
Abstract
Objectives:
To study the histopathologic changes in the urinary bladder associated with Double-J (DJ) stenting and the correlation between these changes and the period of stenting.
Methods:
In a 2-year period, a retrospective study was carried out on 30 patients indicated for DJ stenting. These patients underwent cold-cup cystoscopic biopsies from the ipsilateral ureteral orifice at the time of removal of DJ stents.
Results:
The mean age of the 30 patients included in our study was 43.6 ± 8.6 years (range 26–74 years). The stent size used was 4.7 and 6F. The stent duration was 2 weeks in 2 patients, 4 to 6 weeks in 18 patients, 6 to 12 weeks in 6 patients, and more than 12 weeks in the remaining 4 patients. Stent placement was optimum in all patients. The histopathologic study of 30 biopsies showed mild, acute eosinophilic inflammatory reactions with edema in patients with stenting less than 14 days. Acute lymphocytic eosinophilic cystitis with edema was found with stents of 2 to 6 weeks. Brunn's nests were reported with stents more than 6 weeks. Cystitis cystica was seen in those who had stents more than 12 weeks.
Conclusions:
Our study shows that acute and chronic allergic inflammatory changes can be seen around the bladder coil of the DJ stents. It is of major importance for the urologist to limit the use of DJ stents to highly indicated cases only and for a short interval.
Background
S
Methods
Between March 2013 and December 2015, 30 adult patients who had bladder biopsies at the time of DJ stent insertion and removal were included in the study. All the patients were informed in detail about the aims and procedures of the study and they signed a written informed consent prior inclusion into the study. The protocol and the written informed consent were approved by the local ethics committee of each study hospital (Al Azhar University Hospitals register trial number 7/2013). Bladder cold-cup biopsy has been taken from all patients before the insertion and during removal of the stent from around the ureteral orifice of the ipsilateral side of DJ stent insertion. However, in the case of any intraluminal reaction of the ureter or the renal pelvis, another biopsy was taken to compare it with the histopathology of the planned areas (Fig. 1). Moreover, when bladder polyps were seen at different areas in the bladder, different biopsies were taken for the pathologic examination. DJ stent period was considered according to the surgeon preferences and indications for stenting, that is, less than 2 weeks, between 2–4 weeks, 4–6 weeks, and more than 12 weeks. Then, the correlation between the histopathologic changes and the period of stenting was determined. All the patients had the same stents and the same surgical team.
