
Abstract
Introduction:
The forgotten ureteral stent (FUS) can lead to patient morbidity. To date, tracking ureteral stents is a cumbersome task, given their high frequency of insertion and variable indwelling times. To simplify this process, an application was developed to track patients with indwelling ureteral stents. We report our initial user experience and clinical outcomes with this application.
Methods:
Ureteral Stent Tracker™ (UST) is a secure, Health Insurance Portability and Accountability Act (HIPPA)-compliant, cloud-based point-of-care application. It is designed for logging stent insertion, scheduling the date of anticipated stent extraction, and confirming stent removal. It is accessible via a mobile phone application or web browser interface. We consecutively enrolled all patients who underwent ureteral stent insertion for any indication by two urologists from January 10, 2015, to October 10, 2016. A retrospective chart review was performed of all patients included in the UST database. Data extracted included patient demographics, diagnosis, procedure, and stent characteristics.
Results:
A total of 115 patients were included with a mean age of 52.4 years; 54% (62/115) were male and 58% (67/115) were Caucasian. This cohort represented 146 ureteral stent care plans with 23 patients (23/115; 20%) having more than one care plan during the study period. The most common procedure performed was ureteroscopy (70/146; 48%) for a diagnosis of nephrolithiasis (108/146; 74%). The median indwelling ureteral stent time was 14 days (interquartile range: 7–45 days). A total of three patients (3/115; 3%) did not return for their scheduled extraction, but were identified only through the application. Each patient was contacted, resulting in effective removal of all three stents in the office.
Conclusions:
Tracking of ureteral stents is critical to prevent the patient safety issue of the FUS. The UST is a secure, HIPPA-compliant, cloud-based application, which once incorporated into the workflow of a urologic practice can prevent the FUS.
Introduction
I
To prevent the FUS, urologists have developed several strategies to track ureteral stents after insertion. These include a simple paper card registry that requires manual entry and review, a more advanced electronic database, and a contemporary web-based system with barcode entry and automatic e-mail reminders. 7,8 Despite the value of these strategies, they all suffer from similar limitations. Specifically, they are not available at the point-of-care (POC) or outside of a single institution.
To simplify this process, a Health Insurance Portability and Accountability Act (HIPPA)-compliant, cloud-based POC application, which is universally available across all healthcare environments, was developed to track patients with indwelling ureteral stents. We report our initial user-experience and clinical outcomes with this application to prevent the FUS.
Patients and Methods
Study population
The study population included all patients who underwent ureteral stent insertion for any indication by two urologists (authors J.B.Z. and B.R.M.) at Johns Hopkins Hospital (JHH), which is a tertiary care academic medical center. Patients were enrolled consecutively based on their date of surgery from October 1, 2015, to October 31, 2016.
Application
Visible Health, Inc., in partnership with Boston Scientific Corporation developed Ureteral Stent Tracker™ (UST). UST is a secure, HIPPA-compliant, cloud-based POC application. It is accessible via a mobile phone application or web browser interface. It is designed for logging stent insertion, scheduling the date of anticipated stent extraction, and confirming stent removal. It is available to any consumer, not just those in contract with Boston Scientific Corporation.
For each patient, a unique profile with name and medical record number was created (Fig. 1). Within the profile, one (or multiple) stent care plan(s) was created that included date of insertion, laterality, date of anticipated extraction, and confirmed date of removal (Fig. 2). Additional notes about follow-up were documented in the notes section. This information was shared across the practice through the application. At login, all stent care plans were reviewed through a real-time visual dashboard (Fig. 3). The stent care plans are visually coded to allow for easy identification of patients with stents that have exceeded their anticipated extraction date. This information is also sent as a weekly e-mail reminder to all providers in the practice.
