
Abstract
Background:
The learning curve for laparoendoscopic single-incision live donor nephrectomy, which is technically more complex than the multiport, conventional laparoendoscopic approach, is unknown.
Patients and Methods:
In a retrospective cohort study, we analyzed the learning curve of the initial 114 consecutive single-incision laparoendoscopic nephrectomies performed in nonselected live kidney donors.
Results:
Median donor body mass index was 26 kg/m2 (range 20–34). In all, 92% of the nephrectomies were performed on the left side; 18% of the recovered kidneys had multiple renal arteries. Cumulative sum (CUSUM) analysis of operating time (OT) demonstrated that the learning curve was achieved after case 61. For the learning curve phase (Group 1 [cases 1–61]) vs the postlearning phase (Group 2 [cases 62–114]), the difference of the mean OT was 20 minutes (p = 0.05). Mean warm ischemic time in the donors was significantly longer during the learning phase (Group 1, 6 minutes; Group 2, 5 minutes; p = 0.04). Rates of conversions to multiport procedures and of donor complications were not significantly different between Groups 1 and 2. For the recipients, we observed delayed graft function in 2 (2%) cases, no technical graft losses; and 1-year death-censored graft survival was 100% (p = n.s. for all comparisons of Group 1 vs 2).
Conclusions:
Single-incision laparoendoscopic donor nephrectomy had a long learning curve (>60 cases), but resulted in excellent donor and recipient outcomes. The long learning curve has significant implications for the programs and surgeons who contemplate transitioning from multiport to single-incision nephrectomy. Furthermore, our observations are highly relevant for informing the development of training requirements for fellows to be trained in single-incision laparoendoscopic nephrectomy.
Introduction
O
The three published single-incision laparoendoscopic live donor nephrectomy series that encompass a substantial number of cases of each program's initial experience do not allow for solid inferences with respect to the learning curve. 4,6,7 Wang and colleagues reported on their 100 initial consecutive single-incision donors. They did not, however, perform a specific learning curve analysis. 4 Barth and colleagues reported a learning curve of ∼50 cases based on their series that included 135 nonconsecutive single-incision donors. 6 Rigorous analysis of their learning curve was not possible because (1) right-sided nephrectomies had been excluded from the initial part of their series, (2) nephrectomies were performed by two different surgeons who used five different types of single-incision ports, (3) nephrectomies with planned placement of an additional port were included into the definition of single-incision nephrectomy (84% of the initial 50 cases were done with an additional needlescopic port), and (4) cases converted to a standard multiport operation were excluded from the analysis. 6 Last, in the series by Stamatakis and colleagues, 111 single-incision laparoendoscopic nephrectomies were performed by two different surgeons in nonconsecutive donors. 7 Stringent analysis of the learning curve in their study was impeded by the selected nature of donors and by inclusion of 11 (10%) initial donors with planned insertion of an additional laparoendoscopic working port, as well as by routine use of an additional port for all right-sided nephrectomies. None of these series allows one therefore to reach firm conclusions regarding the learning curve.
When we implemented this procedure, we planned to perform all initial cases in consecutive nonselected donors by using only one type of single-incision port—allowing us to study the learning curve of single-incision nephrectomy in the absence of patient selection biases and other confounders. We hypothesized that the learning curve for single-incision nephrectomy would be long due to the intrinsic complexity of minimally invasive live donor nephrectomy coupled with the surgical–technical challenges posed by the single-incision approach.
Patients and Methods
Study population
The 123 consecutive live donor nephrectomies performed by a single surgeon between October 1, 2010, and December 3, 2012, at the University of California, Davis, constitute the basis for our retrospective cohort study.
The primary intent during the study period was for all live donor nephrectomies to be performed using the single-incision technique. However, 9 of the 123 nephrectomies done during the study period were planned to be performed without using the single-incision approach: 7 of them because the surgeon trained to perform the single-incision nephrectomies was not available (i.e., out of town); 1 because the donor refused a periumbilical incision due to personal beliefs (opting for a multiport approach with a suprapubic kidney extraction incision instead); and 1 because the nephrectomy was performed as a planned open procedure due to the donor's known frozen abdomen from a prior perforated appendicitis.