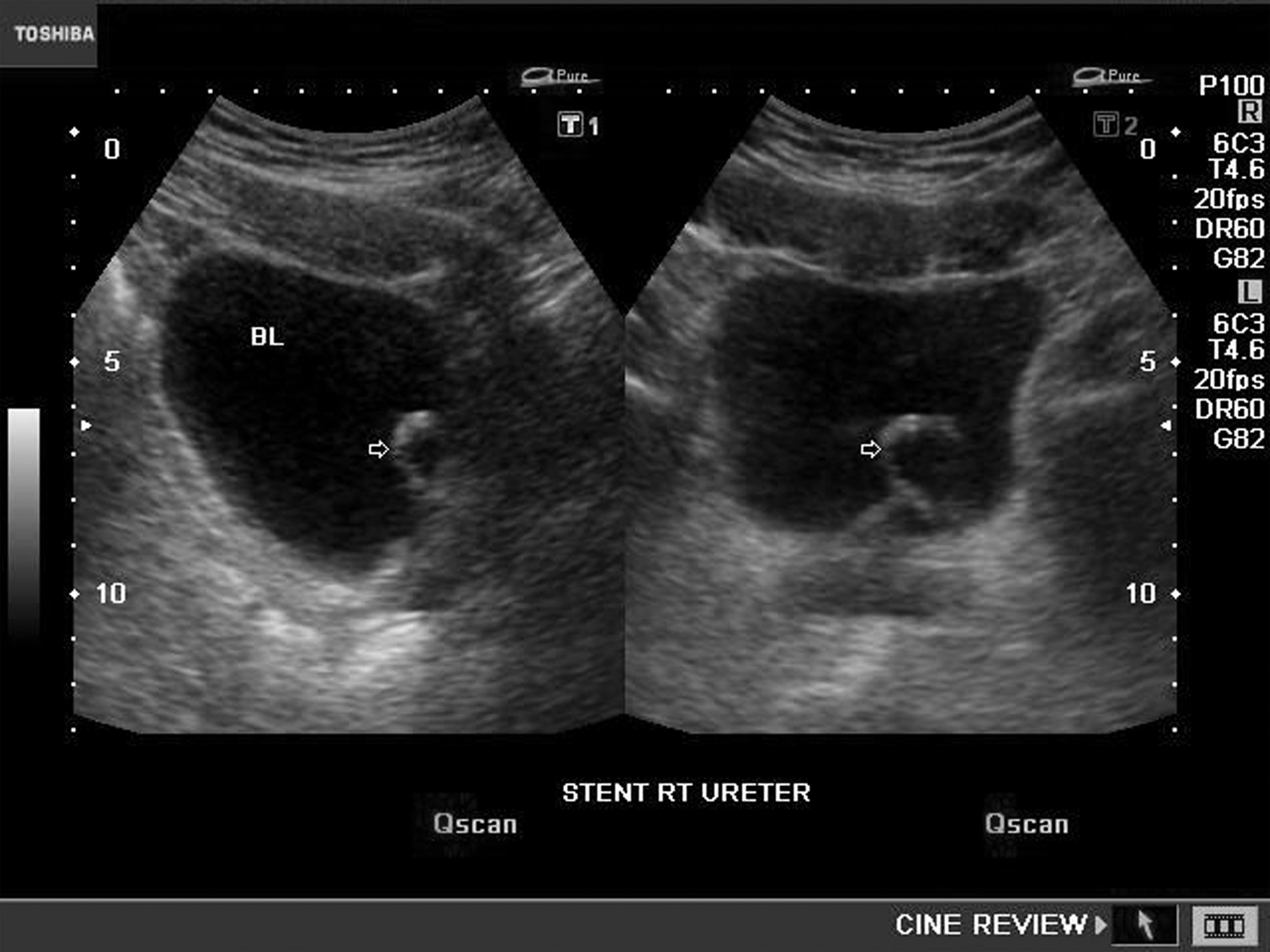
Image for bladder ultrasound shows edema around the coil of Double-J stent.
Inclusion criteria
Only patients with negative bladder biopsies at the time of stenting and had undergone bladder biopsies at the time of DJ stent removal were enrolled in our study. Patients with optimum stent placement with or without bladder growth around the DJ stent coil and had given consent for bladder biopsies at the time of removal were included in the current study.
Exclusion criteria
Patients with a history of bladder stones, specific and nonspecific urinary tract infections, bilharziasis, bladder malignancies, previous DJ insertion, intramural stone, positive histopathologic findings at the time of insertion, and migrated stents were excluded from our study. All stents that had positive cultures for bacterial infections after removal are excluded from our study.
Procedure
The DJ stent was placed with the patient under general or regional anesthesia and in the lithotomy position. Prophylactic antibiotics, as one dose of ceftriaxone or gentamicin before the procedure, were given to all the patients. The size (4.7–6F) and length of the stents (24–26 cm) selected by the surgeon depended on the patient's body size and the caliber of the ureter. The standard soft, single loop, silicone stents were used (Marflow AG, Soodstrasse 57, 8134 Adliswil/Zurich, Switzerland). Using a 22F cystoscope, the stent was placed in the required position over a guide wire under fluoroscopy monitoring. An ipsilateral bladder biopsy is taken from the area of ureteral orifice at the time of DJ stent insertion and sent for histopathologic examination. A plain film of the abdomen was taken as needed to confirm the position of the stent. All the patients were followed up in the outpatient clinic at 2–4 weeks. Depending on the indication for stent placement, the stent was removed by flexible cystoscopy under local anesthesia. Cold-cup biopsies were taken whenever there is any bladder reaction around the ipsilateral and trigone and sent for histopathologic examination by a single histopathologist in the same institution (Fig. 2).

Endoscopic view of the edema around the Double-J coil.
