
Abstract
Objective:
To describe the technique and outcomes of supine percutaneous nephrolithotomy (PCNL) in the Galdako-modified Valdivia position.
Materials and Methods:
Prospective data were collected from 303 patients undergoing PCNL in the Galdako-modified Valdivia position at our institution between 2007 and 2015. We report our technique with outcomes of operative times, stone-free rate (SFR), and complications.
Results:
A total of 202 solitary stones with a mean size of 17.19 ± 5.82 mm, 42 stones in multiple calices, and 57 staghorns were treated. Mean operative time was 79.79 ± 35.72 minutes. A total of 244/303 (80.5%) patients had clearance or <2 mm stone on postoperative CT. Minor complications (Clavien–Dindo Classification [CDC] 1–2) occurred in 59 (19.5%) cases and major complications (CDC ≥3) occurred in 22 (7.3%) cases. Five (1.7%) cases required postoperative blood transfusion for bleeding complications.
Conclusion:
We demonstrate that PCNL in a high-volume center to be safe and efficacious in the Galdalko-modified Valdivia position. We show equivalent SFR and complication rates to large studies of prone PCNL, with potential to decrease operative time. In particular, supine position is optimum for obese or high-risk patients with complex stone disease, because of ease of positioning and lower theoretical risk of anesthetic complications.
Introduction
P
Two earlier meta-analyses showed supine PCNL to be as effective as prone PCNL with regard to stone-free rates, complications, and length of hospital stay. The major advantage identified in these studies was reduction in operative time. 3,4
Since the publication of these two meta-analyses, many studies have been published that have yielded less consistent outcomes between the advantages of supine PCNL vs prone PCNL. The most recent updates to these meta-analyses present conflicting data regarding stone-free rate (SFR), but suggest lower incidence of postoperative fever and blood transfusion. 6 –8 In addition, supine PCNL requires more lateral displacement of the renal puncture site than the prone position. This theoretically may increase the probability of visceral injury and trauma to the intrarenal vessels. 9 However, this is not seen in practice. 6 The debate continues as to which position is the optimum for PCNL.
In our unit we perform all PCNLs in the supine Galdako-modified Valdivia position 1 (Fig. 1) and report our technique and outcomes in this article. The authors aim to demonstrate supine PCNL as a safe and efficacious technique.

Patient positioning.
Materials and Methods
Prospective data were collected on 303 consecutive patients undergoing PCNL at our institution between February 2007 and July 2015. All patients were discussed at a dedicated stone multidisciplinary team meeting, with a consultant urologist and uroradiologist present. All patients underwent preoperative assessment in a dedicated stone clinic, with clinical examination, routine laboratory investigation, and CT imaging.
Demographic, clinical, and stone data were recorded. Comorbid status was recorded using the Charlson comorbidity index (CCI). 10 Stone size was recorded as maximal diameter for single stones and maximal diameter of the largest stone for multiple stones. Mean stone density was measured in HU. In addition, stones were classified according to the Guy's Stone Score (GSS). 11
Surgery was carried out by three consultant endourologists in the Galdako-modified Valdivia position (Fig. 1). The authors use a 3-L air-filled irrigation bag to elevate the patients flank as this can gradually be deflated to attain optimum position. The standard technique constituted access guidance with ultrasound, fluoroscopy, or a combination of both by a dedicated uroradiologist (Fig. 2). A 21 g Chiba needle (Cook Medical, Bloomington, IN) and 0.018 inch guidewire were primarily used for access. This was exchanged for an Amplatz Super Stiff™ (Boston Scientific, Natick, MA) safety wire, passed to the bladder, and, where possible, tract dilatation performed using a Nephromax™ (Boston Scientific) or Ultraxx™ (Cook Medical) balloon dilator. Simultaneous cystoscopy and retrograde contrast study were performed by an assistant.

Ultrasound-guided puncture. Margins: posterior axillary line, 12th rib, Iliac C.
