
Abstract
Purpose:
The present study was designed to investigate the risk factors affecting the conversion to open surgery in retroperitoneal laparoscopic nephrectomy of nonfunctioning renal tuberculosis (TB).
Patients and Methods:
The records of 144 patients who underwent a retroperitoneal laparoscopic nephrectomy procedure by a single surgeon were retrospectively reviewed. The following factors, including age, sex, body mass index (BMI), diabetes status, hypertension status, side of kidney, size of kidney, degree of calcification, mild perirenal extravasation, contralateral hydronephrosis, the time of anti-TB, and surgeon experience were analyzed. Univariate and multivariate logistic regression analyses were used for statistical assessment.
Results:
Twenty-three patients were converted to open surgery and the conversion rate was 15.97%. In univariate analysis, BMI ≥35 kg/m2 (p = 0.023), hypertension (p = 0.011), diabetes (p = 0.003), and kidney size (p = 0.032) were the main factors of conversion to open surgery. Sex, age, side, anti-TB time, calcification, mild extravasation, and surgeon experience were not significantly related. In multivariate regression analysis, BMI ≥35 kg/m2, hypertension, diabetes, and enlargement of kidney were the most important factors for conversion to open surgery.
Conclusions:
Depending on the results achieved by a single surgeon, BMI ≥30 kg/m2, diabetes, hypertension, and enlargement of kidney significantly increased the conversion risk in retroperitoneal laparoscopic nephrectomy for nonfunctioning renal TB.
Introduction
T
Urinary TB (UTB) is one of the most common types of extrapulmonary TB, it occurred by hematologic dissemination of pulmonary TB in almost all cases and most of UTB cases occurred in developing nations. 3,4 The symptoms of UTB are nonspecific, and voiding problems and chronic urgency nonresponding to antibacterial drug regimens are indicative of UTB. Commonly, the symptoms were intermittent and had been present for some time before the patient sought medical advice, and the disease might be in its advanced stage. 5 In addition, drug resistance is another impediment to TB management. 6 As a result, many patients advanced to have a nonfunctioning kidney with or without calcification which need a nephrectomy to deal with. 7,8
With the development of laparoscopic techniques, most patients with nonfunctioning renal TB could get safe and effective treatment through retroperitoneal laparoscopic nephrectomy. The procedure has the characters of minimal invasiveness, less blood loss, and quick recovery. 9,10 However, there was still a small part of patients who required the conversion to open surgery due to severe bleeding and adhesion. 11 It was particularly important to assess the risks of the conversion to open surgery before the operation, to better inform the patient, and prepare accordingly. Herein, we report the results of 144 patients with nonfunctioning renal TB who were treated by retroperitoneal laparoscopic nephrectomy by a single surgeon in the First Hospital of Jilin University. This article may be the only report on this subject.
Patients and Methods
The electronic patient database of the First Hospital of Jilin University was queried for patients with retroperitoneal laparoscopic nephrectomy of nonfunctioning renal TB by a single surgeon in the First Hospital of Jilin University. The surgeon had performed more than 1000 cases of nephrectomy for malignant tumors and benign renal disease. From May 2007 to May 2014, 144 consecutive patients with nonfunctioning renal TB were enrolled in the study.
All patients were preoperatively diagnosed with unilateral renal TB, based on clinical symptoms, radiological investigations, and selected laboratory examinations. Preoperative radiological investigation consisted of urinary ultrasonography, excretory urography, CT, and nuclear scintigraphy (Fig. 1). Renal function was evaluated by Excretory urography and nuclear scintigraphy. The laboratory survey included urine analysis, real-time polymerase chain reaction to detect mycobacterial DNA, and urine culture. Preoperative patients received at least 2 weeks anti-TB treatment.