Results
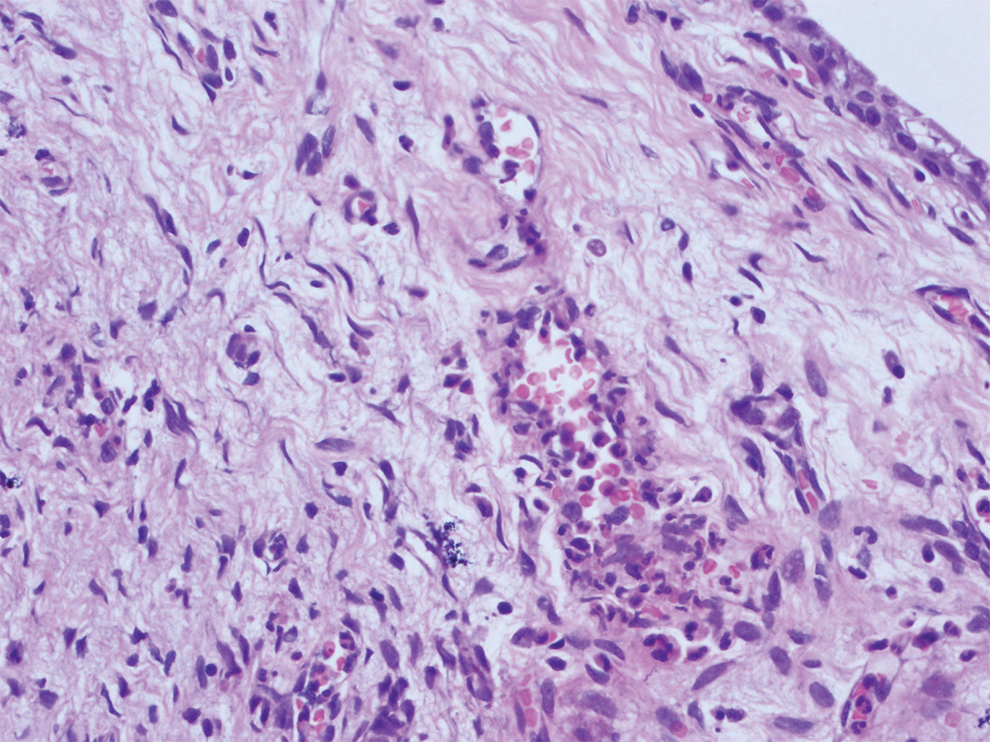
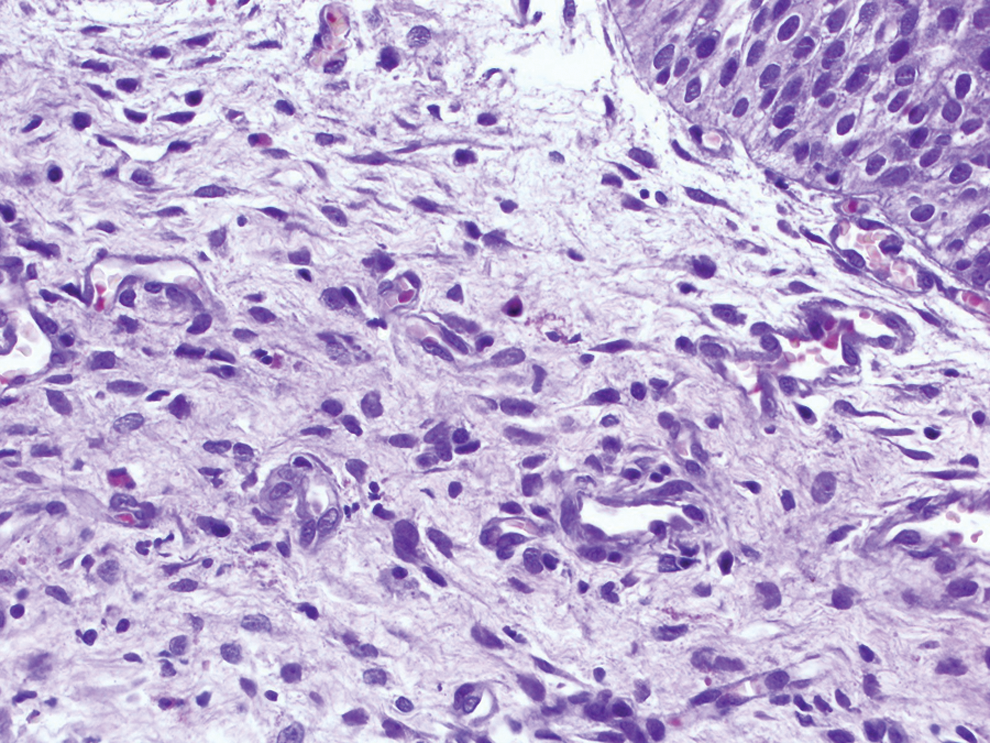
A total of 30 patients (28 males and 2 females) underwent unilateral DJ stenting within 2 years in our institution. The mean age of the patients was 43.6 ± 8.6 years (range 26–74 years). The stents were inserted on the right side in 11 patients and left side in 19 patients. The stent size used was 4.7 and 6F in our study (Table 1). DJ stenting (pre-extracorporeal shock wave lithotripsy) was observed in 6 patients, postureteroscopy in 18, post-PCNL (percutaneous nephrolithotomy) in 2, and forgotten DJ stents in 4 cases. In these four patients with forgotten stents, their DJ stents were planned to be removed after 3 months. Unfortunately, they did not come on the follow-up date for DJ stent removal. One patient came back after 9 months and the others completed 1 year (Table 2). The stent duration was 2 weeks or less in 2 patients, 4 to 6 weeks in 18 patients, 6–12 weeks in 6 patients, and more than 12 weeks in 4 patients (Table 1). Stent placement was optimum in all patients. Mild, acute eosinophilic inflammatory reactions with mild edema (Fig. 3) were reported in patients who had stenting less than 14 days. Acute lymphocytic eosinophilic cystitis with edema (Fig. 4) was found in patients who had stents 2 to 6 weeks. Brunn's nests (Fig. 5) were reported in all patients with stents of more than 6 weeks. Cystitis cystica (Fig. 6) was seen in all patients who had stents of more than 12 weeks (Table 3).
(H&E, 10×) Sections studied showed polypoidal mass lined by transitional epithelium. Underlying transitional epithelium shows congested blood vessels with neutrophilic and lymphocytic infiltration with mild edema. H&E = hematoxylin and eosin.
(H&E, 10 × ) Subepithelium showing eosinophilic and neutrophilic infiltration with mild edema. H&E = hematoxylin and eosin.
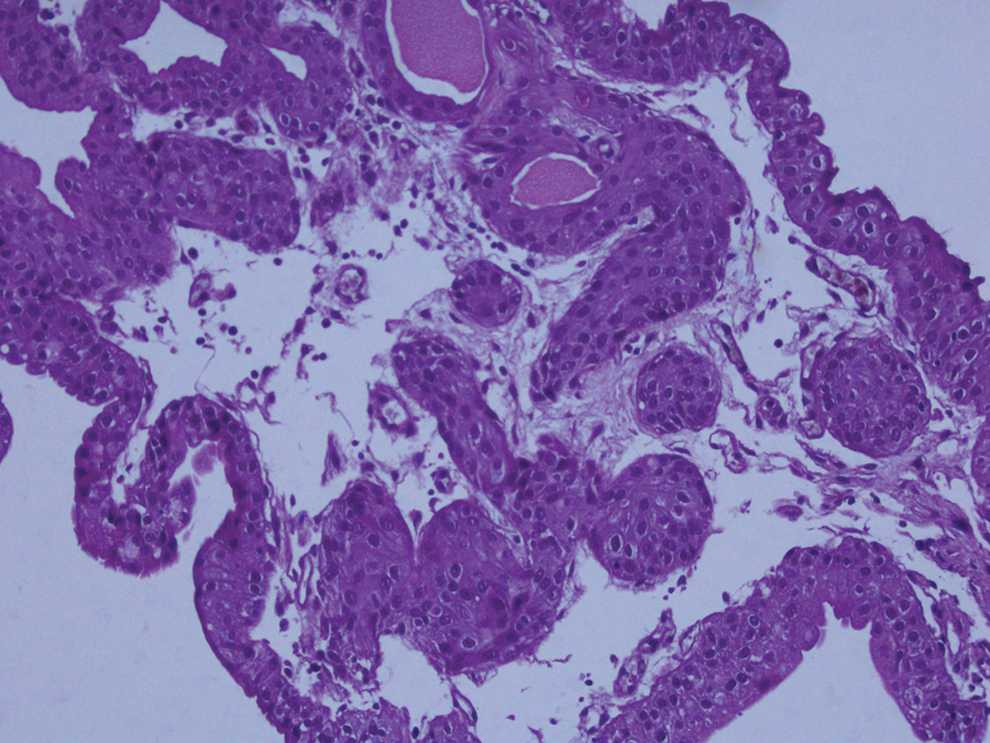
(H&E 40 × ) Sections that studied normal transitional epithelium going into the lamina propria in form of buds show normal transitional epithelium going as buds into the lamina propria with eosinophilic and lymphocytic infiltration and features of cystitis cystica. Von Brunn's nests are seen in the lamina propria. Stroma is edematous, and mild inflammation is seen.

