
Abstract
Objectives:
Evaluation of the feasibility, morbidity, learning curve, and functional results of robotic supratrigonal cystectomy with augmentation ileocystoplasty (RSCAI).
Materials and Methods:
RSCAI was performed in 19 patients between 2012 and 2016. Thirteen patients (66.4%) presented refractory detrusor overactivity or impaired compliance and 6 patients (31.6%) had painful bladder syndrome. A combined robot-assisted laparoscopy and mini-laparotomy approach was performed. Early (<30 days) and late (>30 days) complications were reported according to the Clavien-Dindo classification. Functional results were analyzed according to the surgical indication.
Results:
Mean total operating time was 288.7 ± 92.1 minutes. Mean intraoperative blood loss was 147.4 ± 144.8 mL. Mean length of hospital stay in the surgical ward was 9.4 ± 3.7 days. Mean duration of bladder drainage was 23.3 ± 4.1 days. For surgeons who regularly performed robot-assisted laparoscopy, the learning curve of this technique, as assessed by the operating time, required almost five operations. No major (Clavien-Dindo >2) early (0%) or late (0%) postoperative complication was observed. Early minor complications were observed in 47.4% of cases, usually consisting of pyelonephritis (21.1%). Late minor complications (10.5%) were Clavien-Dindo grade I. Mean follow-up was 13.6 ± 10.1 months. The majority of patients (94.7%) obtained functional improvement of their disease in terms of pain, functional bladder capacity, or bladder compliance.
Conclusion:
Our RSCAI technique is a reliable technique with no early or late major postoperative complications reported in this series. This technique allows patients to be operated by minimally invasive surgery with very satisfactory long-term functional results.
Introduction
S
Robot-assisted surgery overcomes the limitations of laparoscopy (three-dimensional vision, articulation, and precision of instruments), while preserving the advantages of minimally invasive surgery (shorter hospital stay and decreased postoperative pain and surgical scars). 2 The European Association of Urology has published guidelines concerning the use of robotic surgery in urology, 3 but they only recommend robot-assisted radical cystectomy for cancer, which is associated with decreased intraoperative blood loss and morbidity and a shorter convalescence period.
The first case of robotic supratrigonal cystectomy with augmentation ileocystoplasty (RSCAI) was reported by Al-Othman and colleagues 4 in 2008, and 47 cases have subsequently been reported in the literature. 5 –10
The primary objective of this study was to evaluate the morbidity of RSCAI. The secondary objectives were to evaluate the learning curve and functional results of this technique.
Patients and Methods
Population
We conducted a retrospective review of the medical records of 28 patients operated in our center by supratrigonal cystectomy with augmentation ileocystoplasty between October 2012 and April 2016.
Nine patients operated by laparotomy were excluded from this review: seven patients in whom a continent cystostomy procedure was performed at the same time (Mitrofanoff, or Yang-Monti) and two patients presenting a contraindication to pneumoperitoneum due to the presence of syringomyelia.
This review was therefore finally based on the medical records of 19 patients operated by RSCAI.
The indication for RSCAI was as follows: DO refractory to intradetrusor botulinum toxin injections and/or sacral root neuromodulation in six cases (31.6%); low compliance <30 mL/cmH2O in seven cases (36.8%); and treatment-refractory painful bladder syndrome in six cases (31.6%).
The population had a mean age of 49.0 ± 15.6 years with a sex ratio of 9 men to 10 women. An associated neurological disease was present in eight patients (42.1%) (Table 1). Twelve patients (63.2%) performed intermittent self-catheterization before the operation.
ASA = American Society of Anesthesiologists; BMI = body mass index; HT = hypertension.
Operative technique
The operation was performed under general anesthesia. The patient was placed in the Trendelenburg position with nasogastric tube placement at the beginning of the operation. Midline infraumbilical open laparoscopy was performed with placement of a 12 mm optical trocar. Pneumoperitoneum was created by intra-abdominal insufflation to a pressure of 12 mm Hg. The three 8 mm robotic trocars and the two 5 and 12 mm assistant trocars were then placed (Fig. 1). The Da Vinci S 4 arm robot (Intuitive Surgical, Sunnyvale, CA) was connected.
