
Abstract
Objective:
Increasing fluid intake to achieve a urine volume (UV) of >2.5 L/day decreases stone events. We assessed compliance rates and demographic and clinical variables associated with increased fluid intake and UV in patients with urolithiasis following dietary counseling.
Materials and Methods:
In a retrospective study, patients with a low baseline UV (<2.5 L/day) on an initial 24-hour urine collection during metabolic stone evaluation were identified between 2010 and 2015. Patients received detailed standardized dietary counseling, including increasing fluid intake to >3 L/day and titrating it to achieve UV >2.5 L/day. A follow-up 24-hour urine collection was performed at 6 months (FU1) and 18 months (FU2) to assess compliance (UV >2.5 L/day) and predictors associated with it.
Results:
Our cohort contained 363 patients, 53.4% men and 46.6% women. The mean UV of baseline, FU1, and FU2 urine collections was 1.63, 2.52, and 2.48 L, respectively. The compliance rate of obtaining UV of >2.5 L was 50.1% at 6 months. On logistic regression, male sex (odds ratio [OR] 3.27, 95% confidence interval [CI] 1.94, 5.52, p < 0.001), urolithiasis-related procedures such as ureteroscopy (OR 2.31, 95% CI 1.20, 4.42, p = 0.01) or percutaneous nephrolithotomy (OR 3.48, 95% CI 1.58, 7.63, p = 0.002), and baseline 24-hour UV >1 L (OR 3.00, 95% CI 1.02, 8.76, p = 0.04) were associated with greater odds of compliance. Age >58 years (OR 0.39, 95% CI 0.20, 0.75, p = 0.005) and presence of lower urinary tract symptoms (OR 0.50, 95% CI 0.26, 0.95, p = 0.03) were associated with lower odds of compliance. Ethnicity, body mass index, renal function, marital status, renal stone burden, stone type, and household income were not associated with compliance.
Conclusions:
In stone formers, compliance to fluid intake recommendations as measured by 24-hour UV is roughly 50%. Understanding risk factors for noncompliance, especially in at risk patients, can be used for quality improvement initiatives and reducing stone events.
Introduction
N
Several studies have demonstrated the effectiveness of increased fluid intake in reducing stone recurrences. 6,7 This is shown to be a cost-effective prevention strategy for recurrent stones. 8 The American Urological Association Medical Management of Kidney Stone Guidelines recommend a minimum urine output of 2.5 L/day in stone formers. 9 Despite these medical and cost benefits, patients are seldom able to achieve an adequate urine output in clinical practice. Furthermore, compliance and predictors of persistent low urine output in patients with nephrolithiasis are poorly understood.
Using a sample of patients with nephrolithiasis from a specialized stone clinic, our goal was to assess compliance with high fluid intake and urine volume (UV) based on 24-hour urine collection following dietary counseling, as well as investigate demographic and clinical factors associated with compliance.
Materials and Methods
All first-time stone formers presenting to our tertiary hospital stone clinic from January 1, 2010 to December 31, 2015 were reviewed for this study. As part of our standard first-time stone evaluation, patients were recommended to undergo an initial 24-hour urine collection on a typical diet without dietary counseling. This was considered the baseline 24-hour urine collection. Patients who completed this collection and had baseline low urine output of <2.5 L/24-hour were included.
All included patients received detailed verbal and standardized written dietary instructions for a high fluid diet to achieve daily UV of more 2.5 L. Specifically, patients were educated on benefits of high UV, and instructed to consume at least 3 L of fluid daily, and increase it to 3.5 L daily if participating in an exercise program. Water with or without lemon juice was the primarily recommended fluid, with the latter being an adjunct to encourage fluid consumption. Patients were advised on consuming eight to ten 12 oz. glasses of fluids per day, splitting them up in the morning, afternoon, and evening. Other allowed fluids included one to two cups of coffee a day, diet white sodas such as Ginger Ale, 7-up and Sprite, fruit juices, or flavored seltzer. While all fluid consumption was encouraged in general, intake of specific fluids such as sweetened colas and teas was advised based on stone type and 24-hour urine chemistries, and limiting to 8–12 oz. per day in some cases. To check their progress, patients were asked to measure their UV for a period of 24 consecutive hours for the first few months, monitor their urine color, and titrate their fluid intake based on patient factors such as physical activity levels and illness, as well as weather conditions, to achieve the desired daily UV.