(H&E × 40) Sections revealed focal proliferation of the basal layer of the transitional epithelium, producing solid nodules of Brunn's nests or islands within the lamina propria. Buds into the lamina propria with eosinophilic and lymphocytic infiltration and features of cystitis cystica are more predominant and frequently seen. Stroma is edematous and moderate to severe inflammation is seen.
DJ = Double-J; SWL = extracorporeal shockwave lithotripsy; PCNL = percutaneous nephrolithotomy; URS = ureteroscopy.
Discussion
The ureteral stents are commonly used in urologic practice for relief of ureteral obstruction. Despite the frequent use of ureteral stents, they are still associated with morbidity in about 80% of cases. 3,5 These side effects can be minor such as urinary frequency (50%–60%), urgency (57%–60%), dysuria (40%), incomplete emptying (76%), gross hematuria (25%), flank (19%–32%), or suprapubic pain (30%). 6 –11 Encrustation and bacterial adhesion are the most common problems of ureteral stents. 12,13
Al-Marhoon and colleagues studied the factors affecting the development of complications of DJ stenting in 220 patients and concluded that there is no correlation between the stent size and complication rates or better outcomes. However, they reported more complications with longer stents and poor outcomes with older patients after stenting. 14 Lee and coauthors compared 6F ureteral stents provided by five different manufacturers (Bard-Inlay, Cook Endo-Sof, Microvasive Contour, Applied Medical Vertex, and Surgitek Classic Double-Pigtail stent). Bard-Inlay was associated with less severe urinary symptoms although it had no impact on pain scores or narcotic use. 15
Ho and colleagues emphasized that all symptoms can be a consequence of associated stent morbidities such as urinary tract infection and encrustation, and the presence of these should be excluded by urinalysis and imaging as indicated. 16 Miyaoka and his coauthors explained that the cause of suprapubic pain might be due to direct irritation of the bladder mucosa by the DJ stent, and can be increased by the superimposed infection or stones. 17
Joshi and colleagues reported the evaluation of the symptoms associated with stents. They prospectively assessed lower urinary tract symptoms caused by DJ ureteral stents using validated questionnaires (International Prostatic Symptoms Score—IPSS, International Continence Society male questionnaire, Quality of Life questionnaires, and the Bristol Female Lower Urinary Tract Symptoms questionnaire—BFLUTS). 11 They reported the association of urinary symptoms with stents and they showed the negative impact of these symptoms on patients' quality of life. The importance of their study is that they brought researchers' attention to the need for the development of a stent-related symptom score measurement. 11
In our study, we tried to understand the underlying histopathologic changes in the urinary bladder due to the temporary presence of DJ stent. We found that these reactions increase and become severe as the stent duration increased. Acute eosinophilic inflammatory reaction with mild edema was observed in stent duration of fewer than 2 weeks. We found that in stenting patients with DJ for 2 to 4 weeks, the histopathologic study of their biopsies showed acute lymphocytic eosinophilic cystitis with severe edema. The inflammatory reaction became more severe and evident with Brunn's nests at 4 to 6 weeks. Cystitis cystica and Brunn's nests were seen frequently in patients who had stents lasting more than 3 months. It is clear from the current study that when the period of stenting increased, the reaction changed from acute stage to chronic especially after 3 months.