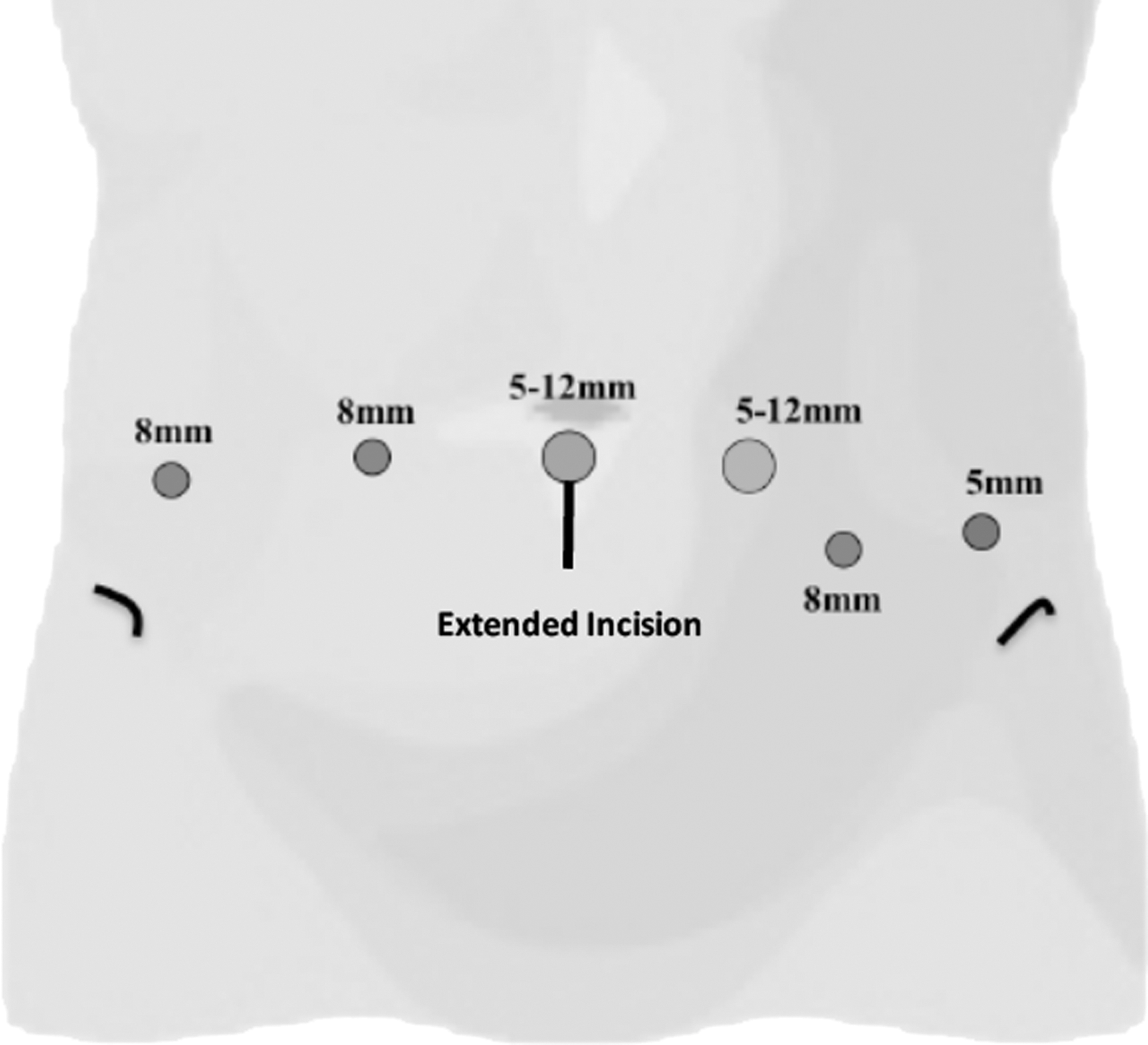
Position of the trocars.
