
Abstract
Introduction & Objectives:
Transurethral enucleation of the prostate for the management of benign prostatic obstruction (BPO) involves two steps: the enucleation and morcellation procedure. The aim of our study was to assess the efficacy of a morcellator device using disposable and reusable blades with different settings of morcellation speed.
Methods:
A prospective randomized study was initiated for patients with symptomatic BPO undergoing Thulium laser enucleation of the prostate. Mechanical tissue morcellation was performed using the Piranha™ morcellator (R. Wolf, Knittlingen, Germany) with disposable or reusable blades at 850 (n = 24) or 1500 revolutions per minute (rpm) (n = 24). Patient characteristics, intraoperative complications, and the morcellation rate (g/min) were recorded. Data are expressed as median and interquartile range (IQR).
Results:
Forty-eight patients were randomized using disposable (n = 24) or reusable blades (n = 24). For reusable blades, the morcellation rate did not increase when changing the morcellation speed from 850 to 1500 rpm (5 vs 4.53 g/min, p = 0.843). The morcellation rate increased significantly when changing the morcellation speed from 850 to 1500 rpm using single-use blades (4.77 vs 10 g/min, p ≤ 0.014). The morcellation rate was not different at 850 rpm between reusable and single-use blades (5 vs 4.77 g/min, p = 0.671). Conversely, the morcellation rate was significantly different at 1500 rpm between reusable and single-use blades (4.53 vs 10 g/min, p ≤ 0.017). The total morcellation rate (at 850 and 1500 rpm) was significantly increased using single-use blades compared to reusable blades (7.67 vs 4.8 g/min, p ≤ 0.026). Interestingly, enucleated weight (g) and the morcellation rate (g/min) correlated inversely using single-use blades at 1500 rpm (r = −0.742, p ≤ 0.004). Only one superficial bladder injury occurred at 1500 rpm, which needed no further interventions.
Conclusions:
The Piranha morcellator facilitates efficient tissue removal with single-use and reusable blades. Disposable morcellator blades increase tissue removal significantly at 1500 rpm.
Introduction
L
Holmium laser enucleation of the prostate (HoLEP) is recommended by the current EAU guidelines as an alternative to transurethral resection of the prostate (TURP) in men with moderate-to-severe lower urinary tract symptoms (LUTS) and should particularly be advocated to patients with prostates >80 cc. 3 Based on the HoLEP technique, alternative transurethral enucleation techniques with different energy sources have been introduced 4 utilizing Thulium:YAG laser, 5 GreenLight laser, 6 Diode laser, 7 or plasma kinetic energy. 8 However, the efficacy and safety of transurethral enucleation of the prostate rely on another important step: the morcellation procedure. Although a tedious, but crucial step for the patient, the morcellation procedure has clinically not been well studied. 9 Only sparse data from ex vivo models are available regarding the optimal morcellation speed and the influence of the morcellator blade design on the efficacy of the morcellation procedure. 10
Aim of this prospective randomized study was therefore to compare two different blade designs for the Piranha™ morcellator at two different speed settings for the first time.
Materials and Methods
After institutional review board approval, 48 consecutive patients with symptomatic BPO were considered eligible for surgical treatment and enrolled in this unicentric prospective randomized study. All patients were treated with Thulium laser VapoEnucleation of the prostate (ThuVEP) combined with consecutive morcellation of the enucleated tissue. During all interventions, physiologic saline was used as irrigation fluid. The technique of ThuVEP has been previously reported in detail. 5 All procedures were carried out by two experienced surgeons (A.J.G., C.N.). A continuous-wave Tm:YAG laser (VelaXL®; Boston Scientific, Ratingen, Germany) was used as the energy source at 90 Watt. Laser energy was delivered through a 550 μm optical core bare-ended, reusable laser fiber. The procedure was performed using a 26F continuous-flow laser resectoscope combined with the mechanical Piranha tissue morcellator by R. Wolf.