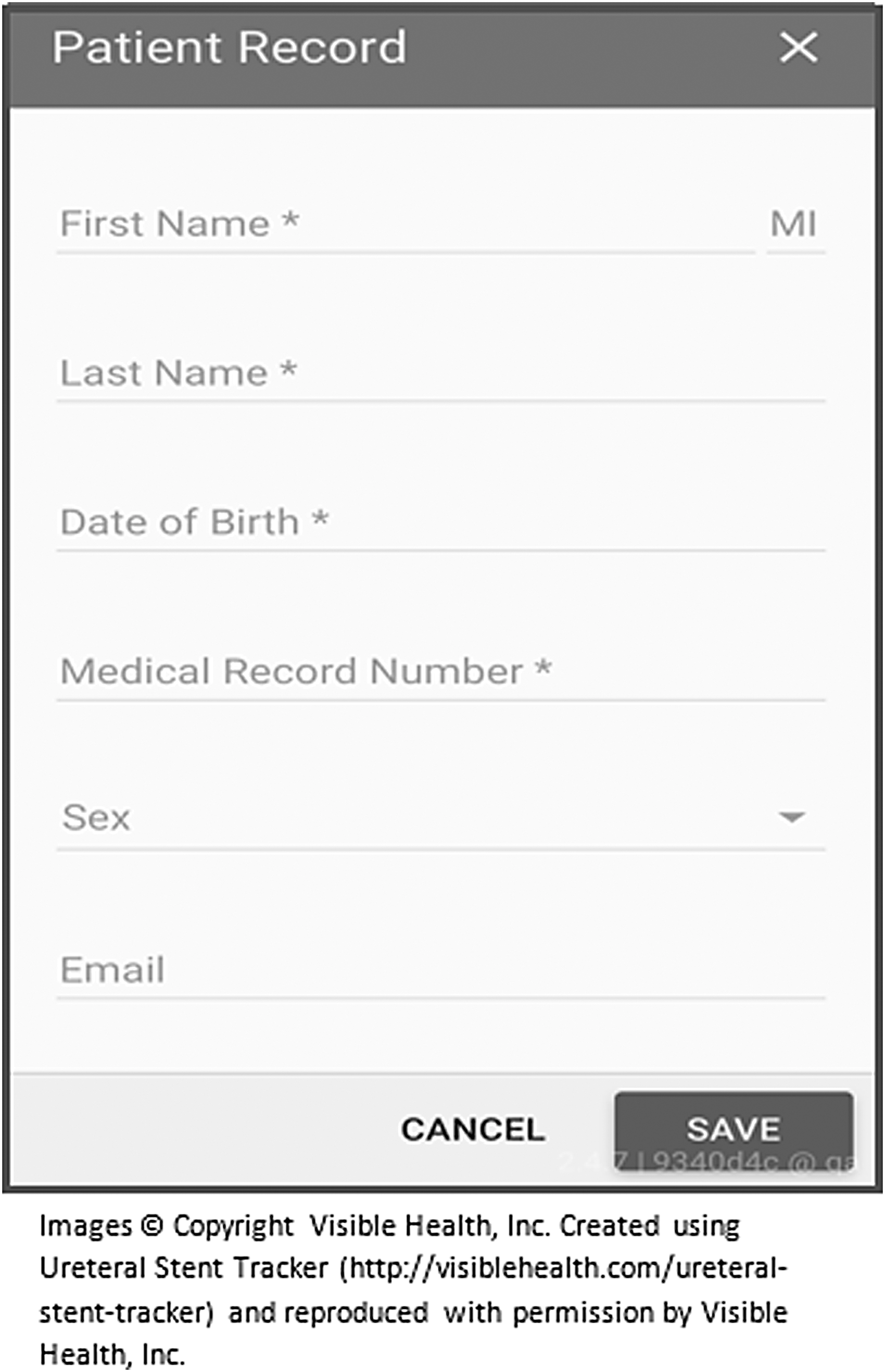
Patient profile entry interface.

Ureteral stent care plan.