A 30F amplatz sheath was inserted and nephroscopy performed. The authors use a Karl Storz Hopkins® wide-angled 6° Nephroscope with 24F or 26F Sheath at 19 or 25 cm length (Karl Storz, Tuttlingen, Germany) as standard. If flexible nephroscopy was required, an Olympus Flexible Cysto-nephro Fibrescope CYF-5 (Olympus Corporation, Tokyo, Japan) was used. Swiss Lithoclast Master® (Electro Medical Systems, Nyon, Switzerland) was used preferentially for stone fragmentation where appropriate. When indicated, ECIRS was carried out by an assisting surgeon using the digital Flex XC (Karl Storz) flexible ureterorenoscope (Fig. 3).
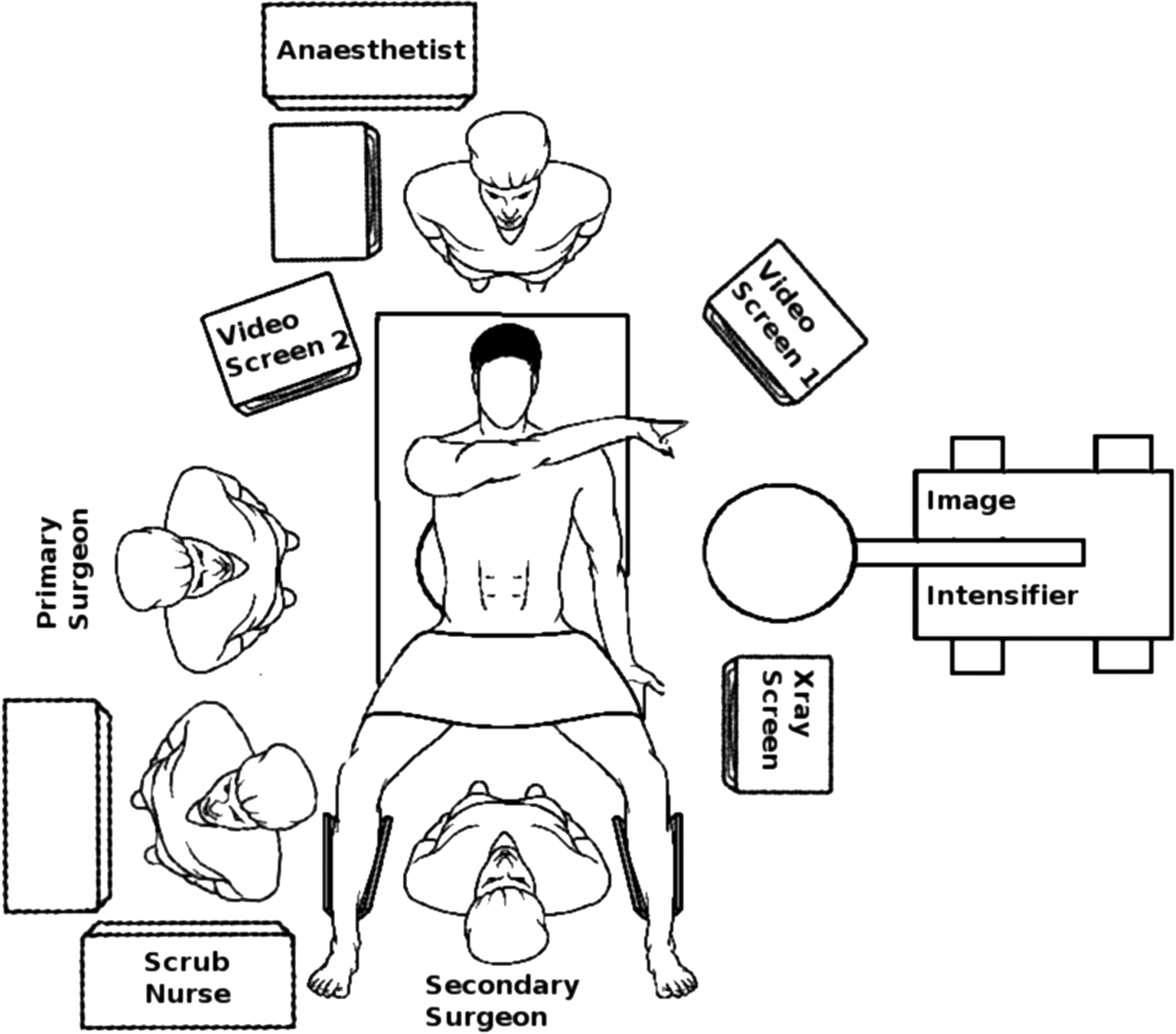
Equipment and theater configuration.