The morcellator knife is equipped with a serrated blade that oscillates the prostate adenoma side to side (Fig. 1). Due to the blunt tip of the morcellator device, bladder injuries can be reduced. Furthermore, the morcellator consists of a motor handle, a generator, and a suction pump. The tube set is a disposable item of the system. Due to a footswitch that has a dual function, the surgeon is able to switch separately between a suction and morcellation mode or a pure suction mode. The morcellator pump has to create a vacuum to start oscillating and suck in the tissue (Fig. 2). The Piranha morcellator can be used with a disposable or a reusable morcellator blade. Due to the surgeon's experience of morcellation and the deteriorating sharpness of the reusable blades, they are generally discarded after five uses at our institution (a total of five reusable blades were used). The morcellator was used at two different speed settings: 850 or 1500 revolutions per minute (rpm). The initial recommended speed setting by the R. Wolf company was 850 rpm for tissue retrieval with the Piranha morcellator.
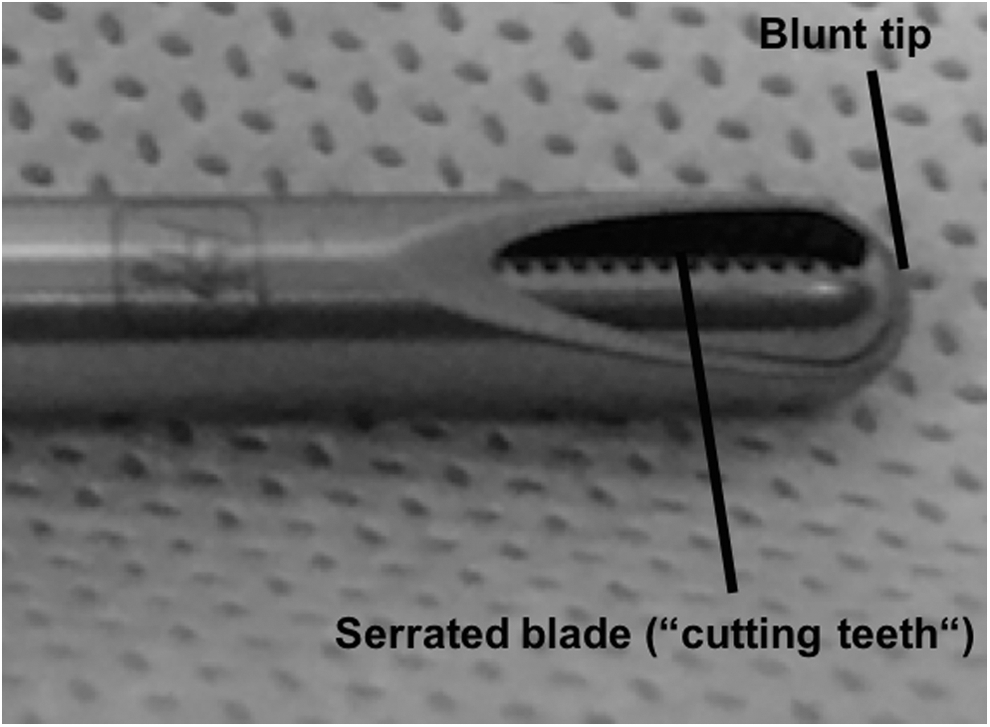
Serrated blade of the Piranha device by Richard Wolf equipped with a blunt tip.

Serrated blade of the Piranha morcellator in action.
In the study of Ritter and colleagues, a significant increase in the morcellation rate at 1500 rpm was pointed out and is also mentioned at the official website of R. Wolf for better tissue retrieval. Our study design was based on these new findings to verify the results for the clinical utility. 10 The morcellation time was measured manually, starting at the time of instrument insertion until complete morcellation and evacuation of the tissue. The suction pump container used to collect the solution and the morcellated tissue was emptied before starting the morcellation process to provide maximal suction. The morcellation time (min) and tissue dry weight (g) were recorded, and the morcellation rate (g/min) was calculated. Tissue dry weight was measured after time in formalin before histological examination. Complications during the morcellation process were recorded.
The primary outcome was the morcellation rate at 1500 rpm. Secondary outcomes were the morcellation rate at 850 rpm, the total morcellation rates of single-use and reusable blades, and the complications during morcellation. Ritter and colleagues published a 93.8% increase of the morcellation rate of the Piranha morcellator using the single-use blade compared to the reusable blade at 1500 rpm. 10 A mean morcellation rate of 2.6 g/min was assumed for the use of reusable blades at 1500 rpm. The institutional mean of 2.6 g/min is based on the findings from the article of Gross and colleagues from our institution. 1080 patients were treated with ThuVEP using the Wolf Piranha morcellator for consecutive tissue morcellation. This morcellation rate seems to be robust although the morcellation rates were calculated from 1080 procedures done by 11 surgeons. 11 This is in contrast to other single-surgeon studies (e.g., HoLEP series), which published the morcellation rates of expert surgeons.
