
Abstract
Objective:
In the perioperative period, renin–angiotensin–aldosterone system (RAAS) inhibitors may result in cardiovascular and renal functional changes. We sought to determine the acute and chronic renal functional and blood pressure effects of continuing or withdrawing angiotensin-converting enzyme inhibitors (ACE-I) and angiotensin receptor blockers (ARBs) after percutaneous nephrolithotomy (PCNL).
Materials and Methods:
This was a retrospective review of all patients undergoing PCNL at our institution from 2002 to 2013. Patients on either an ACE-I and/or ARB who received an ACE-I and/or ARB during their surgical hospitalization were matched based on sex, age, and body mass index to patients who had their medication withheld during the postoperative period. The two groups were compared.
Results:
A total of 2784 patients underwent PCNL during the study period. At the time of PCNL, 15.2% (423/2784) of patients and 6.5% (181/2784) were prescribed an ACE-I and an ARB, respectively. Fifty-nine percent (248/423) of patients on an ACE-I and 66.9% (121/181) on an ARB received their medication during their postoperative hospitalization. There was no significant difference in average length of stay (2 days vs 2 days), perioperative change in glomerular filtration rate, glomerular filtration rate (GFR) (−0.50 mL/min/1.73 m2 vs −2.34 mL/min/1.73 m2, p = 0.267), change in GFR at 1 month postoperatively (−4.63 mL/min/1.73 m2 vs −5.90 mL/min/1.73 m2, p = 0.748), or change in GFR at 1 year (−2.08 mL/min/1.73 m2 vs −0.13 mL/min/1.73 m2, p = 0.267) between patients who received vs withheld their medication during the postoperative stay.
Conclusion:
It is safe to continue RAAS inhibitors in patients undergoing PCNL during their operative hospitalization.
Introduction
T
Additionally, animal and humans studies have suggested that PCNL is associated with acute unilateral decline in renal function, possibly secondary to renal vasoconstriction. 5,6 The continuation of RAAS inhibitors during the PCNL perioperative period may result in renal function changes through fluctuations in renovascular effects. Conversely, withholding a patient's prescription during inpatient hospitalization increases the risk of inadvertent discontinuation due to errors in medication reconciliation at the time of discharge. 7,8
A 2016 Cohrane Database review of seven randomized controlled trials of patients undergoing cardiovascular surgery did not find evidence to support the use of perioperative RAAS inhibitors in preventing mortality, morbidity, and complications (hypotension, cerebrovascular complications, and cardiac surgery-related renal failure). 9 With regard to noncardiac surgery, data exist to support withholding RAAS inhibitors in the perioperative period during orthopedic and bariatric surgery to prevent postoperative acute kidney injury (AKI). 10,11 Recent data have shown resumption of RAAS inhibitors to be safe following partial nephrectomy, with an associated decreased risk of heart failure and severe renal injury. 12 We conducted a retrospective review of all patients undergoing PCNL at our institution to determine the effects of continuing a patient's prescribed ACE-Is and/or ARB during the perioperative period and up to 1 year following the procedure.