The final study population thus consists of 114 consecutive single-incision live kidney donors.
This study was authorized by the University of California, Davis, Institutional Review Board.
Programmatic setting
Significant clinical experience with laparoendoscopic donor nephrectomy had been accumulated before implementation of the single-incision approach (programmatic experience included >500 laparoendoscopic nephrectomies over 14 years with routine clinical use of the purely laparoendoscopic, hand-assisted transperitoneal, and hand-assisted retroperitoneoscopic techniques). 13,14 Proctoring for the single-incision procedure had occurred at an outside institution that performed a high volume of single-incision donor nephrectomies. Prospective donors were informed regarding the use of the single-incision technique; one donor opted for the single-incision approach (vide supra).
Live donor nephrectomy technique
Single-incision right- and left-sided live donor nephrectomies were performed as previously described. 4,8,15 Briefly, we placed a GelPOINT Access Platform (Applied Medical Corporation, Rancho Santa Margarita, CA) into a 5-cm periumbilical vertical midline incision. After complete renal dissection, renal artery and vein were sequentially stapled and cut with an ENDO GIA™ 30 stapler (Covidien, Mansfield, MA).
Conversion to a multiport procedure was done by inserting an ipsilateral 5-mm port subcostally through the posterior axillary line. When necessary, we converted to conventional hand-assisted laparoendoscopic nephrectomy by enlarging the periumbilical incision to insert a hand port (GelPort; Applied Medical Corporation) and by adding two paramedian 12-mm ports. 14 Conversion to open nephrectomy was done by extending the periumbilical vertical incision into a full open midline incision.
Follow-up
After hospital discharge, we followed the donors in our clinic until completion of wound healing and surgical recovery. We contacted patients at 6 months, 1 year, and 2 years for follow-up.
Data acquisition
We obtained donor and recipient demographics and outcomes from the patients' electronic medical records. Donor warm ischemia time (kidney extraction time) was defined as time between renal artery stapling and placement of the kidney on ice.
In all, 15 (13%) kidneys were shipped elsewhere for paired exchange transplantation. We routinely obtained early follow-up information on these grafts regarding vascular complications, perioperative technical graft losses, and delayed function from the receiving centers.
Learning curve analysis
First, we assessed the learning curve quantitatively by cumulative sum (CUSUM) analysis of the operating times (OTs) for all 114 cases, as described by Haas and colleagues. 11,16,17 We defined OT as the time between skin incision and skin closure. The CUSUM for the OT was calculated as the running total of the differences between the individual OTs and the mean for all OTs. We ordered all 114 cases chronologically. The CUSUM for the OT of the first case was, for instance, the difference between the actual OT for the first case and the mean OT for all cases. The CUSUM for OT of the second case was the previous case's OT CUSUM added to the difference between the OT for the second case and the mean OT for all cases. This iterative process was continued until the CUSUM for OT of the last case was calculated as zero. 11,17
Next, to ascertain the absence of donor selection bias, we statistically compared donor and graft characteristics during the learning curve vs the postlearning curve phase as identified by CUSUM analysis.
We then quantitatively analyzed donor outcomes during the learning curve vs postlearning curve phase as identified by the CUSUM analysis. Donor outcomes included warm ischemia time as well as potentially learning curve-associated surgical conversions (i.e., from a single incision to a multiport procedure [defined as insertion of one or more standard laparoendoscopic ports or of a hand port] or direct conversion from a single incision to an open procedure) and donor complications (renovascular injury, injury to extrarenal organs, blood transfusion, reoperation, and hospital readmission, as well as early [e.g., infection, seroma] and late [e.g., incisional hernia] wound complications). We also created a scatter plot to further assess for any potential temporal relationship patterns between timing and incidence of these aforementioned donor conversions and complications and the cumulative experience with the single-incision procedure.
Last, we analyzed recipient outcomes for the learning curve vs the postlearning curve phases identified by CUSUM analysis. The recipient outcomes that were studied included vascular graft complications and ureteral complications (e.g., strictures), as well as short- and long-term graft function and survival.