The sample size calculation assumed a relevant difference in the morcellation rate of 2.402 (SD = 2) g per minute between single-use and reusable morcellator blades. With α = 0.05 and a power of 90% (β = 0.20), a sample size of 12 patients per group was therefore calculated for each speed setting (850 and 1500 rpm). SPSS for windows was used for statistical analysis. The Mann–Whitney U test was applied to determine differences between primary and secondary outcome parameters of the study arms. Categorical variables were compared using the chi-square-test. Data are presented as median (interquartile range). A p-value <0.05 was considered statistically significant.
Results
A total of 48 patients were enrolled in the study and randomized using disposable (n = 24) or reusable blades (n = 24) (Table 1). The total morcellation rate (at 850 and 1500 rpm) was significantly increased using single-use blades compared to reusable blades (7.67 vs 4.8 g/min, p ≤ 0.026) (Fig. 3 and Table 1).
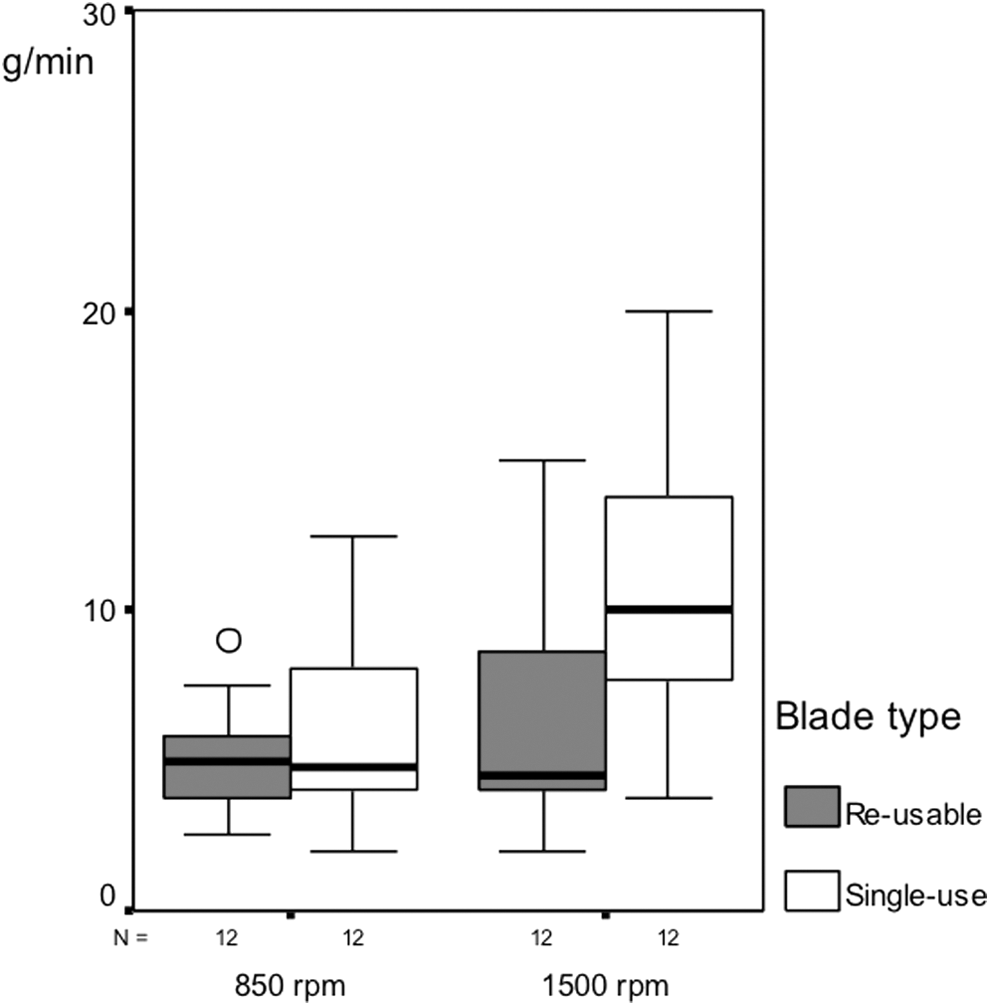
Boxplot. Comparison of morcellation rates [g/min] of reuseable and single-use morcellator blades at 850 and 1500 rpm. The morcellation rate differed significantly between single-use blades at 850 and 1500 rpm (p ≤ 0.014).