Eosinophilic cystitis is a rare and poorly understood inflammatory disorder of the urinary bladder that was first described by Brown in 1960. 18 It has been reported in chronic vesical irritation, food or drug allergy, bladder surgery or injuries, parasitosis, or malignancy. Thompson and colleagues stated that the pathogenesis of eosinophilic cystitis is still unclear. 19,20 In our study, the eosinophilic reaction started as early as 1-week post-DJ stent placement. The patients complained of mainly urinary frequency and dysuria with the cystoscopic finding of papillary reaction over the ipsilateral ureteral orifice and trigone. However, this reaction increases and progresses to the lymphocytic eosinophilic reaction from the time of 2–6 weeks up to cystitis cystica in patients with stents longer than 12 weeks.
Our results clarified the histopathologic morbidity of the DJ stenting. However, there are many questions that should be clarified in the future such as whether the histopathologic morbidity is related to only the stents used or with all types of stents. The correlation between the symptom severity and the histopathologic changes should be studied. The period of stenting was clear in our study, related to an acute phase that changed to chronic with stenting. Brunn's nests and cystitis cystica were seen in long-standing stents inside the ureter.
We claim that the technique or procedure used followed by DJ insertion will not affect the bladder reactions associated with DJ stents. Several studies reported that urothelium trauma or tears heal within 2–5 days. 21 –25 We should claim that the reactions documented are acute and/or chronic allergic cystitis, which are linked to the bladder irritation due to the presence of the foreign body in the ureter and the bladder (DJ stents). In our study, we used two different sizes of DJ stents (4.7–6F). We claim that the bigger size of the stent may aggravate the reaction, but it will not change the nature of the reaction to eosinophilic lymphocytic cystitis. We did not correlate the size of the stent to bladder histopathologic changes. More studies with more patients are required to give a firm conclusion for all of the previous points.
To the best of our knowledge, this is the first study to report the histopathologic changes due to DJ stenting. More studies are needed to clarify all related points with a larger number of biopsies and patients with a prospective study. The proposed study should be multicenter study and correlate the urinary bladder histopathologic changes with the lower urinary symptoms of this group of patients, using validated questionnaires as used by Joshi and colleagues. 12
As this study is a preliminary study, no solid conclusion can be drawn according to the results obtained with this small number of patients. In the future, we plan for a prospective study with more patients to correlate the bladder histopathologic changes to different stent materials, different stent sizes, and different stent lengths. Moreover, more studies are needed to correlate bladder histopathologic changes due to DJ stenting to the presence/absence of urinary tract infections and the associated lower urinary tract irritative symptoms. We plan for long-term follow-up for the current study group by another biopsy to check if these histopathologic changes are temporary, permanent, or progressive after 1 year. One study will not be enough to include all of these parameters. More research and more effort will be needed to give a solid conclusion about the bladder histopathologic changes after ureteral DJ stenting.
We can suggest that due to the clinical hazards of DJ stenting and pathologic changes, the urologists might consider limiting the use of stents and try to shorten the period. Until now, we do not have the ideal stents.
The ideal ureteral stent should be easy to insert and remove, drain the upper tract extremely well, free from side effects such as irritative symptoms, resist encrustation, infection, and migration, radiopaque or visible with ultrasound, and nonrefluxing, durable, and degradable if forgotten; however, such a stent is still not available up till now.
Conclusions
Our study shows that acute and chronic allergic inflammatory changes are seen around the coil of DJ stents. Our preliminary results suggest that the use of DJ stents should be limited to highly indicated cases only. Future prospective multicenter studies with more patients are needed to confirm the present conclusions.
Authors' Contribution
H.A. has made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data. M.G. has been involved in drafting the manuscript or revising it critically for important intellectual content and has given the final approval for the version to be published.
Ethical Approval
All procedures performed in this study were in accordance with the ethical standards of the Institution and/or National Research Committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The protocol and the written informed consent were approved by the local ethics committee of each study hospital (Al Azhar University Hospitals and Menoufia University Hospital, Egypt).
Informed Consent
Informed consent was obtained from all the patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.