Statistical analysis
We analyzed categorical variables using the chi-square test and Fisher's exact test. We analyzed continuous variables using the t-test (in case of equal variances) and the Welch test (in case of unequal variances). Graft and patient survival was calculated according to Kaplan–Meier. For all statistical tests, the significance level was set at 0.05. Statistical calculations were done using MedCalc Statistical Software, version 14.12.0 (MedCalc Software bvba, Ostend, Belgium).
Results
Baseline donor demographics and graft characteristics
Of the 114 donors, 73 (64%) were women. Median donor age was 45 years (range 21–66 years). Median donor weight was 74 kg (range 49–103 kg) and median body mass index was 26 kg/m2 (range 20–34 kg/m2). We performed left-sided nephrectomy in 92% of all donors and noted multiple renal arteries in 18% of all grafts.
Learning curve assessment
CUSUM analysis of OT
Overall mean OT was 246 minutes (range 150–565 minutes). Analysis of the CUSUM for OT demonstrated that the learning curve reached a plateau phase between cases 50 and 61. The consistent decline of CUSUM for OT after case 61 indicated the achievement of the learning curve at that point (Fig. 1).
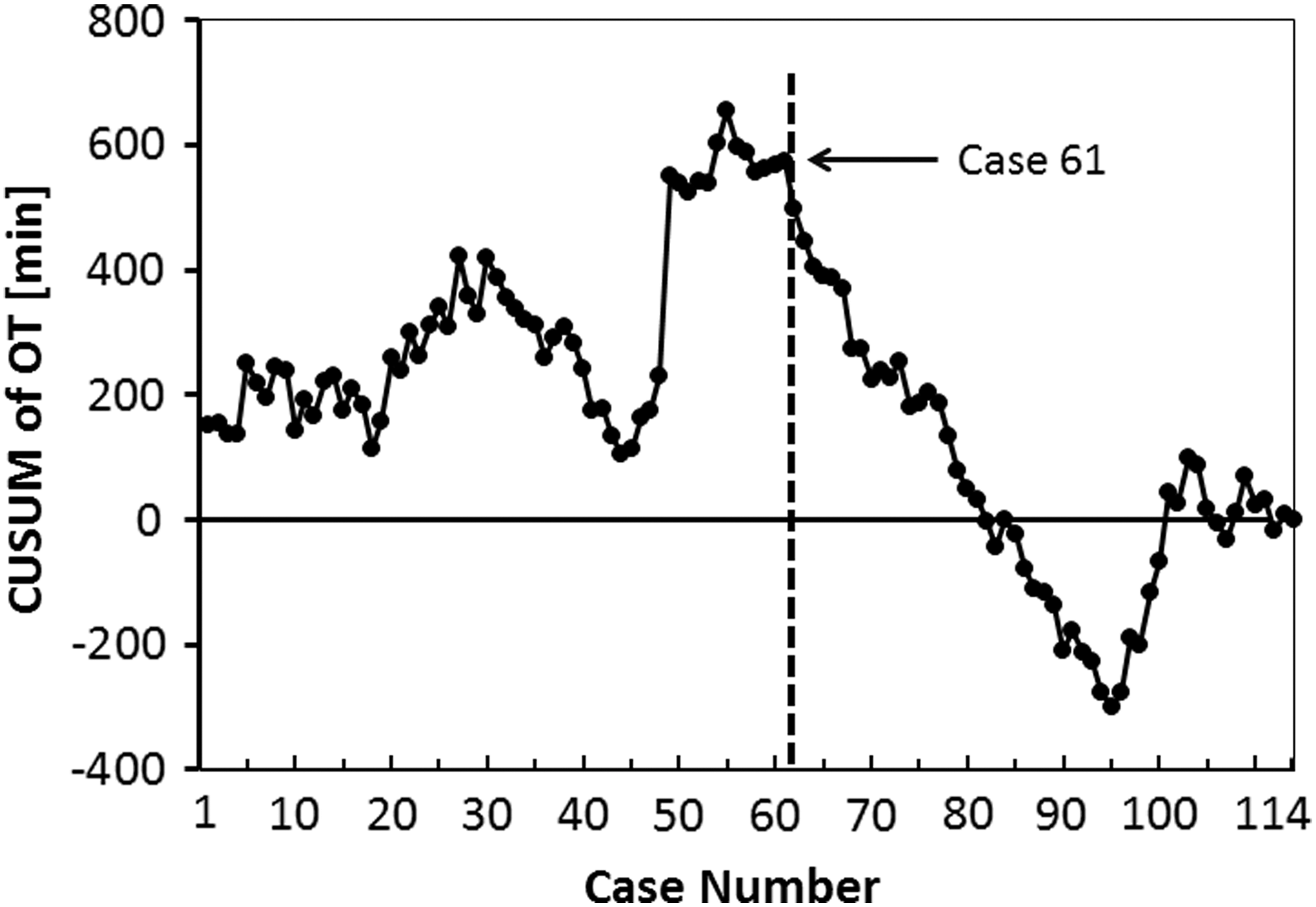
CUSUM analysis of OT. OT = operating time.
