both state that radiation exposure to patients and staff must be kept ALARA. If the doses extrapolated earlier were replicated in real-life surgery, the dose to the surgeon would be within legal annual radiation dose limits. 21,25 The legislation requires “Practitioners” and “Operators” of fluoroscopy equipment to be trained in radiation protection. In an American study of surgeons with weekly occupational radiation exposure, lead aprons were worn on 99% of occasions, thyroid shields were worn 73% of the time, and 70% never wore a dose meter. 12 Although this study has not assessed training, there appears to be lack of knowledge on radiation doses and methods of protection by doctors. 21,33 This study should inform the endourology team on the risks of radiation exposure within their careers and methods of reducing their, their patients' and colleagues' doses. Provision of lead shielding on the table end may incur a one-off cost, but this should be seen as a legal obligation according to the legislations ALARA principles. 25 Other technique changes demonstrated in this study should only incur the cost of time to train radiology staff and surgeons. This collaborative multidisciplinary working can improve patient and staff care. This study provides clear evidence to recommend urologists' focus on keeping fluoroscopy time low and utilizing all of the dose-reducing methods described in the study.
Further studies could add to these data by assessing hand dose with this study's technique adjustments and assessing the dose reduction to surgeons who choose to sit throughout the procedure. Improvement of the measurement technique by using solid-state detectors may improve the accuracy of the data, but data collection would take a lot longer due to the need for longer exposures to achieve accuracy thresholds for the detector. Assessment of dose reduction to female surgeon gonadal tissue is needed but was not possible with the manikins available in this study.
The patient and staff dose-reduction techniques described are simply depicted by the International Atomic Energy Agency and are a useful resource for staff in theater. 34,35
Conclusions
This study demonstrates how the tested alterations in technique reduce patient and, more importantly, cumulative urologist dose. The change with the greatest reduction in dose is slower frame rate. The use of these techniques prove that dose to surgeons can and should be reduced as per the guidelines. By following these strategies, the risk of deterministic effects is very unlikely and stochastic risk is kept ALARA throughout a urologist's career. The potential effects of not implementing these dose-reduction methods are visual loss and fatal neoplasia. Changes that this study suggest have very little cost impact, and they are mostly achievable by alteration of practice and communication with colleagues.
Footnotes
Acknowledgments
The author acknowledges Mr. R. Calvert and Ms. M. Lyttle.
Author Disclosure Statement
No competing financial interest exists.