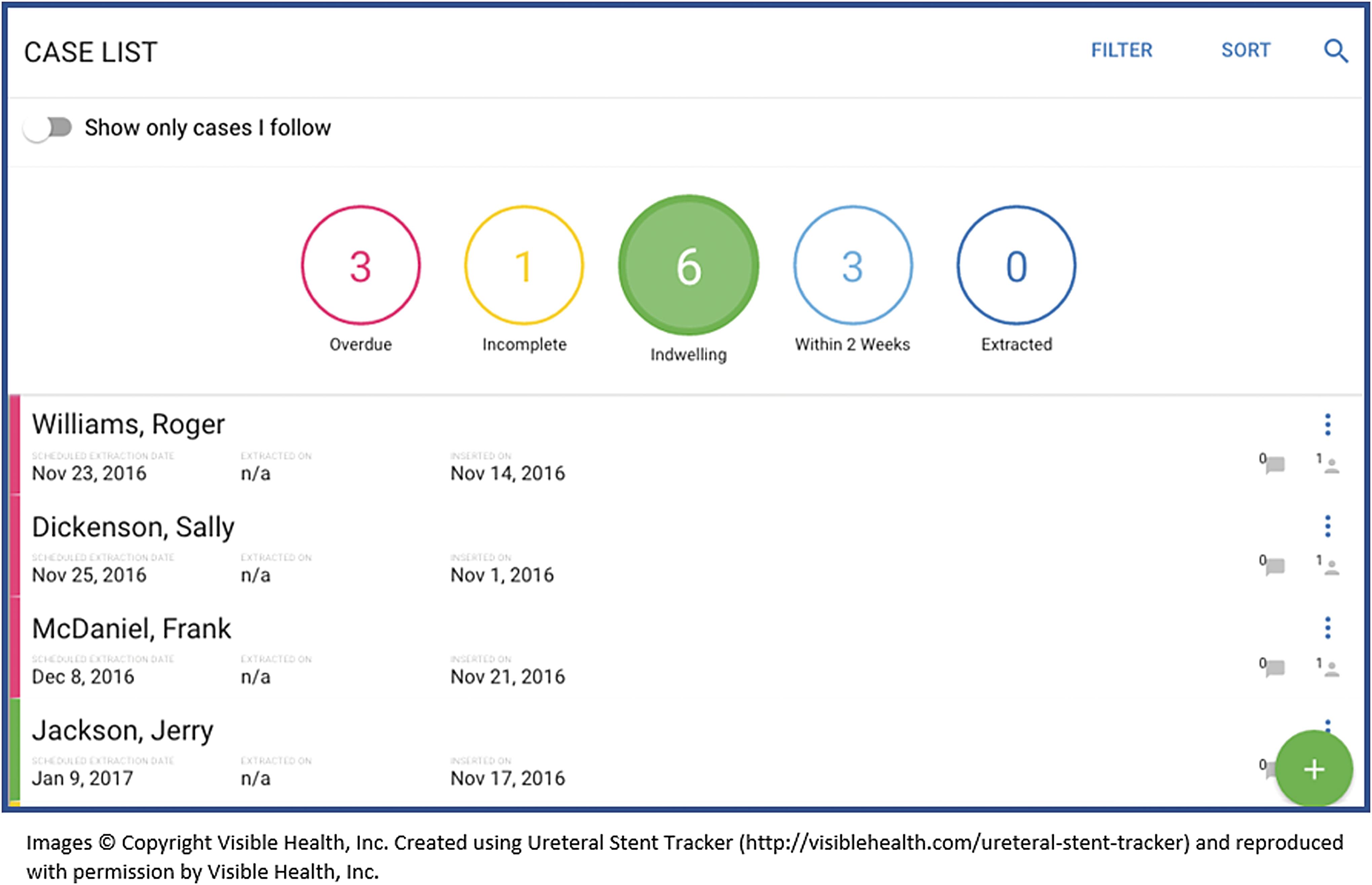
Ureteral stent care plan dashboard.
Integration into practice
Before the introduction of the UST, there was no uniform system in place at JHH to track ureteral stents. The availability of the application represented an opportunity for improved patient safety and was quickly adopted by J.B.Z. and B.R.M. in the Division of Endourology. All entries were made in the operating room at the POC via either the mobile phone application or web browser interface. This was by design to ensure that each patient with a stent was entered into the UST. When a ureteral stent was documented as removed, either in the clinic or operating room, then the care plan was updated, again at the POC. Each week, the UST visual dashboard was reviewed to identify patients who had exceeded their anticipated extraction date, which signified that they had not returned for scheduled follow-up. These patients were then contacted. The care plan was not updated to reflect removal until a healthcare provider could verify and confirm stent extraction.
Analysis
A retrospective chart review was performed of all patients included in the UST database. A patient could only have one profile, but could have more than one ureteral stent care plan during the study period. Bilateral ureteral stents were counted as one ureteral stent care plan, if inserted during the same operative session. Data extracted included patient demographics, diagnosis, procedure, and stent characteristics, such as indwelling time. Descriptive statistics were performed using IBM SPSS Statistics for Windows, Version 24 (IBM Corp., Armonk, NY). This study was reviewed by the institutional review board and informed consent was waived.