Donor and graft characteristics according to learning curve phase
Donor and graft characteristics were not significantly different for the learning curve group (n = 61, Group 1) vs postlearning curve group (n = 53, Group 2) (Table 1).
p = not significant for all intergroup comparisons.
Perioperative donor outcomes
In Group 2, we observed a shorter mean warm ischemic time (p = 0.04) and OT (p = 0.05) (Table 2).
p = 0.04 for comparison of Group 1 vs 2.
p = 0.05 for comparison of Group 1 vs 2.
OT = operating time.
Overall, we noted seven conversions to a multiport procedure directly associated with the single-incision operation. In Group 1, three donors required insertion of an additional 5-mm port (conversion to a purely laparoendoscopic multiport procedure) and three donors required conversion to hand-assisted nephrectomy. In Group 2, one single-incision donor nephrectomy was converted to a hand-assisted procedure.
Furthermore, one of the three donors in Group 1 whose single-incision nephrectomy had been nonurgently converted to a hand-assisted procedure required later during the course of the hand-assisted operation conversion from hand-assisted to open nephrectomy as well as a blood transfusion. One of the superficial wound complications in Group 1 required a late superficial operative reintervention to remove subcutaneous granulation tissue. We noted one early acute fascial dehiscence in Group 2, which occurred in a patient with a single-incision nephrectomy done through a prior umbilical hernia repair site. We observed late incisional hernias in 3 (3%) donors at their umbilical incision site; all have undergone elective hernia repair (Table 3).
p = not significant for all intergroup comparisons.
Data given are based on the 99 recipients (52, Group 1; 47, Group 2) transplanted and followed at our center.
The CO2 pneumothorax and psoas hematoma that were both observed in Group 2 each resolved spontaneously without intervention (Table 2).
Scatter plot analysis of the aforementioned conversions and complications did not suggest clustering (Fig. 2).
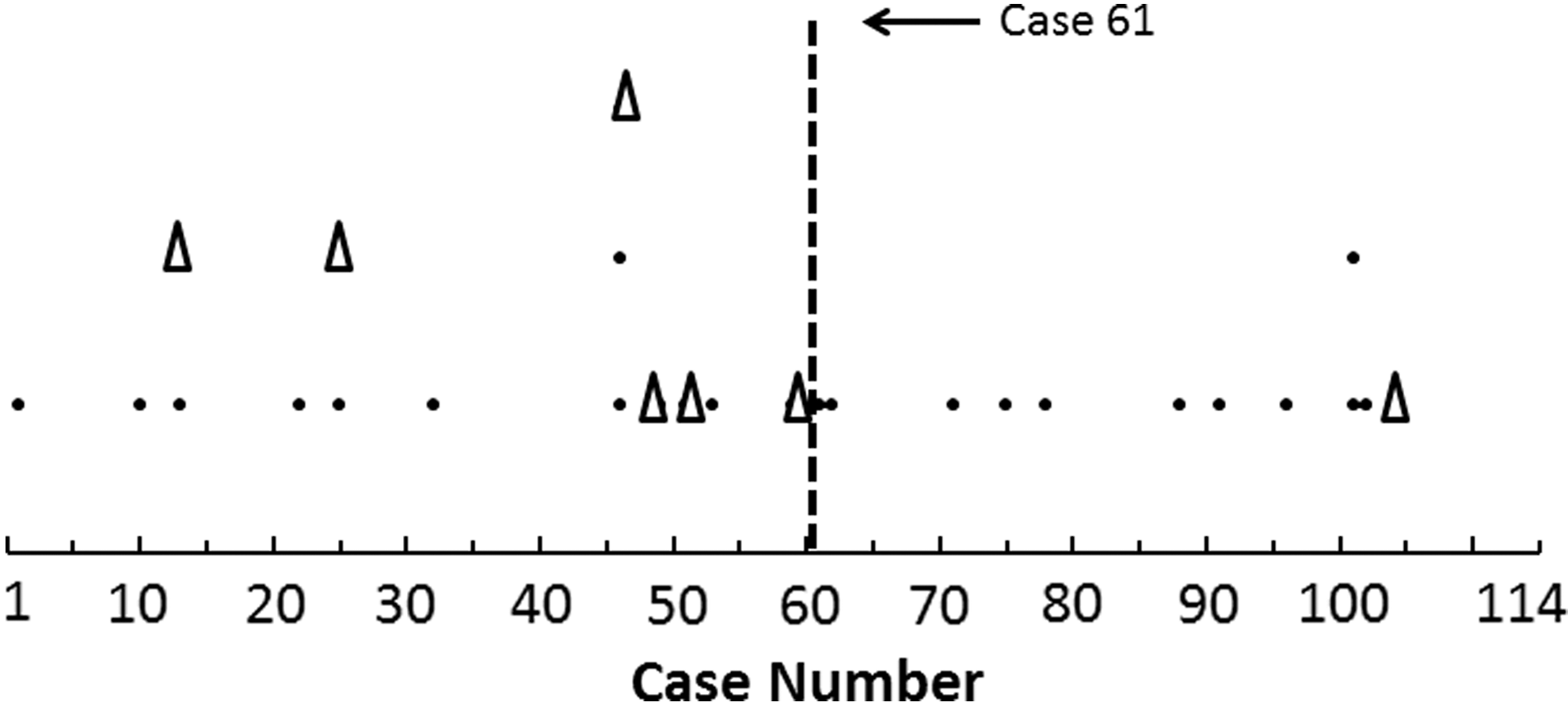