A 10F locking nephrostomy tube on open drainage was sited at completion of the procedure, and in selected (Impacted pelvoureteral junction or ureteral stones) cases retrograde or antegrade, Double-J stents were sited. A 16F urethral catheter was inserted on free drainage.
Operative parameters were recorded including procedure time and patient radiation exposure.
Standard postoperative care was carried out in a dedicated urology ward, including removal of catheter on day 1 and removal of nephrostomy on day 1 or day 2 depending on clinical progress.
Complications were graded using a modified Clavien–Dindo Classification (CDC). 12 In addition, pre- and postoperative hemoglobin values were recorded as well as blood transfusion rates.
Coprimary outcome measures of SFR, procedure success, and operative time were recorded. All patients deemed clear at the time of surgery were evaluated using noncontrast CT imaging at 3 months postoperatively to assess stone clearance, as per standard local practice. Procedure success was considered to be achieved for residual fragments <2 mm or stone-free patients. In the case of significant residual stone detected intraoperatively, subsequent procedures were booked without updated cross-sectional imaging.
Statistical analysis was performed using Prism® (GraphPad Software, Inc., San Diego, CA) software. Descriptive statistics are reported using mean ± SD for continuous variables and proportion/percentage for categorical variables. Comparative statistics were analyzed using chi-square test for categorical variables and analysis of variance for continuous variables.
Results
Demographics
A total of 303 patients underwent PCNL: 185 (61.1%) males and 118 (38.9%) females with a mean age of 53.43 ± 16.31 years and mean body mass index (BMI) of 28.98 ± 6.59kg/m2. Forty-six (15.1%) patients had previous treatment with PCNL, 60 (19.8%) with endoscopic methods (stent/ureteroscopy), and 5 (1.7%) with shockwave lithotripsy.
Eighty-three (27.4%) patients had CCI score of 0, 81 (26.7%) had a score of 1 to 2, 80 (26.4%) had a score of 3 to 4, and 56 (18.5%) had a score of ≥5. Three (1%) patients had no CCI score recorded.
Access
Ultrasound alone was used for access imaging in 77 (25.4%) cases, fluoroscopy alone in 2 (0.7%) cases, and a combination in 224 (73.9%) cases.
Twelve (4%) patients required a second tract to be created, all because of stones in multiple calices or staghorn stones. Primary lower pole access was used most frequently (58.4%) with the interpolar calix accessed in 26.7% of cases. Upper pole access was performed in 14.8% of cases.
Simultaneous ECIRS was carried out in 45 (14.9%) cases with a flexible ureterorenoscope in 39 (12.9%) and a rigid scope in 6 (2%) cases.
Outcomes
A total of 210/303 (69.3%) patients had no residual stone on CT, whereas 34/303 (11.2%) had <2 mm stone fragments. A total of 244/303 (80.5%) patients were deemed to have an effective procedure by the mentioned criteria. Mean operative time was 79.79 ± 35.72 minutes. Mean fluoroscopy time and radiation dose were 533.8 ± 374.5 seconds and 108.79 ± 101.47 mGy, respectively. Patients had a mean hospital stay of 4 ± 3 days.
Minor complications (CDC 1–2) occurred in 59 (19.5%) cases and major complications (CDC ≥3) occurred in 22 (7.3%) cases. Failed access occurred in 9 (3%) cases. Mean decrease in hemoglobin was 1.71 ± 1.66 g/dL. Five (1.7%) cases required postoperative blood transfusion for bleeding complications.
Stone factors
The left kidney was treated in 159 (52.5%) cases and the right in 144 (47.5%) cases. Mean stone size excluding staghorn stones was 17.26 ± 5.96 mm. Mean stone density was 1081.04 ± 413.77 HU.