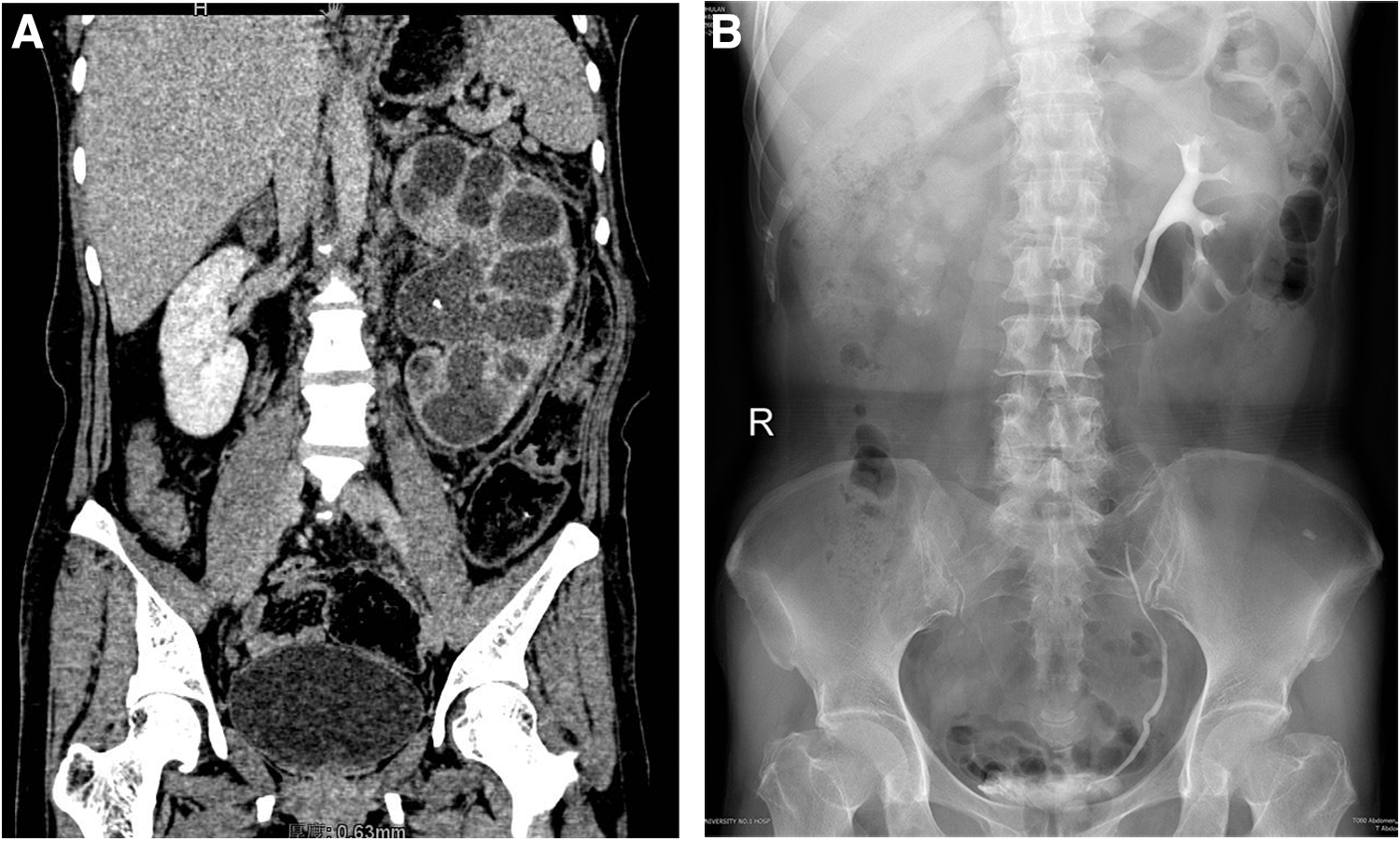
Representative imaging of renal TB.