Robot-assisted supratrigonal cystectomy started with a longitudinal peritoneal incision of the bladder dome with preservation of the peritoneum. Lateral, anterior, and posterior surfaces of the bladder dome were released as far as the bladder neck. The bladder was then opened at the dome in the sagittal plane to reveal the trigone and ureters. Ureteral stenting was performed by the robot using 5F ureteral stents as landmarks. Supratrigonal cystectomy was performed by circular excision of the bladder dome, passing 1 to 2 cm above the trigone using an Ultracision® scalpel allowing hemostasis and section of the bladder wall and pedicles. The cystectomy specimen was placed in an extraction bag.
The robot was disconnected and the cystectomy specimen was extracted by the umbilical incision that was enlarged to a maximum of 5 cm below the umbilicus. An Alexis wound protector/retractor (Applied Medical, Rancho Santa Margarita, CA) was inserted. A 40 cm ileal loop was harvested by this mini-laparotomy with restoration of intestinal continuity by end-to-end anastomosis using resorbable braided suture material (Vicryl 3/0). The ileal loop was detubularized and a Z-plasty or U-plasty was then performed (at the surgeon's discretion) with resorbable braided suture material (Vicryl 3/0). Two resorbable V-lock 3/0 sutures tied together were then inserted around the most posterior part of the ileal graft.
The graft was reintroduced into the abdominal cavity. The reduced port was positioned on the Alexis wound protector/retractor with placement of the 12 mm optical trocar. After insufflation, the four-arm robot was again connected. The ileal graft was anastomosed to the trigone by robot-assisted surgery by means of two V-lock 3/0 simple running sutures starting at 6 o'clock on the posterior surface and then ascending to 12 o'clock on the anterior surface. Ureteral stents were left in place during suture of the posterior plane to clearly identify the ureters and the stents were then removed before completing the ileovesical anastomosis. During the first cases, when the incision was too close to the ureteral orifice, we preferred to leave ureteral stents for the cicatrization. A urethral catheter was inserted and a leak test was performed. The catheter was left in place for at least 3 weeks.
Reperitonealization was performed with V-lock 3/0 by suturing the free edge of the peritoneum of the bladder dome to the lateral border of the ileoplasty on either side of the mesentery. Nonsuction drainage (20F Portex® drain) was placed anterior to the ileoplasty underneath the peritoneum.
The robot was disconnected and the various incisions were closed by fascial suture for incisions longer than 10 mm and skin suture.
Complications
Complications were reported according to the Clavien-Dindo classification 11 and were classified into two categories: minor (grades I and II) and major (grades III, IV and V). Complications were considered to be early when they occurred during the first 30 postoperative days and late when they occurred after 30 days.
Return of bowel function was defined by the first bowel movement. Postoperative ileus was considered pathological when the first bowel movement appears after >72 hours.
Functional results were analyzed at the last follow-up visit, at least 3 months after surgery. Postoperative evaluation was based on a pain visual analogue scale (VAS) and voiding frequency/24 hours for patients with painful bladder syndrome, functional bladder capacity and urodynamic studies for patients with DO, and postoperative urodynamic studies for patients with impaired compliance.
Results
Perioperative data
Perioperative characteristics are represented in Table 2.
All 19 operations (100%) were able to be performed by robot-assisted laparoscopy with no conversions to either open surgery or laparoscopy.
In four cases (21.1%), the ileovesical anastomosis was performed close to the ureteral orifices, essentially during the first cases of the series, requiring postoperative maintenance of ureteral stents or double J stents.