The impact of stone position is given in Table 1. Staghorn stones had the lowest procedure success rate and longest operative time. No significant difference was seen in hospital stay, complication rate, or hemoglobin drop (p = 0.516). Solitary stones situated in the upper pole had a significantly lower clearance rate (p = 0.011) and higher rate of failure to access (17.4%) than stones in any other position.
CDC = Clavien–Dindo Classification.
The impact of stone size on outcomes is displayed in Table 2. Stones >25 mm and staghorn stones had significantly longer operative time and lower procedure success (p < 0.0001). Considering stones between 1 and 2 cm, a procedure success of 91.3% was achieved with a major complication rate of 4.7% (overall complication rate of 25.2%). Mean operative time was 71.4 ± 31.3 minutes.
Procedure success for GSS1 was 158/169 (93.5%), GSS2 was 49/63 (79%), GSS3 was 8/18 (44.4%), and GSS4 was 25/50 (50%).
Patient factors
Impact of BMI on operative parameters is given in Table 3. Increase in BMI did not significantly reduce procedure success, increase hospital stay, or major complication rate. Radiation exposure and fluoroscopy time were not significantly different between weight categories. Overall complication rate and failure to access were not significantly affected by obesity.
BMI = body mass index.
Discussion
The Galdalko-modified Valdivia position for supine PCNL offers many well-described advantages over prone position. The 2010 audit data from the British Association of Urological Surgeons showed only 6% of procedures were undertaken in the supine position. 13 This increased to 20% in the most recent published data (2015) in keeping with the Clinical Research Office of the Endourological Society study in 2011, which also quoted a 20% rate worldwide. 14 This suggests a growing acceptance of the supine position among stone surgeons.
We describe a large single-center experience of supine PCNL. Our study is limited by the lack of comparative arm; however, all PCNLs in our center are carried out in the Galdalko-modified Valdivia position, which in itself reflects the versatility of this approach.
The authors also recognize the limitation of maximal stone diameter as a measure of stone burden; however, at inception of the study, this was the most reliable method using available local technology. We note the relatively small mean stone size for a PCNL series (17.26 mm). However, it is important to identify that this probably underestimates the true stone burden treated as it excludes measurements of all staghorn and partial staghorns, as well as providing a single measurement for patients with multiple stones. Measurement of stone volume may better reflect the stone burden treated in these patients. The GSS was used to classify complexity, requiring simple clinical and radiological data to categorize patients in a reproducible manner. However, as with other scoring systems, this is limited by user variability in classifying partial and complete staghorn stones, as well as anatomical complexity.
In addition, we note our relative long fluoroscopy time (533.8 seconds) particularly given that ultrasound-guided puncture was employed in most cases. The authors did not collect a detailed inventory of radiation exposure or use for specific portions of the procedure, efforts should be made to limit exposure to radiation for patients and staff.
Although anesthetic complications are rare in PCNLs, prone position can present a challenge, particularly in obese or unfit patients. Cardiac output is decreased by up to 24%, emergency airway access is compromised, and both direct and indirect pressure injuries can occur during prolonged surgery. 15 In addition, Zhang et al. 6 showed a significantly shorter operative time for supine PCNL, time savings are made by not having to reposition the patient intraoperatively. Reducing manual handling of obese patients limits the potential for staff “lifting” injuries. Given that 29.4% of patients in our series were obese or morbidly obese and 44.9% had a CCI ≥3, anesthetic considerations must be taken into account when deciding on patient position for PCNL, with supine position offering clear advantages. The rising rates of obesity worldwide coupled with the links between obesity, metabolic syndrome and stone disease mean that future considerations must be given to the high-risk population. 16
The primary outcome measure was stone clearance rate, with a criteria of <2 mm fragment on low-dose CT imaging defined as effective clearance. Previous authors have used <4 mm, <2 mm, and complete clearance to define procedure success. Raman and colleagues demonstrated on multivariate analysis that residual fragments >2 mm predicted future stone events. 17 In addition, a variety of imaging modalities have been used throughout the literature with varying sensitivity. Standard practice in our unit for all stone follow-ups is with low-dose noncontrast CT, which is easily accessible and provides detailed clinical information with an acceptable radiation dose.