Results
A total of 115 patients were included, which represented 146 ureteral stent care plans. Table 1 outlines patient demographics. A total of 23 patients (23/115; 20%) had more than one ureteral stent care plan during the study period. Table 2 shows the procedural characteristics for all ureteral stent care plans. During the study period, a total of three patients (3/115; 3%) did not return for their scheduled extraction, but were identified only through the application. Each patient was contacted, resulting in effective removal of all three stents in the office.
N = 115.
SD = standard deviation.
N = 146.
IQR = interquartile range.
At the end of the study period, there were 14 (14/146; 10%) ureteral stents still indwelling. Of these patients, 12 (12/146; 8%) were appropriately awaiting their upcoming procedures, while 2 (2/146; 1%) had stents indwelling beyond their maximal safe life. One patient is on hospice and one was unable to be contacted, despite multiple attempts via telephone and certified mail.
Interestingly, a total of four patients (4/115; 4%) had a history of being lost to follow-up after a prior stent insertion. All of these patients presented with an encrusted ureteral stent, requiring a percutaneous nephrolithotomy for removal. A new ureteral stent was inserted in each case and the patients were added to the UST. After entry, none (0%) of these patients was lost to follow-up, each having the stent appropriately removed in the office.
Discussion
Ureteral stent insertion remains one of the most common procedures performed by urologists. 1 Once inserted, it is both the physician's and patient's responsibility to ensure timely, appropriate removal or exchange. However, this does not always occur, resulting in an FUS.
As the FUS continues to dwell in the urinary tract, it is at risk for both incrustation and encrustation, which can occur relatively rapidly. 9 When encrustation does develop, it can result in patient morbidity and, rarely, even in mortality rate. 3 In an analysis of 22 FUS from 1990 to 1994, 32% of patients presented with a urinary tract infection and 10% presented with pyelonephritis. 2 All patients required more than simple cystoscopy for removal with 27% requiring more than one procedure. 2 A similar analysis of 26 FUS from 1998 to 2002 demonstrated a mean of 2.7 procedures (range 1–4) to completely remove the FUS and alleviate the stone burden. 10 Subsequent series have demonstrated comparable results with the necessity for more invasive and additional procedures for stent and stone clearance. 4 Together, the complicated presentation and the need for complex surgery all contribute to an increased cost of care, which is estimated at almost sevenfold higher than timely, appropriate removal. 5
With the risk of complications from an FUS high, urologists need adequate strategies to ensure proper ureteral stent removal. One option is through the identification of risk factors for an FUS. In an analysis of 28 FUS, male gender and uninsured were both associated with an FUS. 11 Thus, the authors concluded that increased attention should be given to these at-risk groups. 11 Although this information is potentially useful, it alone is not sufficient to prevent the FUS, particularly in patients without these risk factors. Therefore, alternative approaches are needed.
One such approach is the ureteral stent log. In 2008, Tang and colleagues described their single-center experience in the United Kingdom with a ureteral stent card registry. 8 An audit of their practice revealed 6% of patients who had a stent inserted, but who were not included in the registry. 8 Furthermore, 25% of patients had no documentation of stent removal in the registry with 5% of patients overdue. 8 All of these patients were ultimately contacted and all had their stents removed appropriately. 8 The authors attributed this deficiency to the cumbersome task of manual review of the cards, and that patients often had their ureteral stents removed at other facilities. 8
Unlike paper-based systems, computerized tracking has the benefit of ease of data entry, ability to rapidly search, and access across multiple sites. In 2007, Lynch and colleagues described their experience with a ureteral stent database housed within their center's electronic medical record (EMR). 7 An audit of their system demonstrated that 13% of stents were not captured within the database, even after implementation of a barcode for data acquisition. 7 A total of 49% of the stents extended beyond their anticipated removal date, but all were subsequently removed within 21 days. 7 This is likely due to the e-mail reminder function of the system with 83% of notifications resulting in an action plan within 4 days. 7
To ensure complete capture of all inserted ureteral stents, a billing-based system was recently described by Baumgarten and colleagues. 12 In this system, ureteral stent insertions are automatically identified by the ICD-9 procedure code with an accuracy rate of 85%. 12 Once a ureteral stent is identified by the system, then a reminder letter is sent to the patient and uploaded to the EMR. 12 It is unclear if the reminder letters alone will reduce the rate of FUS. 12
Although strategies to track ureteral stents have evolved from cumbersome paper logs to computer-based systems, a constant limitation was that they were only available at the creating institution. The UST has eliminated this constraint. It is a commercially available product that can be used as stand-alone application or integrated into an EMR. It is secure and HIPPA compliant. It can function across practice settings and environments via a cloud-based smartphone application or web browser interface. This makes it available at the POC facilitating data entry for both ureteral stent insertion and extraction.