Mean intraoperative blood loss was 147.4 ± 144.8 mL, and was <100 mL in 10 patients (52.6%) and >300 mL in 2 patients (10.5%).
The mean time to return of bowel function, defined by the first bowel movement, was 3 days. Weaning from narcotic analgesics was performed on average after 2.6 ± 1.8 postoperative days and two patients did not require morphine.
The mean length of hospital stay was 9.4 ± 3.7 days, while two (10.5%) spinal cord injury patients were admitted to the surgical intensive care unit for 24 hours. Seven patients (36.8%) with a neurological disease required admission to a rehabilitation center for a mean duration of 32.0 ± 3.7 days.
Learning curve
Before starting to perform this type of operation, the two operators had an experience of >200 robotic surgery procedures for surgeon 1 and 40 robotic surgery procedures for surgeon 2. Operating times as a function of the learning curve are represented in Figure 2. Surgeon 2 was assisted by surgeon 1 for the first two operations.
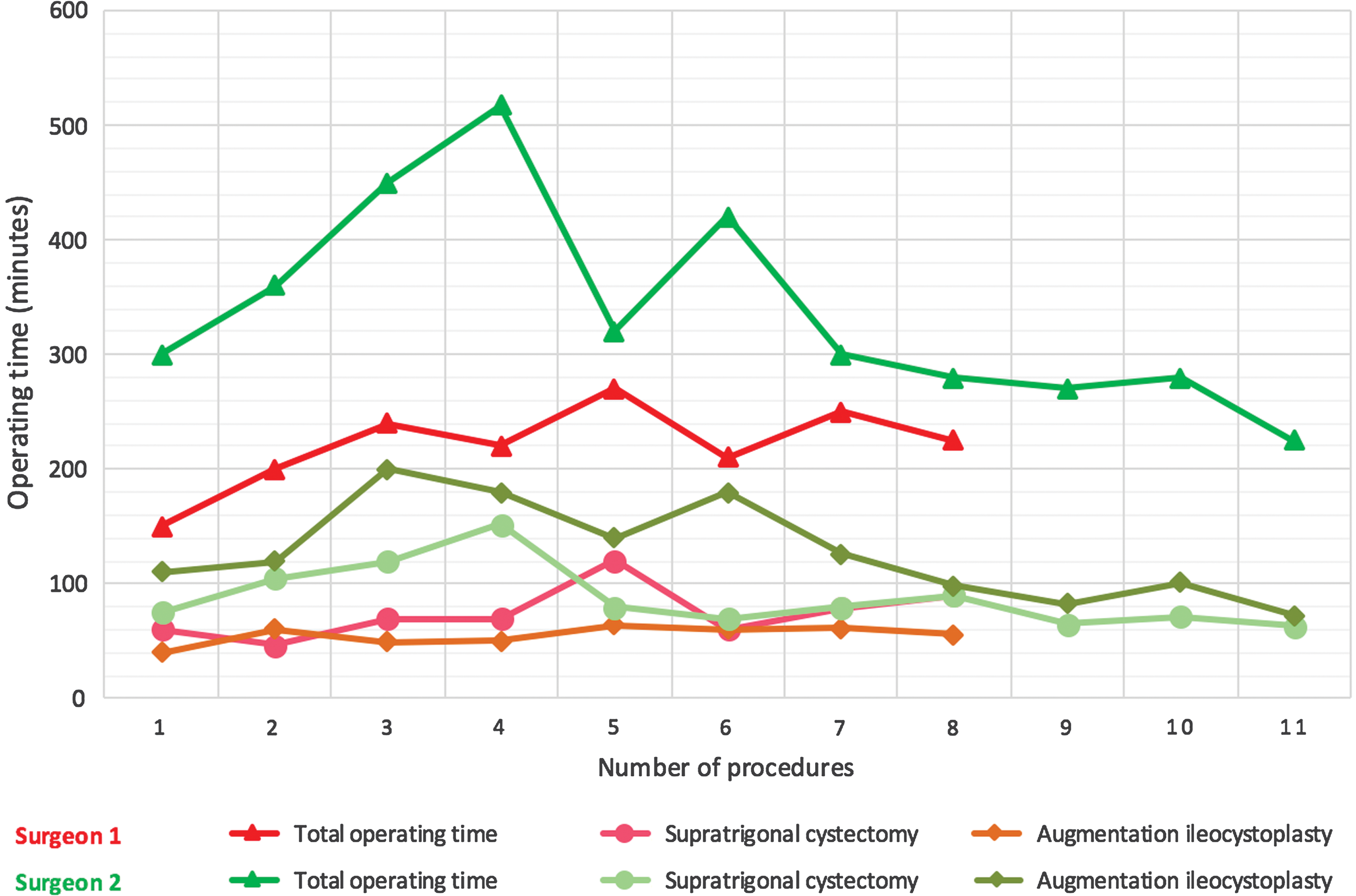
Operating time learning curve.