Data as median (Interquartile range).
For reusable blades, the morcellation rate did not increase changing the morcellation speed from 850 to 1500 rpm (5 vs 4.53 g/min, p = 0.843) (Table 2), while the morcellation rate significantly increased changing the morcellation speed from 850 to 1500 rpm using single-use blades (4.77 vs 10 g/min, p ≤ 0.014) (Table 3). The morcellation rate was not different at 850 rpm between reusable and single-use blades (5 vs 4.77 g/min, p = 0.671). Conversely, the morcellation rate was significantly different at 1500 rpm between reusable and single-use blades (4.53 vs 10 g/min, p ≤ 0.017) (Fig. 4). Interestingly, enucleated weight (g) and the morcellation rate (g/min) correlated inversely using disposable blades at 1500 rpm (r = −0.742, p ≤ 0.004) (Fig. 5).
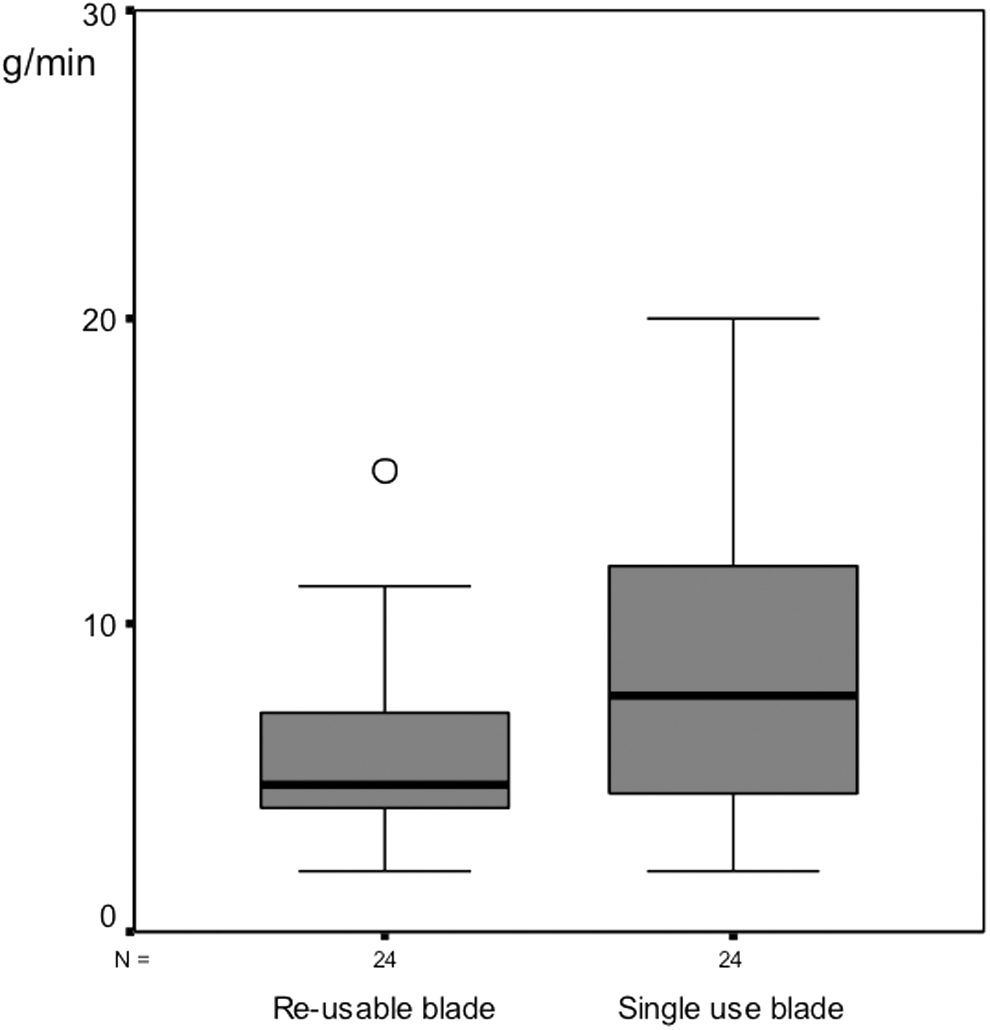
Boxplot. Comparison of morcellation rates [g/min] of reuseable and single-use morcellator blades. The morcellation rate differed significantly between single-use blades and reusable blades (p ≤ 0.026).