Materials and Methods
Our study received IRB approval. The population consisted of 2784 patients who underwent PCNL between July 19, 2002 and October 14, 2013 at our institution. The following demographic data were extracted from electronic patient medical records: sex, birth date, body mass index (BMI), hospital admission date, and hospital discharge date. Medication information included if the patient was prescribed an ACE-I or an ARB and the doses. Preoperative vital signs extracted included systolic blood pressure (SBP) and diastolic blood pressure (DBP). Preoperative blood pressure measurements were obtained anywhere from 1 to 140 days before the date of surgery. Preoperative laboratory values collected included blood urea nitrogen, serum creatinine (SCr), glomerular filtration rate (GFR), and serum hemoglobin. GFR was calculated utilizing the Modification of Diet in Renal Disease Study equation: GFR (mL/min/1.73 m2) = 175 × (Scr)−1.154 × (Age)−0.203 × (0.742 if female) × (1.212 if African American). 13 Inpatient perioperative data extracted included GFR and SBP/DBP during the inpatient perioperative period. Perioperative blood pressure was calculated as a mean of intraoperative and immediate postoperative pressure readings. Posthospitalization data extracted included SCr/GFR and SBP/DBP at ∼1 month postoperatively, SCr/GFR and SBP/DBP at ∼6 months postoperatively, and SCr/GFR at 1 year postoperatively. Patients were excluded from analysis if relevant data were not available or if they had not completed the follow-up schedule. Individuals taking a RAAS inhibitor who were prescribed these medications during their postoperative inpatient recovery were matched by age, sex, and BMI to patients who had their RAAS inhibitor withheld during their postoperative inpatient recovery. The decision to continue or withhold ACE-I or ARB was at the discretion of the preoperative anesthesia provider. Patients instructed to stop their RAAS inhibitor, were asked to not take the morning dose of their medication. The student's t-test was used to compare mean for the two groups for normally distributed data. JMP version 10.0 was used to perform the statistical tests. All tests were two-tailed, and p < 0.05 was considered statistically significant.
Results
A total of 2784 patients underwent PCNL during the review period. At the time of PCNL, 15.2% (423/2784) of patients had a listed prescription for an ACE-I in the medical record and 6.5% (181/2784) had a listed prescription for an ARB. Fifty-nine percent (248/423) of patients on an ACE-I and 66.9% (121/181) on an ARB had their medication administered during their operative hospitalization. Therefore, 369 patients received a RAAS inhibitor during hospitalization and 235 patients had their RAAS inhibitor held.
Patients who had their ACE-I or ARB withheld during their inpatient hospitalization were matched by age, sex, and BMI to patients who had their ACE-I or ARB administered during their hospitalization. To qualify as a match, the difference in ages between patients in a pair was required to be less than or equal to 3 years. The difference in BMI was required to be less than or equal to 3 kg/m2. A total of 132 pairs of patients (264 patients) who were prescribed either an ACE-I or ARB were selected from the overall cohort based on the above match criteria.
Table 1 lists the clinical and demographic data for the two groups. About 54.5% of the subjects in each group were male. Comparing patients who had their medication administered during their postoperative inpatient admission vs patients who had their medication withheld, there was no statistically significant difference in patient age at the time of PCNL (62 vs 61, p = 0.268). There was no significant difference in BMI (32.9 kg/m2 vs 33.1 kg/m2, p = 0.979), preoperative SBP (132 mm Hg vs 131 mm Hg, p = 0.726), preoperative DBP (73 mm Hg vs 74 mm Hg, p = 0.483), preoperative SCr (1.02 mg/dL vs 1.05 mg/dL, p = 0.443), preoperative glomerular filtration rate, GFR (72.5 mL/min/1.73 m2 vs 69.8 mL/min/1.73 m2, p = 0.355), preoperative serum hemoglobin (13.4 g/dL vs 13.2 g/dL, p = 0.392), and length of postoperative inpatient admission (2 days vs 2 days, p = 1.0).
ACE-I = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMI = body mass index; DBP = diastolic blood pressure; GFR = glomerular filtration rate; Hgb = hemoglobin; PCNL = percutaneous nephrolithotomy; SBP = systolic blood pressure; SCr = serum creatinine.
Figure 1 demonstrates the change in GFR perioperatively, at 1 month, at 6 months, and at 1 year, which is our institutional schedule for follow-up. Tables 2 and 3 list the changes in renal function for the two groups. Comparing patients who had their medication administered vs patients who had their medication withheld, there was no significant difference in mean perioperative change in GFR (−0.50 mL/min/1.73 m2 vs −2.34 mL/min/1.73 m2, p = 0.267), change in GFR at 1 month (−4.63 mL/min/1.73 m2 vs −5.90 mL/min/1.73 m2, p = 0.748), change in GFR at 6 months (−1.90 ml/min/1.73 m2 vs +2.09 ml/min/1.73 m2, p = 0.359), or change in GFR at 1 year postoperatively (−2.08 mL/min/1.73 m2 vs −0.13 mL/min/1.73 m2, p = 0.573).