In 80.5% of patients, we achieved complete clearance or <2 mm fragments, rising to 87.4% when staghorn stones were excluded. Although comparison with other studies has limitations, these rates are broadly similar to those of large series of prone PCNL and rates in meta-analysis of comparative studies. 3,4,6 Conflicting data exist regarding the SFR in supine position, but in the experience of the authors, supine position does not have significant limitations on scope mobility or caliceal access, particularly with the additional benefit of retrograde access and flexible instruments during the procedure. 18 A total of 14.9% of our patients had simultaneous ECIRS to achieve stone clearance that would otherwise have been impossible without a second tract. ECIRS can be performed in the prone split leg position; however, the supine position provides a familiar operating environment and anatomical orientation for the surgeon.
Our coprimary measure of operative time is often cited as one of the major advantages to supine position, with Liu et al. reporting a 24.8-minute reduction in operative time compared with prone PCNL. 4 As expected, we demonstrate increasing stone size as the most significant factor in increasing operative time. The major time savings with supine Galdalko-modified Valdivia position are because of the lack of intraoperative repositioning, rescrubbing, and redraping. Some time savings may also be because of simultaneous retrograde access, allowing easy manipulation of difficult-to-reach stones.
In contrast to the 2012 CROES analysis on obese patients by Fuller and colleagues, 19 our study does not demonstrate increasing BMI to negatively influence operative time, SFR, or complication rates. The authors suggest that given the anesthetic benefits and lack of need for repositioning, supine position should be considered the preferred option for all obese patients undergoing PCNLs.
In our series, failed percutaneous renal access was documented in 9 out of 303 (3%) cases. However, these were all in the first 100 cases of the series during our learning curve with this approach. Failed access was not as a result of the patient's intraoperative position, but as a result of renal anatomy (two caliceal diverticulum stones, four upper pole stones, two parenchymal stones, and one large complex staghorn calculus). The patients with stones in caliceal diverticulum, upper pole, and staghorn cases were subsequently treated after percutaneous renal access the day before PCNL by the interventional radiologist in the interventional radiology suite. The authors would recommend delayed urogram phase CT for all cases when the anatomical location of the stones cannot be verified on noncontrast CT scan, with consideration of preoperative tract formation.
Upper pole stones present a unique challenge because of limitations on anatomical access directly into the upper pole. Twenty-three solitary upper pole stones were treated, with an overall success rate of 65%. Seventeen (73.9%) had direct upper pole access; however, four (23.5%) of these had failed access procedures. In all, 45 (14.9%) had upper pole access, 2 (4.4%) had major complications (1 pseudoaneurysm, 1 migrated ureteral stent), but no injuries to lung or adjacent organs were encountered. No significant difference in complication rates compared with other locations (p = 0.435) was seen.
However, significantly lower procedure success and higher failed access rates were seen with upper pole access. This limitation to upper pole access is common to both supine and prone positions. 20 The advantage over prone position is seen in 45 (14.9%) of patients who had simultaneous ECIRS to achieve clearance that would otherwise have been impossible without a second tract. Sixteen of these patients had stones in the upper pole or multiple calices including the upper pole.
Visceral injury is a rare but serious complication of PCNL occurring in 0.2% to 0.3% of prone procedures. 21 Hopper et al. showed the presence of a retrorenal colon on CT imaging in only 1.9% of supine PCNL patients, but 10% of prone patients. 22 No visceral injuries were encountered in our study. Overall, complications arose in 81 (26.7%) cases, with the majority minor (CDC 1–2). Infection was the most common complication occurring in 6% of patients. Previous authors have suggested that theoretically lower infective rates in the supine position may be possible than in the prone position because of lateral position of the Amplatz sheath, resulting in better irrigant outflow and lower intrarenal pressure, reducing pyelovenous reflux 9 ; however, this has not been translated into practice.
We have demonstrated that PCNLs in a high-volume center to be safe and efficacious in the Galdalko-modified Valdivia position. We show equivalent SFR and complication rates to large studies of prone PCNL, with potential to decrease operative time. In particular, supine position is optimum for obese patients with complex stone disease, because of ease of positioning and lower risk of anesthetic complications. The supine position PCNL continues to gather support as the procedure of choice for complex renal stones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.