A follow-up 24-hour urine collection was recommended at 6 months (FU1) and 18 months (FU2) from baseline. Only the first three 24-hour collections (baseline, FU1, FU2) were included in this study. Compliance with fluid recommendation was defined as UV >2.5 L on FU1 and FU2. All 24-hour collections were analyzed by Litholink Corporation, Chicago IL.
Patient demographics, including age, sex, body mass index, marital status, household income based on Zone Improvement Plan codes, and ethnicity, were recorded. In addition, clinical factors such as initial and residual stone burden (≥2 mm), documented history of lower urinary tract symptoms (LUTS; urgency, frequency, nocturia, dribbling, weak stream, hesitancy, intermittency, and incomplete emptying due to conditions such as bladder outlet obstruction, overactive bladder, urgency, and frequency syndrome), and medical and surgical management of stones were also analyzed.
Patients were excluded if they were <16 years old, had stones associated with an anatomic abnormality (e.g., horseshoe kidney and medullary sponge kidney), underlying complex metabolic disease (e.g., renal tubular acidosis and hyperparathyroidism), or diarrheal states (e.g., inflammatory bowel disease, irritable bowel syndrome, and gastric bypass surgery). In addition, patients with inadequate or excess urine collection based on 24-hour urine creatinine per kilogram (less than 15 mg or more than 20 mg in women and less than 18 mg or more than 25 mg in men) were excluded. This parameter was used because it is easy to interpret, has recommended ranges, provides a conservative estimate of adequate urine collection, and has been used to determine inadequate or excess 24-hour urine collection in earlier studies. 10,11
Categorical ratios and percentages were compared using Pearson's chi-squared test, and continuous variables were compared using the Mann–Whitney test. A binomial logistic regression model was examined to assess factors associated with compliance on FU1. Statistical significance was set at p < 0.05. All statistical analyses were conducted using STATA v13 software. The Northwestern University Institutional Review Board approved this study (STU00056087).
Results
Demographic data
In total, 363 patients were included—194 (53.4%) men and 169 (46.6%) women. The median patient age was 51 years (interquartile range 38–61). Three hundred thirty-six (92.8%) patients supplied both their baseline and FU1 24-hour urine collections on either a weekday or alternatively on a weekend day. The majority of patients were overweight, white, and married (Table 1). Concomitant LUTS due to urine outflow or storage dysfunction was present in 71 (19.6%) patients. Most patients presented with multiple stones and required surgical intervention for nephrolithiasis before evaluation. Calcium oxalate was the most common stone type. Majority of the patents were stone free (defined as residual stone burden <2 mm) following conservative or operative management. Patient clinical and stone specific details are listed in Table 2.
BMI = body mass index; CKD = chronic kidney disease; GFR = glomerular filtration rate.
Includes thiazides, citrates, and allopurinol for nephrolithiasis.
LUTS = lower urinary tract symptoms; PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy; URS = ureteroscopy.
Compliance based on initial 24-hour UV
The mean UV at baseline and FU1 24-hour collections were 1.63 ± 0.44 L and 2.52 ± 0.55 L, respectively. FU1 collections were submitted at a median of 175 days from baseline collection date. In addition, 208 patients submitted a second 24-hour urine collection (FU2) at a median of 407 days from FU1, with a mean volume of 2.47 ± 1.09 L.
On their baseline 24-hour collection, 30 (8.3%) patients had a volume of <1 L, 257 (70.8%) had a volume between 1 and 2 L, and 76 (20.9%) had volume between 2 and 2.5 L. The overall compliance of achieving a UV >2.5 L following dietary counseling on 6-month follow-up 24-hour collection (FU1) was only 50.1% (180/363) and dropped to 47.5% at 18-month follow-up (FU2) (Table 3). The mean increase in UV in compliant patients was 1.25 ± 0.81 L, whereas the change in noncompliant patients was only 0.15 ± 0.52 L. Of the 208 patients who submitted a FU2, 76 (36.5%) had both FU1 and FU2 below 2.5 L, whereas 80 (38.46%) had both FU1 and FU2 with greater than 2.5 L. Nineteen patients (9.1%) had FU1 < 2.5 L and FU2 > 2.5 L while 33 (15.9%) had FU1 > 2.5 L and FU2 < 2.5 L indicating regression of compliance.
