
Abstract
Objective:
To compare the outcomes between laparoendoscopic single-site (LESS) and a novel percutaneous externally assembled laparoscopic (PEAL) nephrectomy in an in vivo porcine model.
Materials and Methods:
Ten female farm pigs were randomized to LESS nephrectomy (5) or PEAL nephrectomy (5). Operative times, estimated blood loss, and intraoperative and postoperative complications were compared. The surgeons used a Likert scale to grade difficulty of peritoneal access, port placement, tool assembly, hilar dissection, closure, and overall difficulty of surgery. Scar assessment was performed by a blinded plastic surgeon using the Vancouver Scar Scale. Descriptive statistics were reported as median and range. The Mann–Whitney U test was used for continuous and ordinal variables. A p value <0.05 was considered significant.
Results:
Median operative time was significantly shorter in the PEAL group vs the LESS group (85 minutes vs 127 minutes, p = 0.03). Median Likert scores showed overall hilar dissection and nephrectomy to be significantly easier using PEAL compared with LESS (2 vs 9, p < 0.01 for both). The PEAL instruments left no visible scar at 5 feet in any animal, and only 1 out of 10 scars could be identified on physical examination.
Conclusions:
The PEAL surgical paradigm demonstrates nearly scarless outcomes while providing shorter operative times and easier performance than LESS nephrectomy in a porcine model.
Introduction
S
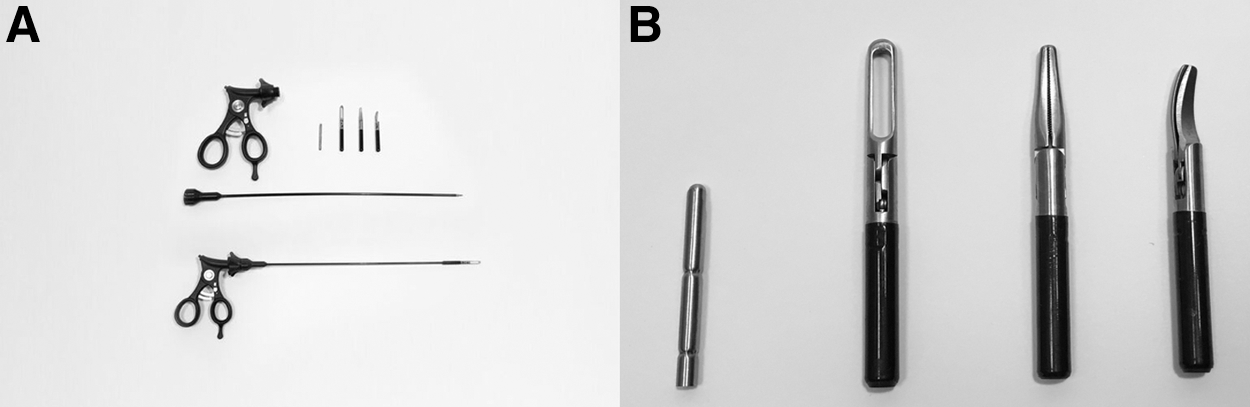
In an attempt to create an instrument with a more functional 5 mm tip while maintaining the nearly scarless cosmesis of a 2.96 mm instrument shaft, our group designed and created percutaneous externally assembled laparoscopic (PEAL) instruments. The prototype instruments employed in this study were manufactured by Teleflex Surgical (Percuvance™ Percutaneous Surgical System; Teleflex Surgical, Wayne, PA) (Fig. 1). These 5 mm tips are functionally similar to conventional laparoscopic instrumentation, but the smaller shafts maintain a nearly scarless cosmetic outcome similar to conventional LESS. 8 In addition, because of their small-caliber shafts, these instruments can be percutaneously inserted at sites away from the main incision to reestablish triangulation, an essential element of conventional laparoscopic surgery. A recently published case report and case series demonstrated the feasibility of PEAL gynecologic and gastrointestinal surgery. 9,10 To date, no previous studies have evaluated the use of these instruments in urologic surgery. This prospective, randomized, single-blinded study compares the outcomes of nephrectomy using PEAL instruments vs LESS in an in vivo porcine model. We hypothesize that using PEAL instruments can simplify LESS by restoring triangulation while maintaining the cosmetic advantages that LESS has over conventional laparoscopy.