Single-incision nephrectomy-associated conversions to multiport nephrectomy (purely laparoscopic or hand-assisted; open triangles) and complications (incl. blood transfusion requirement, organ or vascular injury, reoperation within 30 days, wound and other complications, and hospital readmission within 30 days; black dots) according to case number. Each symbol represents one conversion or complication event (note that for some cases, there was more than one event).
Recipient outcomes
Overall, delayed graft function rate was 2%, and ureteral complication rate was 2% (all strictures). For the recipients at our institution, we observed 8 (8%) graft losses between 8 and 40 months post-transplant; death-censored 1-year graft survival was 100% (Table 3).
Discussion
Single-incision laparoendoscopic donor nephrectomy has emerged as an alternative to conventional multiport nephrectomy. 4,6 –8 In a recent randomized trial that compared single-incision vs conventional multiport nephrectomy, operative parameters as well as recovery and postdonation donor satisfaction scores were similar between groups. 8 Importantly, however, a systematic review of single-incision laparoendoscopic surgery in general (that included both clinical and training laboratory studies) underscored the very specific skill sets required for, and ergonomic demands associated with, single-incision laparoendoscopic procedures. 12 Furthermore, the authors of that review concluded that it may therefore not be possible to directly adapt the skills required for single-incision surgery from a surgeon's existing (multiport) laparoendoscopic surgical experience. 12 It is therefore not surprising that rather long learning curves have been described for complex laparoendoscopic procedures when transitioning to the single-incision approach. 9 –12
For single-incision live donor nephrectomy, however, the learning curve remains largely unknown. Importantly, our donors were nonselected (as underscored by similar donor demographics and baseline characteristics in Groups 1 and 2), and we employed only one type of surgical single-incision port.