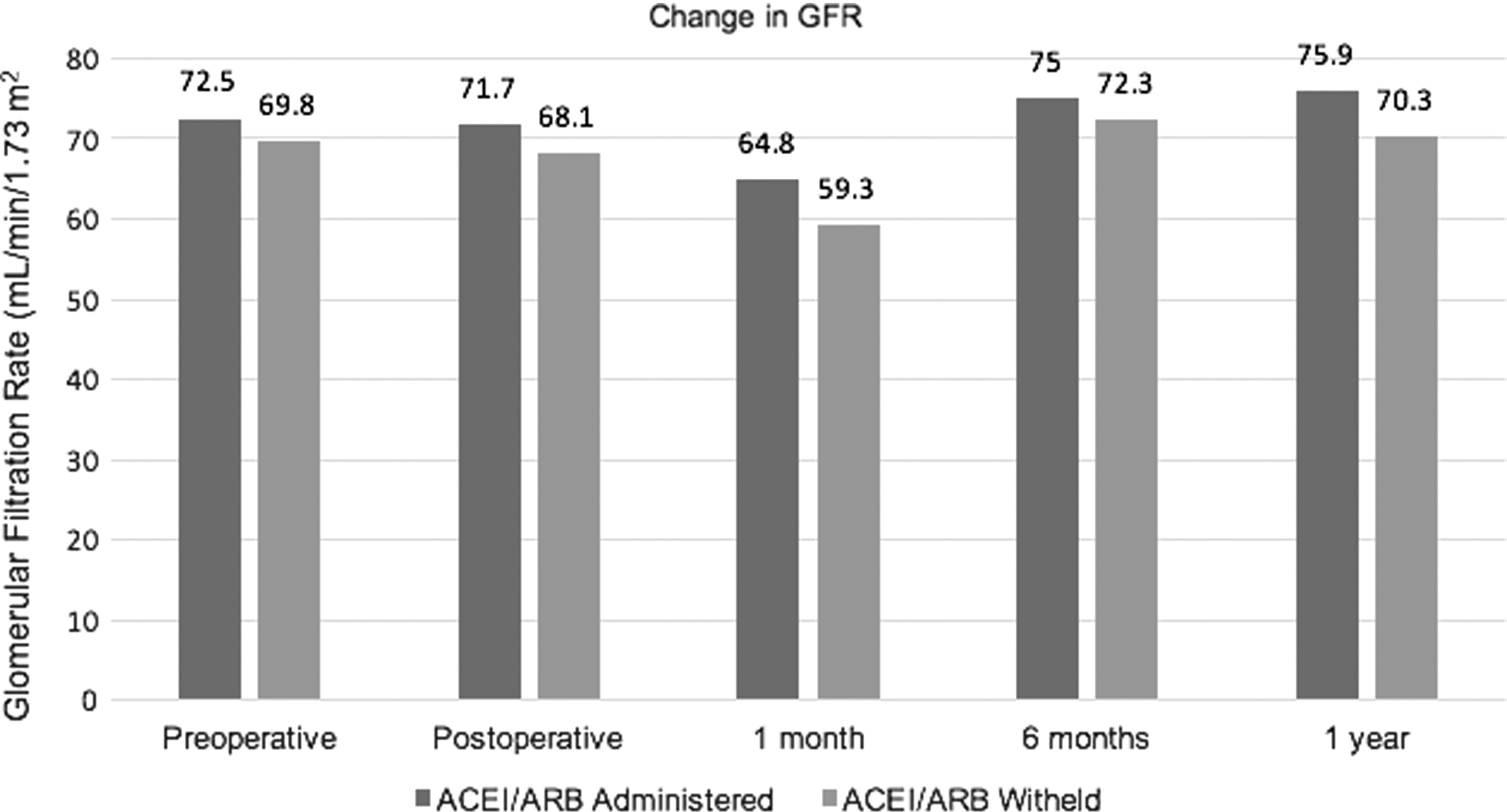
Mean GFR perioperatively, at 1 month, at 6 months, and at 1 year in patients receiving vs holding ACE-I/ARB. ACE-I = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; GFR = glomerular filtration rate.