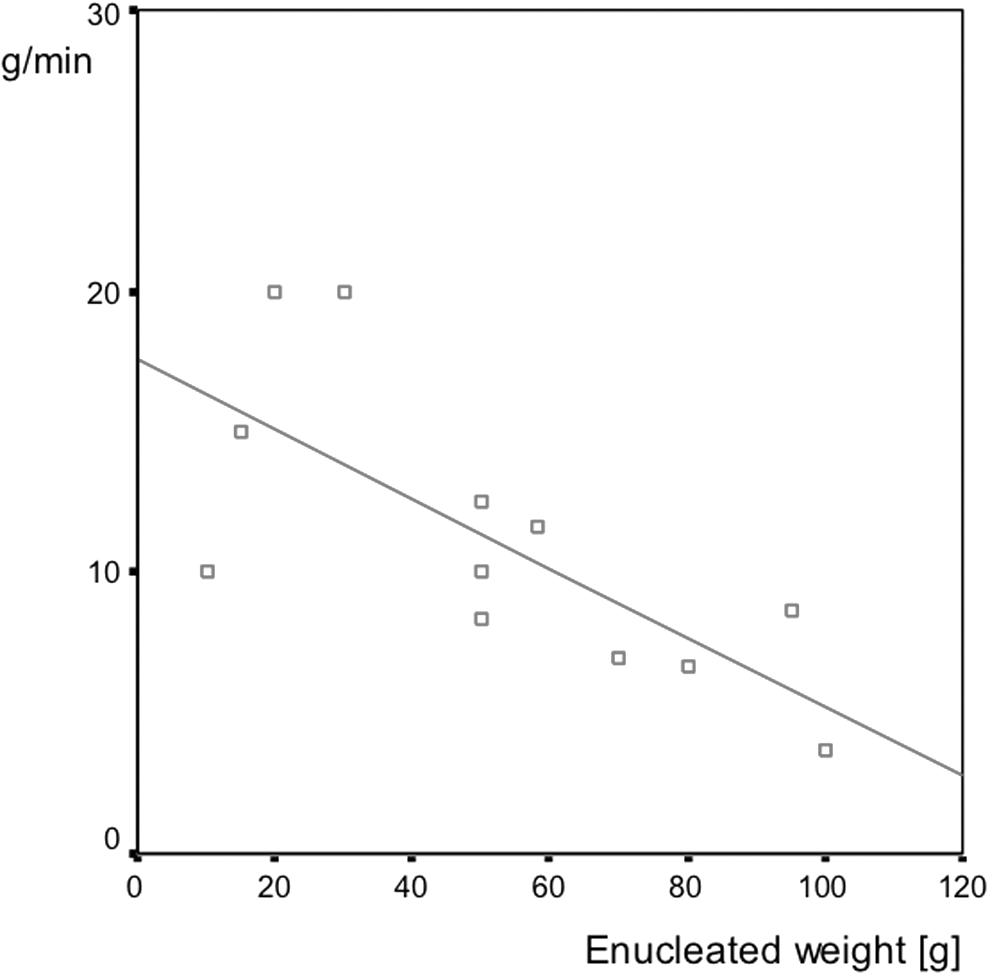
Scatterplot of enucleated weight [g] and the morcellation rate [g/min] using the single-use blades at 1500 rpm. Enucleated weight and the morcellation rate correlated inversely at 1500 rpm (r = −0.742, p ≤ 0.004).
Data as median (Interquartile range).
Data as median (Interquartile range).
The appearance of “beach balls” or the so-called “crazy-ball effect” during morcellation hindered the process of tissue retrieval due to the plain surface and the trouble to suck the small adenoma parts into the morcellator device. However, there was no beach ball that required retrieval with graspers or by second morcellation. Regarding the complications during morcellation, one bladder injury occurred at 1500 rpm using a disposable blade. Bladder mucosa was incidentally sucked in and created a superficial bleeding of the bladder. It was bipolar coagulated and did not entail any complications postoperatively with regular removal of the urinary catheter after 2 days.