Materials and Methods
This study was approved by our Institutional Animal Care and Use Committee. Ten female farm pigs were randomized to LESS (5) or PEAL (5) nephrectomy. All surgeries were performed under general anesthesia by using a combination of ketamine (2.2 mg/kg), telazol (4.4 mg/kg), and xylazine (2.2 mg/kg) for induction. The pigs were intubated, and general anesthesia was maintained by using isoflurane (2.5%–3.5%).
In both LESS and PEAL surgeries, a 4 cm umbilical incision was made through which a GelPoint (Applied Medical, Rancho Santa Margarita, CA) was placed. This single-site port provided for instrument tip exchange and ultimate specimen removal. Carbon dioxide gas was used to insufflate the peritoneal cavity to 15 mm Hg.
In the LESS group, three 12 mm ports were placed through the GelPoint and a 10 mm 30° laparoscope was used (Fig. 2). For the PEAL group, three 12 mm ports were also placed through the GelPoint as in the LESS group for standardization purposes. However, only two of these ports were used during the PEAL surgery, one for a 10 mm 30° laparoscope and a second port for a conventional hook electrode and clip applier. In addition, two 2.96 mm PEAL instrument shafts were percutaneously inserted through the abdomen 2 cm lateral to the nipple line by using the PEAL insertion retractable needle tip (Fig. 3a, b). The instrument shafts were then brought out of the umbilical incision after removing the Gelpoint multi-access port lid, and the insertion tip was removed (Fig. 3c). Next, the desired instrument tip was screwed into place and brought back into the abdomen (Figs. 3d, e, and 4). Both LESS and PEAL nephrectomy proceeded as described in our previously published study. 8,11 The PEAL instruments were employed to reestablish triangulation and to maintain lateral traction on the ureter and kidney, which greatly simplified the hilar dissection and performance of the nephrectomy. The same senior endourology fellow who was a skilled laparoscopic surgeon but had no experience with either LESS or PEAL performed all procedures to allow assessment of the learning curve. He was assisted by a fellowship-trained endourologist. Operative times, estimated blood loss (EBL), and intraoperative and postoperative complications were recorded. On completion of each procedure, a Likert scale (1 = easy; to 10 = very difficult) was completed by both members of the surgical team, grading difficulty of peritoneal access, port placement, tool assembly, hilar dissection, wound closure, and overall ease of nephrectomy. Operative time was calculated as the time from skin incision to the completion of wound closure. The pigs were observed for 4 weeks postoperatively, after which the scars were evaluated by a blinded board-certified plastic surgeon using the Vancouver Scar Scale. 12
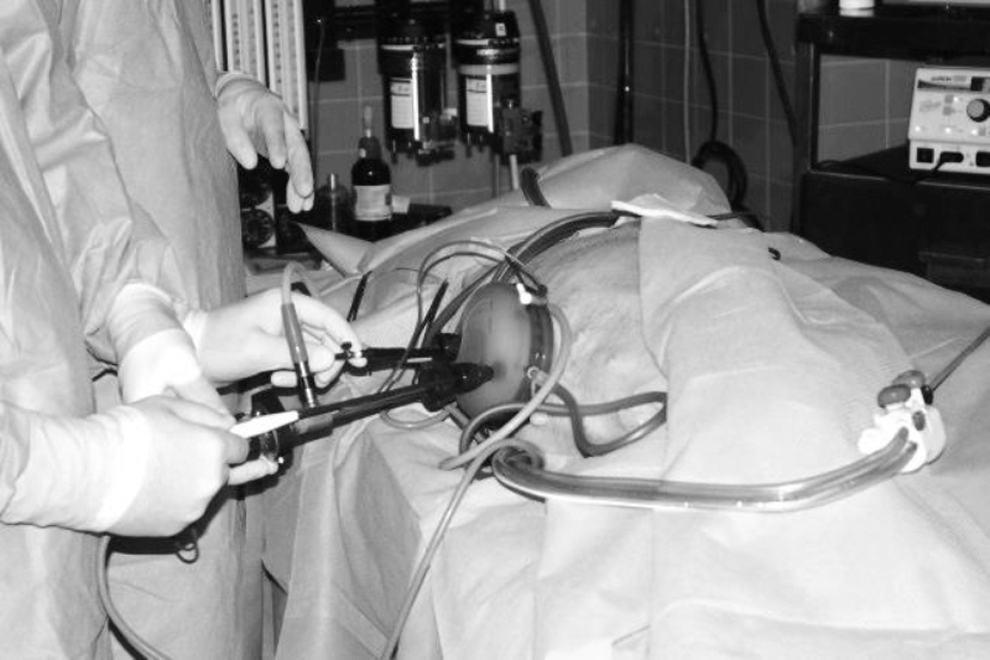
Port placement and technique employed for traditional LESS nephrectomy. Close instrument proximity during traditional LESS limits triangulation and predisposes to instrument collision. LESS = laparoendoscopic single-site.