Preoperative factors that were analyzed were patient age, sex, the presence of hypertension, diabetes mellitus, body mass index (BMI), side, kidney volume, calcification, contralateral hydronephrosis status, and anti-TB. Age was stratified into <60 group and ≥60 group (Chinese standard of definition of old people). According to WHO 2004 classification published in BMI, it was divided into three groups (<25 kg/m2, 25–35 kg/m2, ≥35 kg/m2). Kidney volume was defined according to the length of the kidney by CT scan (<10, 10–12, >12 cm). The preoperative time of anti-TB was divided into three groups (<1, 1–3, >3 months). Surgeon experience defined as <50 cases, 50 to 100 cases, and >100 cases. Preoperative blood pressure and glucose in all patients are controlled within the normal range or meet the surgical requirements, and the intraoperative blood pressures in all cases were controlled below 140/90 mm Hg by the anesthesiologists.
Statistical methods
SPSS software, (version 17.0; SPSS, Institute, Chicago, IL) was used for all statistical analyses. Chi-square and Fisher exact tests were used for univariate analysis to determine the main risk factors of laparoscopic surgery conversion to open surgery. Multivariate binary logistic regression was performed for further investigation if any parameter was found to be significant with univariate test. In all analyses, two-sided hypothesis testing was carried out, and probability values less than 0.05 were deemed significant.
Results
Mean age was 47.9 years ±11.9 years (range 16–76 years), and mean BMI was 26.5 ± 2.6 kg/m2 (range 21.8–33.0 kg/m2). Diabetes status and hypertension status were present in 21 (14.6%) and 38 (26.4%) patients, respectively. The average of the kidney size was 11.4 ± 3.2 (range 7.8–14.3 cm). Fifty-two (36.1%) patients had a calcification and 8(5.6%) patients had a mild extravasation according to the CT scan. Fifty-seven (39.6%) patients received an anti-TB treatment for more than a month. The mean operative time was 124.2 ± 44.3 minutes (range 60–275 minutes).
Twenty-three cases were converted to open surgery due to severe adhesions and bleeding, whereas the other patients were treated successfully. The conversion rate was 19.01%. In univariate analysis, BMI ≥35 kg/m2 (p = 0.023), hypertension (p = 0.011), diabetes(p = 0.003), and kidney size(p = 0.032) were the main factors of conversion to open surgery. However, sex, age, side, anti-TB time, calcification, mild extravasation, and surgeon experience were not significantly related (Table 1). In multivariate regression analysis, BMI ≥35 kg/m2, hypertension, diabetes, and enlargement of kidney were the most important factors for conversion to open surgery (Table 2).
Data show results from patients with nonfunctioning renal tuberculosis (n = 144). p Values ≤0.05 were considered significant.
BMI = body mass index.
Data show results from significant factors in univariate analysis are analyzed by multivariate regression analysis.
p Values ≤0.05 were considered significant. OR values >1 were risk factors.
CI = confidence interval.
Discussion
Advanced stage renal TB is characterized by the appearance of severe hydronephrosis and calcification. When a tuberculous lesion has advanced to the collecting tubules or the renal pelvis, it never heals completely because of a hindered drainage and backpressure effects. Nephrectomy is strongly indicated in patients with a nonfunctioning tuberculous kidney with calcification or extensive disease involving the whole kidney with other complications, including hypertension or coexisting renal cell carcinoma. 12
Because of severe adhesions of nonfunctioning renal kidney and surrounding tissue, and disturbance of normal anatomy structure, laparoscopic surgery was once considered to be a relative contraindication for inflammatory kidneys. 13,14 With the development of laparoscopic instruments and techniques, Kim and Hemal and colleagues confirmed the equal therapeutic effect of laparoscopic surgery and open surgery for nonfunctioning kidney TB treatment. 10,15 Simultaneously, because of small trauma, faster recovery, less blood loss, and less additional damage, open surgery was replaced gradually. 9,16 But there were still some patients turning to open surgery during operation due to severe adhesions of kidney and surrounding tissue or bleeding. Manohar's studies indicated that the conversion rate of laparoscopy had reached 10% to 25%. 11 Therefore, we should evaluate the risk of conversion to open surgery sufficiently before operation, confirm good communication with patients, and appropriate preventive measures. This study used univariate and multivariate logistic regression analyses to determine the main risk factors of conversion to open surgery. Due to the advantage of avoiding contamination to the abdominal organs, all of these cases were performed by retroperitoneal approach.