Our outcomes suggest that the learning curve for this complex single-incision laparoendoscopic procedure is long (i.e., >60 cases) in spite of the surgeon's extensive prior experience over the course of more than one decade with three different modifications of multiport laparoendoscopic donor nephrectomy. The long learning curve that we observed appears to be related—based on our experience—to the more challenging exposure and perinephric dissection that are both associated with the single-incision technique. They are at least, in part, a result of (1) the inability to significantly triangulate the laparoscopic instruments and camera and (2) the increased distance between the (umbilical) single-incision laparoscopic instrument insertion site and the operative area of interest. These observations are mirrored by the learning curve analysis for single-incision laparoendoscopic radical nephrectomy by Park and colleagues. They observed the longest learning curve for the kidney mobilization phase, followed by the medial retraction of the colon. In their experience, the learning curve was shortest for the hilar dissection phase. 18 Finally, the direct clinical consequences of the observed absolute differences for donor warm ischemia time and operative time in our series may be relatively limited. Nonetheless, our observations are also consistent with the learning curve-related findings that have been described for other, similarly complex laparoendoscopic procedures. 9,11,12
Our 15% complication rate observed during the initial 61 cases is in line with the complication rates reported by other major programs that perform donor nephrectomies. In their randomized prospective study, Aull and colleagues reported a 12% complication rate for the single-incision study arm—which included only donor nephrectomies done after the learning curve had already been achieved. 8 Similarly, Stamatakis and colleagues reported 16% complications in their initial 102 single-incision laparoendoscopic donors. We also found that donor and recipient complication rates varied only insignificantly over time. This finding may at least, in part, be due to the low absolute frequency of these complications (which renders it more difficult to demonstrate any statistically significant difference over time). 13,14,19 –23
Our findings have several potential implications both for the implementation of this technique by surgeons already performing routinely multiport laparoendoscopic nephrectomy and for the determination of single-incision donor nephrectomy training requirements for transplant surgery fellows. First, with regard to the adoption of this technique by surgeons already experienced in multiport laparoendoscopic donor nephrectomy, it is important to note that laparoendoscopic donor nephrectomy is a low- to intermediate-volume procedure at most centers. For instance, in 2014, only 23 (10%) of the 230 live donor kidney transplant programs in the United States did perform more than 60 live donor transplants. 24 Assuming that at least two surgeons share the nephrectomies in these larger programs and given that the learning curve is at least 60 procedures long, it may take 2 years or longer even for those higher volume programs to overcome the learning curve (under the assumption that all cases be performed using the single-incision technique).
Second, further study is necessary to determine the optimal timing for learning the single-incision technique (e.g., during fellowship training vs after already having practiced multiport laparoendoscopic nephrectomy for some time). A recent analysis of the learning curve for multiport laparoscopic donor nephrectomy suggested that transplant fellows may require more than 35 multiport donor nephrectomies to achieve surgical proficiency with the conventional technique. 25 The complexity and the long learning curve associated with single-incision donor nephrectomy in our study suggest that it might be highly beneficial to first become proficient with conventional multiport donor nephrectomy before contemplating training in single-incision nephrectomy.
Finally, future studies should explore whether the learning curve for single-incision nephrectomy could be shortened by training in the surgical simulation laboratory or by having two laparoendoscopically experienced surgeons assist each other during the initial cases performed with this new technique.
Our study has several limitations. We were not able to determine the learning curve for surgeons with only limited laparoendoscopic experience or no laparoendoscopic experience at all. Furthermore, given the low absolute frequency of very serious adverse events in laparoendoscopic donor nephrectomy (e.g., blood transfusion, relaparotomy), the statistical power of our analysis with respect to analyzing the incidence of these serious events over time was limited. 13,14,19 –23 Finally, our study was retrospective. Nonetheless, we believe that we were able to avoid the main issues typically associated with that study design, namely selection bias and intersurgeon variability, as all procedures were performed in consecutive nonselected patients by one surgeon.
We conclude that single-incision laparoendoscopic live donor nephrectomy has a long learning curve that is typical of complex laparoendoscopic procedures when these are transitioned to a single-incision approach. This finding has significant implications for surgeons who consider using this technique and for determining training requirements for residents and fellows who are to be trained in single-incision nephrectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.