Discussion
In this study, we evaluated two different kinds of blades of the Piranha morcellator system by Richard Wolf (disposable vs reusable blades) with two different basic adjustments of the oscillation rate (850 and 1500 rpm). We could prove that the tissue retrieval significantly increased with an increasing morcellation speed for disposable blades. However, this difference could not be shown for reusable blades.
In numerous prior studies, it has been shown that HoLEP is superior to TURP and open prostatectomy regarding perioperative complications. 1 –3,12 Since the first description of HoLEP by Fraundorfer and Gilling, a lot of technical improvements and different sources of energy were introduced to improve the process of transurethral enucleation of the prostate. 4,13 The enucleation procedure is followed by an intravesical mechanical morcellation of the enucleated adenoma in the initial description of the HoLEP procedure by Gilling and Fraundorfer. 13,14 Thereafter, the safety and efficacy of the enucleation step of the HoLEP procedure have been widely described and variables such as surgical devices, laser systems, and the learning curve have been explored. 1,2 However, the second step of the surgical procedure–the morcellation step–is yet poorly evaluated. 15
Only few studies have investigated the tissue retrieval rate after enucleation of the prostate in a clinical setting. This is the first study that elucidates the morcellation rate after ThuVEP. Currently, two morcellators (Piranha by R. Wolf, Knittlingen, Germany, and VersaCut by Lumenis, Yokneam, Israel) are widely used. The differences include the movement (oscillation vs guillotine) and the shape of the blades (serrated vs nonserrated) for either Piranha or the VersaCut morcellator. In experimental and clinical settings, the morcellation rates for both morcellators achieved comparable results. Another morcellator, the Drillcut-X® II N (Karl Storz, Tuttlingen, Germany), has not been investigated in clinical studies so far. Therefore, this morcellator is disregarded in this article.
In our study, at a speed setting of 850 rpm for both types of blades as well as 1500 rpm for reusable blades, there were no significant differences in the tissue retrieval rate. These data are comparable to the morcellation efficacy as reported in the literature. 12,16 However, using disposable types of blades at a speed setting of 1500 rpm, we could show a significantly higher morcellation rate of 10 g/min compared to 4.53 g/min at a speed setting of 850 rpm. We believe that the significant increase in morcellation rate at 1500 rpm with the disposable blade is based on the design of the cutting teeth with a closer range of each tooth as well as the wider opening of the knife. 1500 rpm seems to be most effective for sucking the adenoma into the blade without losing its grip and is recommended for regular tissue retrieval of prostate adenomas after transurethral enucleation. Another possible explanation might be that morcellation at 850 rpm leads to larger tissue chips. Due to the wider opening of the disposable blades, it might cause a more difficult extraction of these larger tissue chips during suction than producing smaller chips at 1500 rpm. Recently published data by El Tayeb and colleagues showed contrary tissue retrieval rates of 5.6 g/min with the Piranha using disposable blades and 4.8 g/min with the VersaCut morcellator using reusable blades at a speed setting of 1500 rpm. 9
Similar results were presented by Elshal and colleagues for the Piranha with 6.2 g/min. The VersaCut morcellator merely achieved 2.13 g/min, which turned out to be significantly less compared to the Piranha. In this study, only reusable blades were employed. The median number of morcellations performed per blade was 22 with Piranha and 18 with VersaCut, respectively. 17 One explanation for the higher morcellation rate in this study, compared to our findings, might be the exclusion criteria of diagnosed prostate cancer in the histopathological examination. In prostate carcinoma, the prostate tissue loses its homogeneity if infiltrated with cancer cells and it might therefore be harder to morcellate. Data of speed setting, tract size, and the suction power during surgery are not mentioned in this article, which makes it difficult to find other reasons for the higher morcellation rate compared to our findings.
Prior studies show median retrieval rates of 2.6–6.5 g/min using the Piranha and 1.9–11 g/min using the VersaCut morcellator. 17 More exact and with greater consent are median rates of 3.19 (1.9–4.3) g/min. 12,16,18 In clinical trials, no significant differences between disposable and reusable blades were shown. 17 In our study, we could confirm the postulated median tissue retrieval rate. However, the use of disposable blades at a speed setting of 1500 rpm showed a significantly higher morcellation rate with a median rate of 10 g/min. Technical improvements of the disposable Piranha blade with more aggressive cutting teeth, a modified cutting geometry, and a bigger suction and cutting window for faster morcellation, as it is stated by Richard Wolf on their official website, might also lead to an increase in tissue retrieval rate.