Thus, patients' physical condition played an important role in determining if it was necessary to turn to open surgery. Gong and colleagues divided 239 patients, who had received laparoscopic surgery, into several groups according to BMI, and indicated that the degree of obesity would increase the difficulty of laparoscopic surgery. 17 However, whether obesity was a risk factor of conversion to open surgery still remains a controversy. 18,19 In our study, obesity was a key factor associated with the conversion. The possible reasons might be that the rich retroperitoneal adipose tissue of obese patients led to a smaller operation space and insufficient exposure of anatomical landmarks.
Hypertension and diabetes status also influenced the conversion rate in this study. Some research explained the relationship between hypertension and intraoperative and postoperative bleeding in many kinds of surgery with arteriosclerosis. 20 Diabetes affects the whole vascular system, resulting in microangiopathies and arteriosclerosis, which are highly vulnerable to bleeding. The impact of diabetes and hypertension on lipid metabolism could lead to peripheral vascular sclerosis and fibrosis of perirenal tissues, which increase the difficulty of intraoperative separation between kidney and perirenal tissues. 21 However, only two patients with diabetes and three patients with hypertension were not well controlled in our cohort, and we could not stratify these two groups into subcategories of severity. We are not sure whether uncontrolled hypertension and diabetes will be significant contributing factors. This may limit the generalizability of our results.
As for relevant factors of kidney itself, enlargement of kidney became a main risk factor. Compared with 94 cases of open surgery, Manohar who made retrospective analysis of 84 cases of laparoscopic surgery for benign and inflammatory kidney diseases, found that the kidney diameter >10 cm displayed significant correlation with conversion to open surgery. 11 Related report also indicated that the enlargement of kidney would increase the difficulty of laparoscopic nephrectomy for renal cell carcinoma. 22 However, Fan and colleagues' meta-analysis indicated that kidney size had no significant correlation with conversion to open surgery. 23 There is no report about the procedures for a TB kidney in literature. In our study, we considered that enlargement of kidney was a main risk factor. Tissue adhesions of perirenal fat and the changes in anatomy might cause the difficulty of separating the renal pedicle vessels, and increase vascular injury during the separation.
Extravasation is a common phenomenon in TB patients, which indicate that severe adhesion may exist around perirenal tissues. 9 Preoperative CT examination was very important to evaluate the extravasation in renal TB patients, and it could provide a clear outline of the entire urinary system. 11 In our study, the preoperative CT showed 18 cases of patients with a mild perirenal extravasation, and 5 cases converted to open surgery. However, the univariate analysis showed that the conversion rate had no significant difference compared with the normal patients. The small sample size of patients with mild extravasation may be one of the reasons. In addition, for patients with a moderate or severe extravasation according to preoperative imaging examinations, open surgery may be chosen directly.
Clinical experience, perhaps, has an influence on the conversion rate. In our study, to avoid differences in surgical technique, we enrolled the patients whose surgeries were performed by a single well-experienced surgeon. The patients were divided into three groups, and the results showed no difference in the risk of conversion to open as observed between groups. Therefore, the surgeon's experience was not the major risk factor for conversion to open. This might be based on the skilled experience of laparoscopic nephrectomy for other kidney diseases. But for young physicians with less laparoscopic surgery experience, it was recommended to strengthen their professional skills, and then to carry out such operations.
Conclusions
Depending on the results achieved by a single surgeon, BMI ≥30 kg/m2, diabetes, hypertension, and enlargement of kidney significantly increased the conversion risk in retroperitoneal laparoscopic nephrectomy for nonfunctioning renal TB. For patients who have the risk factors, we could inform the patient the situation preoperatively, and prepare accordingly.
Footnotes
Author Disclosure Statement
No competing financial interests exist.