Early morbidity
No early major complication was observed. Nine patients (47.4%) experienced a minor complication, three (15.7%) classified as Clavien grade I and six (31.6%) classified as Clavien grade II (Table 3). The most severe complication was pelvic hematoma with reflex ileus requiring transfusion of 3 U of packed cells. The most common complication was pyelonephritis, observed in four cases (21.1%).
Late morbidity
No late major complication was observed. Two (10.5%) Clavien grade I minor complications were reported (Table 3). One patient developed urinary retention due to difficulties of self-catheterization related to a mucus plug and the other patient developed pyelonephritis.
Functional results
Mean follow-up was 13.6 ± 10.1 months. None (0%) of the seven patients (36.8%) voiding spontaneously before the operation required postoperative intermittent self-catheterization.
In six patients with painful bladder syndrome, the preoperative mean VAS was 8.7 ± 1.2 and the preoperative mean voiding frequency was 37.6 ± 11.6 voids/24 hours. Postoperatively, VAS and voiding frequency were improved in all patients, with a mean VAS of 0.3 ± 0.5 and a mean voiding frequency of 9.6 ± 3.8 voids/24 hours.
In seven patients with impaired bladder compliance, preoperative mean bladder compliance was 13.1 ± 8.3 mL/cmH2O. Six months after the operation, compliance was improved in all patients with mean bladder compliance of 39.4 ± 12.0 mL/cmH2O.
In six patients with refractory DO, preoperative mean functional bladder capacity was 188.3 ± 37.6 mL. After surgery, five patients no longer presented any sign of DO on postoperative urodynamic studies with improvement of their functional bladder capacity to 380.8 ± 171.7 mL. One patient presented autonomic hyperactivity of the ileoplasty for a filling volume of 200 mL associated with bladder pain and urinary incontinence, and required reoperation for removal of the ileoplasty and trigone and Bricker ileal conduit urinary diversion.
Discussion
Although retrospective, this study represents the largest published series of RSCAI. It was also based on a homogeneous patient series, in which we deliberately excluded patients requiring an associated continent cystostomy, which can make the procedure more complicated. Our technique differs from that reported in the most recently published series by the use of a mini-laparotomy for extraction of the cystectomy specimen and creation of the ileocystoplasty. Finally, we report the functional results with a postoperative follow-up of >1 year.
This technique was associated with low early and late complication rates and no major complication was observed. The learning curve in terms of operating time was rapid with reasonable operating times after five procedures, even for a surgeon less experienced in robotic surgery. Finally, long-term functional results were excellent, regardless of the operative indication: painful bladder syndrome, refractory DO, or impaired bladder compliance.