Interestingly, we noticed a decrease in efficacy of tissue retrieval for larger glands (> 100 g) using single-use blades at a speed setting of 1500 rpm in this study. The increasing dullness (“fatigue of material”) of the blades during morcellation is the most likely reason to explain the inverse relationship between tissue weight and morcellation rate. Another explanation would be that in very large prostates, the enucleated tissue might fill out the complete bladder. Due to the operating mode of the morcellator with its oscillating serrated blades, space is needed at the tip of the morcellator for optimal oscillating movement of the blades to morcellate the enucleated tissue efficiently. If the bladder is completely filled out with enucleated tissue, this might impair tissue retrieval.
In addition, the prostate cavity sometimes becomes really big after enucleation. Small parts of the enucleated tissue might drop into the prostatic fossa and have to be morcellated inside the cavity or have to be repositioned into the bladder. These issues are time-consuming and might extend the morcellation process in big prostates.
Several complications during morcellation might occur and may lead to a prolonged morcellation and therefore limit the validity of morcellation rates found in the literature. In our study, one superficial bladder injury during morcellation occurred at a speed setting of 1500 rpm utilizing the Piranha morcellator with a disposable blade. It was bipolar coagulated and did not lead to consequences in postoperative care. In a clinical setting bleeding, a restricted field of vision or technical problems might lead to lower morcellation rates as it is stated in experimental studies.
Ritter and colleagues were the first study group that compared the performance of different morcellators in an experimental setting. Four different morcellators were tested with raw bovine heart in a saline-filled tank as a sample. Raw bovine heart showed most equivalent characteristics to prostate tissue. The Piranha morcellator showed higher morcellation rates compared to the VersaCut morcellator with maximum morcellation rates of 20 (19.3–21.4) g/min and 10.8 (8.2–13.1) g/min, respectively. A Karl Storz prototype and another one of Richard Wolf showed morcellation rates of 9.8 (7.9–10.76) g/min and 38.6 (35.3–42.9) g/min, respectively. 10
There are different possibilities to explain the extraordinarily high morcellation rate: first, the ex vivo setting in a box avoids complications such as intraoperative bleeding, elongated operation time, bad vision, or technical problems that can arise during in vivo morcellation. 10 Second, the homogenous muscle tissue of a bovine heart, whereas prostate glands might contain prostate cancer, abscess, or calculi obstructing the oscillation movement of the blade.
At the same time, Cornu and colleagues tested the same morcellators (Piranha and VersaCut) in an ex vivo model with baked chicken meat. They postulated a morcellation rate for Piranha and VersaCut of 2.5 and 6 g/min, respectively. 19 Due to the findings of Ritter and colleagues, the differences between these two studies are most likely due to the different tissue characteristics of bovine heart and chicken meat. 10
Due to the limits of intravesical morcellation in a realistic setting and its multiple sources of error that can affect the morcellation, we cannot confirm the results of Ritter and colleagues of a median tissue retrieval rate for the Piranha morcellator with 20 g/min in our clinical trial. To verify our findings and make them comparable to other morcellators, it is necessary to perform further studies with different morcellators at different speed settings.
One limitation in this study is the missing analysis of the morcellation rate of reusable blades after each use. This needs to be investigated in further studies to find out at what point reusable blades start to decrease significantly in tissue retrieval rate.
Finally, the morcellator is a complex device with lots of technical challenges. For the urologist as well as for the nurse, it is crucial to know about the instrument and its handling to avoid pitfalls. A reason why the Piranha and VersaCut morcellator showed significantly different morcellation rates in the study of Elshal and colleagues 17 and El Tayeb and colleagues 9 could be the little experience in either one of the morcellators that was used for the experimental study design, but not in the daily clinical routine.
Conclusions
Morcellation after transurethral enucleation of the prostate is an important step for transurethral enucleation procedures. To the best of our knowledge, this is the first study that compares disposable with reusable blades of the Piranha morcellator in a prospective randomized trial. It shows that the Piranha morcellator is safe and efficient for tissue retrieval after ThuVEP using reusable or disposable kinds of blades. No differences could be shown at a speed setting of 850 rpm. However, with increasing oscillation up to 1500 rpm, a significantly higher morcellation rate could be noticed for the disposable blades without a higher incidence of arising complications.
Footnotes
Author Disclosure Statement
For all authors, no competing financial interests exist.