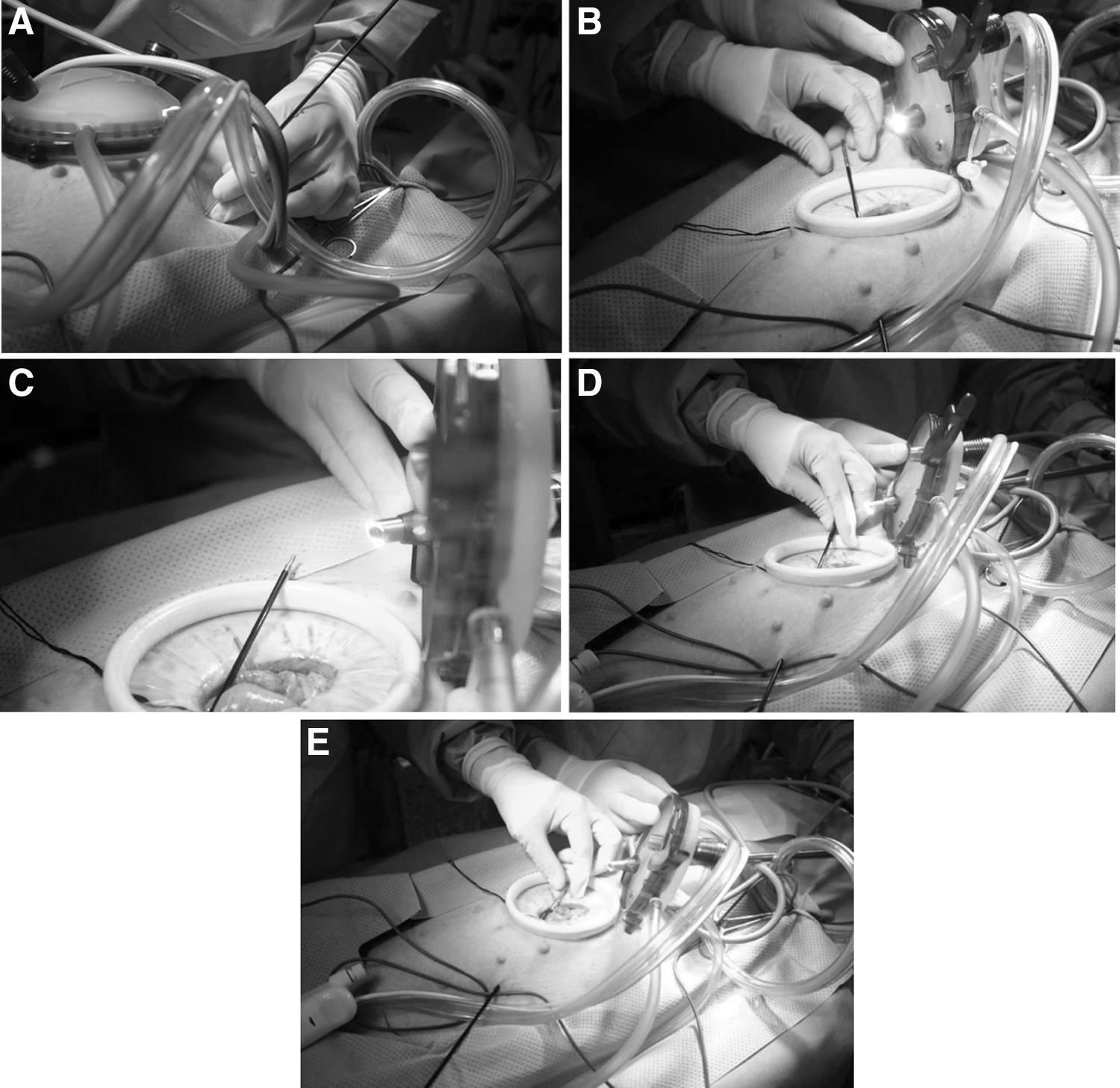
Assembly of PEAL instrument.