A combined approach comprising robotic assistance and mini-laparotomy was used in this series, allowing the intestinal anastomosis to be performed without contamination of the abdominal cavity with digestive fluid, which limits the risk of postoperative abscess and fistula. 5,12 This technique also allowed a shorter operating time, which could limit the risks of thromboembolism and nerve compression, and facilitates postoperative recovery. The mean operating time in this series was 288 ± 92 minutes, which is close to that reported during open surgery, ranging from 230 to 337 minutes. 13 Conversely, the mean operating time in series of completely intracorporeal robot-assisted laparoscopy in patient with neurogenic bladder ranged from 365 to 623 minutes. 9,10 However, in these series, they performed an enterocystoplasty, but not always a supratrigonal cystectomy, and in most cases, a catheterizable channel associated, which can explain the difference in operating time.
Arguments of operating time and contamination of the abdominal cavity by opening the gastrointestinal tract were, for us, the justification for performing extracorporeal ileocystoplasty to limit the risk of postoperative complications, as no major complication (Clavien grade ≥II: thromboembolic complications or peritoneal abscesses) was observed in this series. During supratrigonal cystectomy, an abdominal incision must be performed to extract the cystectomy specimen and this incision is the same size as that used for ileocystoplasty. However, this technique requires disconnection and reconnection of the robot during the operation, but without increasing the operating time.
No case of robot-assisted laparoscopic supratrigonal cystectomy with augmentation ileocystoplasty associated with continent cystostomy was performed in this series, as this procedure would significantly prolong the operating time. 9 Furthermore, due to distention of the abdominal cavity by pneumoperitoneum, useless tractions could be applied to the appendix (Mitrofanoff procedure) or Monti's procedure that could potentially damage anastomosis with the bladder or the mesentery. 9
For surgical teams regularly performing robot-assisted surgery, this technique appears to be associated with a short learning curve to achieve similar operating times to those of open surgery. For surgeon 1, specialized in robot-assisted laparoscopic surgery, the operating time was close to that of open surgery by the first operation, while surgeon 2 had to perform five operations to achieve a similar operating time. The ileovesical anastomosis appears to be the most difficult part of the procedure at the beginning of the learning curve.
The early minor postoperative complication rate was 47.4%, similar to that reported in the literature. 9,10 Early complications essentially consisted of four cases of pyelonephritis and two cases of ileus, similar to the reported complication rates for this operation. 8 Similar low levels of blood loss have also been reported in recent series. 9,10 In contrast, we did not observe any early or late major complication in this series. However, Murthy and colleagues reported two Clavien grade III complications 10 and Flum et al. reported three Clavien grade IIIB complications (late bladder perforation, ruptured ileovesicostomy anastomosis, and bowel obstruction due to adhesions) and one Clavien grade IVA complication (severe sepsis). 9
Finally, analysis of the functional results showed 100% good results in terms of pain scores and voiding frequency in the group of patients with painful bladder syndrome. However, it should be stressed that these patients were strictly selected, as they initially presented true bladder wall disease, inducing a small anatomical functional bladder capacity. 14,15 This type of surgery was not proposed to patients with a more general pain syndrome corresponding to hypersensitization.
Similarly, in patients with refractory DO or impaired compliance on urodynamic studies, augmentation ileocystoplasty decreased intravesical pressures and consequently, improved patient comfort and protected their renal function. This procedure should be proposed, 16,17 but it provides excellent long-term functional results. However, in case of failure, the last option is to realize a urinary diversion, but with a nonnegligible impact on the body schema of patients.
Conclusion
This RSCAI technique comprises a robotic phase to perform supratrigonal cystectomy followed by mini-laparotomy for extraction of the cystectomy specimen and creation of the ileocystoplasty and a second robotic phase for anastomosis of the ileocystoplasty to the trigone. This approach was found to be reproducible with a rapid learning curve in terms of operating time. In particular, this technique decreased the major complication rate (Clavien >grade II), with the advantages of minimally invasive surgery. The long-term functional results were very satisfactory in these carefully selected patients.
Footnotes
Author Disclosure Statement
Prof. J.R. is a proctor (consultant) for Intuitive Surgical. The other authors have no personal financial or institutional interest in any of the drugs, materials, or devices described in this article.