Unfortunately, it is not possible to determine if we improved our ability to prevent the FUS, given we have no historical comparison data. Nevertheless, we found the UST to be easily and effectively incorporated into a busy endourologic practice. Particularly helpful was the cloud-based functionality that allowed us to transition across practice environments from the operating room to the clinic, updating ureteral stent insertion and removal at the POC. This facilitated capture of all inserted ureteral stents and documentation of all extractions, which was a major limitation of prior strategies. 7,8,12,13 The real-time dashboard and the weekly notifications were critical to the detection of three patients (3/115; 3%) who did not return for their scheduled removal, and would have otherwise been lost to follow-up. These patients were spared the potential morbidity of an encrusted ureteral stent. 2,5,10 However, this was not the case for a small subgroup of patients (4/115; 4%) who were referred to us for the complications from an FUS. In this high-risk cohort, all 4 patients had their new, postprocedural ureteral stents appropriately removed in the office. With entry into the UST, none was again lost to follow-up.
Despite the potential of the UST, there are limitations in its ability to prevent all future FUS. First, the application is not completely automated in adding or removing ureteral stents to and from the database, even when integrated into the EMR. Presently, ureteral stent care plans need to be created and modified by a human. Second, even if the UST could automatically detect both ureteral stent insertion and removal through the EMR, the notification of an overdue ureteral stent would still require human action for resolution. Third, patients may have their ureteral stents removed at home, in the emergency department, or by another urologist, which makes confirming removal challenging. Future versions of UST could include a patient portal or smartphone application. This could house a ureteral stent identification card, provide educational materials, push removal reminders, and allow for patients or other physicians to securely document extraction. Finally, urologists are not the only physicians inserting ureteral stents, and thus, we must share our effective strategies, such as UST with our colleagues.
Unfortunately, humans are fallible, 14 and even with the best ureteral stent tracking application, patients will be missed. Therefore, if we are truly committed to patient safety surrounding ureteral stents, then we must not rely only on technologic solutions, but instead develop a comprehensive systems-based strategy. 15 In this framework, countermeasures can be developed at every level of the system (e.g., institution, practice, team, provider, task, and patient) to prevent errors, detect them when they do occur, and mitigate their effects. 14,15 For example, at the institutional level, a policy could be created which mandates that implants such as ureteral stents be logged/tracked and that confirmation of the logging/tracking (into UST) be included as part of the universal surgical safety timeout and debrief in the operating room. 16 This procedure would create an additional layer of accountability on the part of the urologist and circulating nurse to ensure that the new stent is added to or removed from the UST before leaving the operating room. Similarly, at the practice or team level, notification of overdue ureteral stents from UST can be primarily assigned to the patient's urologist, and also simultaneously directed to the scheduling team and practice manager or charge nurse. Once notified, the scheduling team can coordinate a timely follow-up appointment, and the practice manager or charge nurse can discuss the case with the urologist to help mitigate barriers to stent removal. Again, this would add redundancy to the system, which is particularly important in situations where one urologist inserts the ureteral stent, but another is charged with removing it. Although these represent potential examples of systems-level interventions aimed at preventing the FUS in the context of UST, it is important to understand that each practice will have unique workflows, resources, and safety cultures that necessitate designing and deploying individualized strategies.
Conclusion
The FUS is a risk in a busy urologic practice. Therefore, tracking of ureteral stents is critical to prevent this patient safety issue. The UST is a commercially available, secure, HIPPA-compliant, cloud-based application that is accessible via a web browser or smartphone for use in managing ureteral stents. Once incorporated into the workflow of a urologic practice it can help to prevent the FUS.
Footnotes
Acknowledgments
We thank Mr. and Mrs. Jerry and Helen Stephens for their continued support of kidney stone disease research at the Brady Urological Institute. We also thank Visible Health, Inc. for providing us with the screenshots for the figures.
Author Disclosure Statement
J.B.Z., W.W.L., L.R., and E.C. have no competing financial interests. B.R.M. is a consultant for Boston Scientific Corporation.