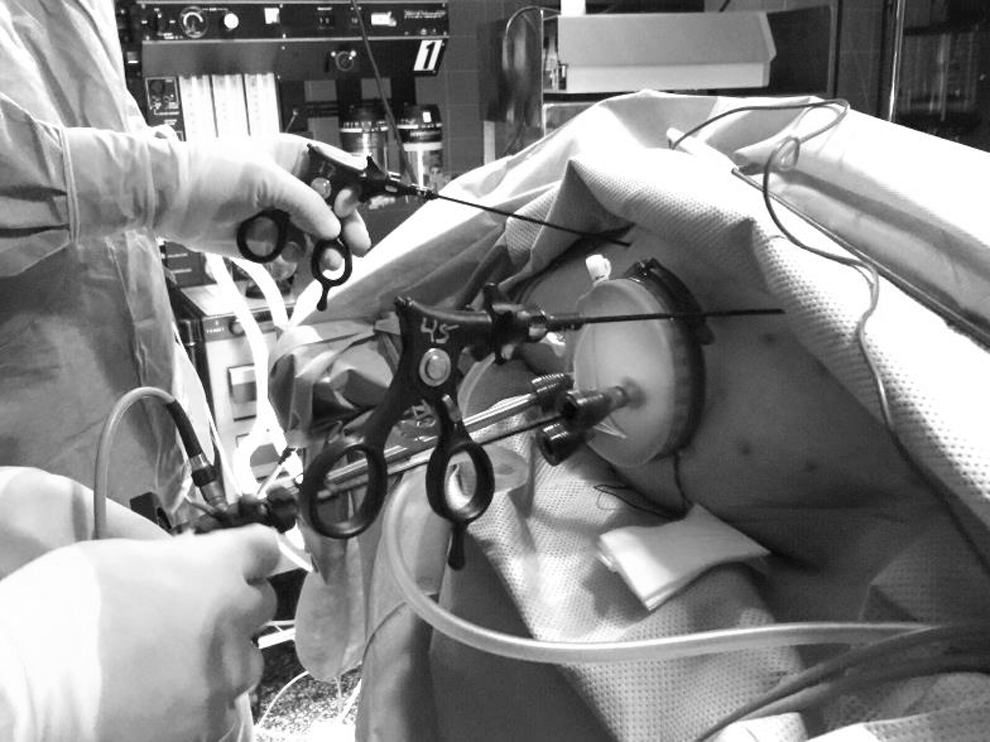
Port placement and technique employed for PEAL nephrectomy. Use of PEAL instruments restores instrument triangulation and minimizes instrument conflict, allowing significantly reduced operative time and difficulty.
Descriptive statistics were reported as a median and range. The Mann–Whitney U-test was used for continuous and ordinal variables by using SPSS version 21.0 (IBM, Armonk, NY) with p < 0.05 considered significant.
Results
Five pigs underwent conventional left LESS nephrectomy, and five pigs underwent left PEAL nephrectomy. There was no difference between the two groups in terms of EBL, pig weight, or hemoglobin change (Table 1). However, median operative time was significantly shorter in the PEAL group vs the LESS group (85 minutes vs 127 minutes, p = 0.03). The median Likert score for difficulty of hilar dissection for the PEAL group was significantly lower than for the LESS group (2 vs 9, p < 0.01). The median Likert score for overall difficulty of nephrectomy was also significantly lower in the PEAL group than in the LESS group (2 vs 9, p < 0.01). The remainder of the categories graded showed no statistically significant difference (Table 2). The median Likert score for difficulty of tool assembly was 3 for the PEAL instruments and there was no score for the LESS instruments, as they did not require any assembly. There were no intraoperative complications but there were two hernias at the umbilical incision site, one in each group. Percentage decrease in operative time between the first and last surgeries was greater in the PEAL group compared with the LESS group (26.1% vs 21.7%, respectively).