FU1 6-month 24-hour UV; FU2 18-month 24-hour UV.
Only six patients (20%) with a UV of <1 L achieved compliance on FU1 compared with 129 patients (50.2%) with a UV between 1 and 2 L and 47 patients (61.8%) with a UV between 2 and 2.5 L (p = 0.001). In general, patients with a higher baseline UV had a higher FU1 volume (Fig. 1).
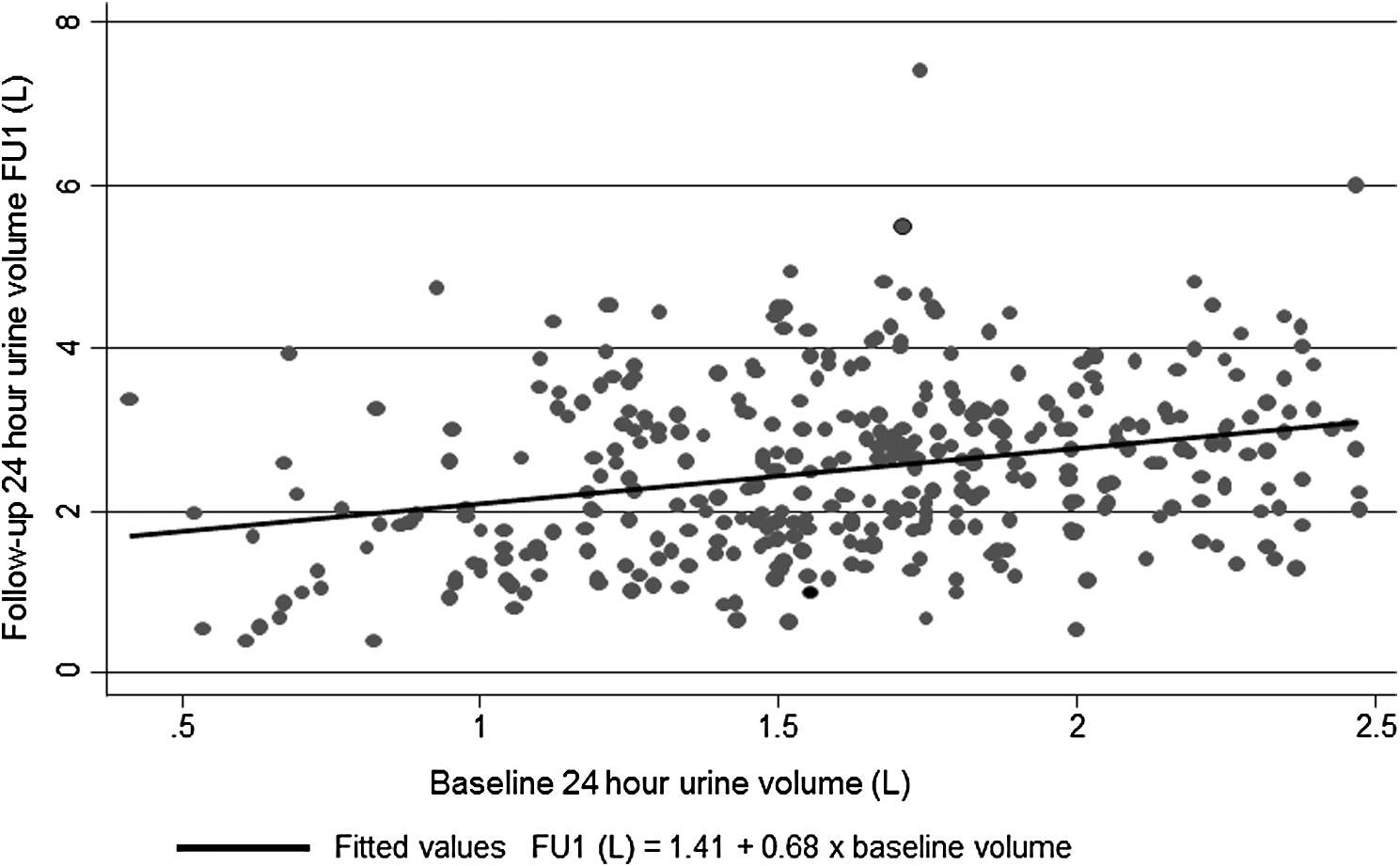
Follow-up 6-month 24-hour UV FU1 (y-axis) based on baseline UV (x-axis). UV = urine volume.