Bold values indicate p value <0.05.
EBL = estimated blood loss; LESS = laparoendoscopic single-site; PEAL = percutaneous externally assembled laparoscopic.
Bold values indicate p value <0.05.
There was no difference in median Vancouver scar score for the midline umbilical scar (2.2 for the LESS group vs 2.0 for the PEAL group, p = 0.85). At a distance of 5 feet, the blinded plastic surgeon could identify the umbilical incision in four out of five pigs in both groups. He was able to identify 0 out of 10 scars caused by the PEAL instruments from a distance of 5 feet. There were no scars other than the umbilical scars in the LESS group. After the type of surgery was disclosed, the plastic surgeon was able to identify the midline umbilical incision in all five pigs but still could not identify the PEAL instrument scars at a distance of 5 feet. From bedside, the plastic surgeon was able to identify the midline umbilical incision in all 10 pigs but could identify only 1 out of 10 PEAL instrument insertion sites.
Discussion
LESS and needlescopic surgery were developed to further reduce the invasiveness of conventional laparoscopy by decreasing its morbidity and cosmetic impact. Urologists first applied LESS to renal surgery, 13 and demonstrated success via both transperitoneal and retroperitoneal approaches. 14 LESS has subsequently seen modest worldwide growth and is now performed in a wide variety of urologic surgeries. 15,16
While providing exceptional cosmesis, LESS has been hindered by the fact that it is technically challenging to perform and is associated with a steep learning curve. The use of a single site results in a loss of instrument triangulation and predisposes to instrument collision. 6 A study by Montero and colleagues included 14 residents and fellows and reported that LESS was associated with decreased surgical performance and increased surgeon workload by 35%–53% compared with standard laparoscopy. 17 Another study by Islam and colleagues included 45 participants of differing surgical experience who performed peg transfer comparing conventional laparoscopy with LESS. The study reported a 40%–65% decline in peg transfer performance for LESS compared with conventional laparoscopy. 18 All these studies quantified what was immediately clear to surgeons performing LESS procedures: that these surgeries were technically more difficult to perform than conventional laparoscopy. Although technically challenging, LESS improves cosmesis and reduces invasiveness compared with conventional laparoscopic nephrectomy. 19,20
To compensate for these technical challenges, surgeons became more stringent in selecting patients to undergo LESS. In a multicenter study on global trends in minimally invasive adrenalectomy that included more than 700 patients, LESS was reported to be the most widely used in Asia, where it represented 60% of cases. In contrast, it accounted for less than 20% of cases in the United States and only 10% of cases in Europe. 21 A method to restore triangulation that would not significantly increase the invasiveness of the procedure or alter the nearly scarless cosmetic result could allow more patients to benefit from LESS surgery.
One method employed to re-establish triangulation, while reducing the invasiveness of traditional laparoscopic surgery, was the use of needlescopic instrumentation with tools ≤3 mm in size. Needlescopic surgery maintains triangulation and avoids instrument collision. However, it is associated with its own technical challenges. In a series of 101 patients who underwent needlescopic surgeries including Nissen fundoplication, splenectomy, Heller myotomy, and bilateral thoracic sympathectomy, Mamazza and colleagues reported that despite excellent cosmesis and short hospital stay, the decreased robustness of needlescopic instruments resulted in less compression force for hemostasis and heavy organ manipulation. 7 A similar finding was also reported in a series of needlescopic adrenalectomies, where Gill and colleagues reported frequent slippage of the grasped tissues due to instrument weakness. Needlescopic instruments also may be more prone to cause puncture injury to intra-abdominal viscera, and the authors recommended extreme caution during tissue handling. 22 Conventional needlescopic instruments placed with a 3.3 mm port leave a 5 mm scar, whereas instruments placed without a port may be more prone to dislodgment. In contrast, PEAL instruments do not fall out, are placed without a port, and are placed through a puncture that can be identified only 10% of the time.