Factors associated with compliance on 24-hour UVs
There was no significant difference in compliance rates based on initial stone burden: 50.5% (n = 88) for 0–5 mm stone(s) vs 53.1% (n = 59) for 5.1–10 mm stone(s) vs 44.8% (n = 35) for >10 mm stone(s) (p = 0.527). Similarly, there was no difference in compliance based on single vs multiple stones at presentation—48.5% (n = 100) vs 52.2% (n = 82, p = 0.48). Complete unadjusted rates of compliance for each variable are listed in Table 4.
Thiazide/citrate/allopurinol based drugs.
AA = African American; OR = odds ratio.
Regression analysis was performed to examine factors associated with compliance (defined as UV >2.5 L/24 hours) on FU1 24-hour urine collection. Compared with patients with a baseline 24-hour UV <1 L, those with 1–2 L (odds ratio [OR] 3.00, 95% confidence interval [CI] 1.02, 8.76) and 2 + L (OR 4.83, 95% CI 1.48, 15.70) had stronger associations with achieving compliance. Male sex (OR 3.27, 95% CI 1.94, 5.52) was associated with higher odds of compliance, whereas patients older than 58 (OR 0.39, 95% CI 0.20, 0.75) were less likely to reach compliance compared with younger patients (ages 16–43). Patients with a documented history of LUTS (OR 0.50, 95% CI 0.26, 0.95) were less likely to reach compliance. Compared with patients who did not undergo any surgical intervention for their stones (i.e., managed conservatively), patients who had stones managed with either percutaneous nephrolithotomy (PCNL) (OR 3.48, 95% CI 1.58, 7.63) or ureteroscopy (OR 2.31, 95% CI 1.20, 4.42) were more likely to reach compliance. Patient ethnicity, marital status, obesity, renal function, and household income were not associated with compliance. Similarly, residual stone burden, stone type, and use of lithiasis related medications, such as thiazides, urine alkalinizing agents (e.g., citrates), and allopurinol, were not associated with compliance (Table 4).
Discussion
Increased fluid intake and urine output protect against nephrolithiasis by reducing supersaturation of calcium oxalate, calcium phosphate, and uric acid. 12 In a systematic review, high fluid intake reduced risk of nephrolithiasis recurrence by 60%. 13 Borghi and colleagues demonstrated that the group randomized to a high fluid diet with a daily UV >2 L had fewer recurrences at 5 years. 6 Similarly, patients who underwent extracorporeal shockwave lithotripsy had fewer recurrences when randomized to high fluid intake diet to achieve a UV of >2.5 L/day. 7 While benefits of increased fluid intake in reducing the risk of nephrolithiasis are well established, individual compliance rates with high fluid intake and urine output are poorly studied. van Drongelen and colleagues assessed compliance to dietary therapy, including fluid intake, based on patient reported questionnaires. 14 Patients were deemed compliant if they described the original prescribed therapy during their initial visit. The overall compliance rate was 36% at 5 years, however, 64.8% for daily fluid consumption >2 L/day.