The 5 mm PEAL instrument tips have demonstrated surgical performance similar to conventional laparoscopic tools in a benchtop study. 8 In the current study, PEAL surgery resulted in a restoration of triangulation with robust 5 mm instruments that reduced the operative time by one-third and greatly simplified hilar dissection and the performance of the nephrectomy. With traditional LESS nephrectomy placing the lateral and anterior retraction on the ureter to facilitate the hilar dissection was challenging. In contrast, the PEAL instruments greatly facilitated this step, dramatically simplifying the hilar dissection and, subsequently, the overall nephrectomy. In addition, PEAL instruments are less likely to result in injury to intra-abdominal organs 11 and may shorten the learning curve as demonstrated in our current study.
Other potential benefits of the PEAL surgical paradigm may include a nearly scarless cosmetic outcome, reduced postoperative pain, reduced cost, and improved patient safety, although these factors will need to be studied in human trials. Although needlescopic surgery has been reported to have excellent cosmetic outcomes, 22,23 it does require placement of a port, which necessitates a larger skin incision. For example, the outer diameter of a 3 mm port is 5.16 mm. In contrast, PEAL instruments are employed without a port and, thus, they allow the largest, stiffest instrument shaft possible to be placed through the 3 mm puncture. A 4 cm umbilical incision was selected in this study to allow intact extraction of the kidney, thereby reducing the costs of the study by avoiding a laparoscopic retrieval bag. However, these instruments can be easily employed in combination with any port that is 5 mm or larger.
In a prospective study of 60 patients undergoing cholecystectomy, 2–3 mm needlescopic instruments produced 37% less postoperative pain than those whose surgery was performed with conventional 5 mm laparoscopic instruments, confirming that smaller incisions produce less pain. 24 Although postoperative pain could not be quantified in the present porcine study, we expect that the use of smaller-caliber instrument shafts will decrease postoperative pain. Lastly, we expect shortened operative time and decreased technical difficulty of surgery to translate into reduced cost and improved patient safety. 25,26
Early published cases using PEAL instruments have confirmed some of these hypothesized benefits. Rossitto and colleagues published a case report of a successful hysterectomy performed by using PEAL instruments in combination with a traditional 5 mm port. 9 Chang and colleagues reported the efficacy of PEAL instruments in combination with 5 and 10 mm ports in a retrospective series of 15 gastrointestinal surgeries. 10 The technique was feasible, and the introduction of the PEAL instrument and application of the instrument tips was not technically difficult. There was no loss of pneumoperitoneum on removing the PEAL instruments, and no intraoperative complications attributed to the use of the instruments were encountered.
In addition to its use as a stand-alone surgical modality, PEAL instruments may also be used to supplement traditional laparoscopic surgery. PEAL instruments have the ability to perform simple tasks such as organ retraction as well as relatively complex tasks such as intracorporeal suturing. 9,10 PEAL instruments may be used to simplify a complex procedure while providing minimal scar formation and expand the application of LESS to even large and obese patients.
This study is not free of limitations. Although we were able to perform a prospective single-blinded study, it was limited by a modest sample size. To evaluate the learning curve associated with PEAL surgery, we carried out this study with a surgeon who had no previous experience in LESS or needlescopic surgery. For this reason, we chose to perform our initial study in pigs rather than humans, which is itself a well-established training model for laparoscopic renal surgery. 27 The anatomy of a pig differs compared with that of a human. In particular, pigs often have a single renal artery that divides into caudal and cranial segmental branches. 28 However, for the purposes of scar evaluation, pigs represent an excellent model that resembles human wound healing. 29 All nephrectomies were done on normal kidneys, and, therefore, we were unable to evaluate the performance of PEAL instruments in situations that alter the normal anatomy and increase the difficulty of surgery. Finally, experienced LESS surgeons were not included in the randomization process. It is possible that experienced LESS surgeons may perceive reduced benefit from the PEAL instrumentation. Future multicenter prospective studies including surgeons with a wide variety of surgical experience will be necessary to fully validate the efficacy of this novel instrument paradigm. Despite these limitations, this study is the first to compare the outcomes of conventional LESS and PEAL nephrectomy in a prospective, randomized fashion.
Conclusion
The addition of PEAL instruments to LESS is feasible and decreases the difficulty of nephrectomy in a porcine model while maintaining nearly identical cosmetic outcomes. Prospective studies carried out in humans are needed to demonstrate the benefits and expand the indications for PEAL surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.