In our study, we investigate compliance rates and predictors of compliance with fluid intake in patients with nephrolithiasis using their 24-hour UV. We used this parameter to assess compliance since it is an objective measure that is known to correlate with concurrent fluid intake 15 and is a part of stone management guidelines. 9 The initial compliance rate at the 6-month (FU1) visit was only 50.1%. At the 18-month visit (FU2), 47.5% were compliant with a UV >2.5 L; however, only 38.5% of patients remained compliant at both visits. We assessed characteristic features of compliant and noncompliant patients. Patients older than 58 years were less likely to be noncompliant. This may be related to increased prevalence of bladder outlet obstruction, overactive bladder, and cardiovascular disease that might be exacerbated by increased fluid intake. We found that patients with coexisting LUTS at the time of presentation were less likely to be compliant with fluid intake. Moreover, alteration in the physiologic homeostasis involving thirst in the elderly can lead to decreased water intake 16 and also affect compliance. Men were more compliant, consistent with earlier findings. 14 The compliance rates were also related to the invasiveness of the surgical intervention. The morbidity associated with ureteroscopy and PCNL may incentivize patients to adhere to dietary recommendations to prevent recurrences and subsequent procedures. Interestingly, the initial and residual stone burden did not affect compliance with fluid intake and UV.
Barriers to increasing fluid intake among kidney stone formers have been assessed. 17 These include absence of awareness, not remembering to drink, dislike for the taste of water, absence of thirst, need to void, and disruption of work. In our study, compliance was based on initial UV, and patients starting with a higher UV were more likely to be compliant at their follow-up visits. Importantly, the OR for compliance in patients with a baseline UV >2 L was 4.8 compared with patients with a volume of <1 L. This is partly explained by the fact that some barriers to increasing fluid intake are personal habits, which may be difficult to overcome. Therefore, patients with a baseline 24-hour UV <1 L may require additional supports and encouragement in achieving compliance with fluid intake.
To be effective in increasing fluid intake in patients with stones, it is essential to address these barriers at an individual level. Tarplin and colleagues found that unsuccessful patients were less aware of future stone risk and less likely to be counseled by an urologist. 18 Hence, it is essential that emphasis is placed on fluid intake counseling, especially since patients are more willing to adhere to a dietary plan as opposed to a medication regimen. Dauw and colleagues found an adherence rate of only 30.3% with preventive pharmacologic therapy in kidney stone patients, highlighting the importance of dietary management in these patients. 19
The retrospective nature and small sample size of our study are limitations. In addition, our cohort of patients from a specialized stone clinic may not be applicable to the general population. In addition, we were not able to control for change in UV due to seasonal variations, which may affect extrarenal fluid losses and, hence, need to be assessed in future studies. We encourage patients to compensate for this by titrating their fluid intake and monitoring their urine color. Similarly, there can be intrasubject variability in daily fluid intake depending on whether the patient collected their urine on a weekday or weekend. In our study, 92.8% of patients collected both their baseline and FU1 urine samples either on a weekday or a weekend, hence, limiting the “workday” vs “weekend” effect on fluid consumption. Finally, we did not have information on types and quantities of fluids consumed by patients, which may highlight differences in dietary habits between compliant and noncompliant patients. Accurately recorded daily patient fluid intake information would supplement the 24-hour UV in assessing compliance as well.
Additional strategies may need to be adopted for improving adherence with fluid intake in at risk demographics as identified in our study. This can include patient self-monitoring tools such as self-administered 24-hour urine recording and use of urine dipsticks to measure urine specific gravity. 20,21 Use of phone based technologies that remind patients to drink fluids and providing water bottles may help in achieving compliance. 22,23 Diversifying the types of fluids consumed may also aid in boosting the overall intake and help achieve the desired UV. Regular patient contact with telephone follow-up may also be necessary in this group.
Conclusions
Compliance with fluid intake and UV in first-time stone patients is about 50%. Patients with a UV <1 L at baseline, female sex, age >58 years, and patients with LUTS are less likely to achieve the desired daily UV of >2.5 L despite dietary counseling, whereas patients undergoing an invasive surgical intervention are more likely to be compliant. The importance of increasing fluid intake to reduce stone recurrences needs to be emphasized at the time of dietary counseling, especially with at risk demographics, and closer follow-up may be required to ensure compliance.
Footnotes
Author Disclosure Statement
No competing financial interests exist.