Table 4 lists the changes in systolic and DBP for the two groups. Comparing patients who had their medication administered vs patients who had their medication withheld, there was no significant difference in mean change in perioperative SBP (−2.5 mm Hg vs −2.79 mm Hg, p = 0.943), mean change in perioperative DBP (−3.43 mm Hg vs −1.77 mm Hg, p = 0.461), mean change in SBP at 1 month postoperatively (+2.25 mm Hg vs −2.0 mm Hg, p = 0.235), mean change in DBP at 1 month postoperatively (+4.72 mm Hg vs +4.27 mm Hg, p = 0.807), mean change in SBP at 6 months postoperatively (1.03 mm Hg vs −3.69 mm Hg, p = 0.243), and mean change in DBP at 6 months postoperatively (+2.94 mm Hg vs +1.61 mm Hg, p = 0.521).
Discussion
Many variables account for fluctuations in perioperative renal function after PCNL, including hypotension and blood loss (prerenal), parenchymal disruption or acute tubular necrosis (renal), and downstream obstruction (postrenal). Inhibition of the RAAS with ARB/ACE-I may result in decreased renal blood flow and lower glomerular filtration, through efferent arteriole vasodilation. The cardiac surgery literature offers conflicting evidence on the risk of perioperative AKI and administration of RAAS inhibitors with some studies demonstrating decline in postoperative renal function, 14,15 another with no effect 16 and some with a protective effect against AKI. 17,18 Limited data exist on the effects of RAAS inhibition in patients undergoing noncardiac surgery, however, continuation of RAAS inhibitors in the perioperative period during orthopedic and bariatric surgery is associated with postoperative AKI. 10,11
In a recent study, Nyame et al. demonstrated that renin–angiotensin blockers were safe to continue immediately after partial nephrectomy as evidenced by no significant difference in postoperative GFR and a decreased risk of heart failure within 30 days of surgery. 12 Performing partial nephrectomy routinely necessitates temporary clamping of the renal artery during excision of renal masses, and, thus results in a theoretically greater renal ischemic insult compared with PCNL. As continuation of RAAS inhibitors in a partial nephrectomy cohort has been deemed safe, the same is likely true in a PCNL cohort.
Our study design was to assess the renal function impact of continuing or withdrawing RAAS inhibitors during the PCNL perioperative period. Our results indicate that among patients undergoing PCNL, there was no adverse effect of continuing RAAS inhibitors during the perioperative period on short and long-term renal function. Furthermore, continuation of RAAS inhibitors appeared to have, on average, no deleterious effect on blood pressure during inpatient recovery.
Studies of postoperative renal function after PCNL offer conflicting evidence. Agrawal et al. performed a study of 75 patients with severe chronic kidney disease and demonstrated improvement in average SCr following PCNL. 19 Jones et al. noted stable SCr and preservation of renal function following PCNL in 53 solitary kidneys. 20 Gorbachinsky et al. demonstrated that multiple access tracts are associated with a 2.28% decrease in renal function based on mercaptoacetyltriglycine nuclear renogram. 21 Handa et al. have utilized experimental animal models to demonstrate changes in renal function during PCNL. Their initial study concluded that PCNL destroys parenchymal tissue and unilateral PCNL results in an acute decline in renal filtration, perfusion, and excretory function bilaterally. 22 They also observed that needle puncture of the kidney for percutaneous access may be the driving force of renal vasoconstriction after PCNL, as evidenced by a decrease in effective renal plasma flow. 6 As renal function based on estimated glomerular filtration rate and creatinine can be impacted by patient factors such as baseline renal function, BMI, and ethnicity, a growing interest in more precise methods of renal functional assessment has taken place. The use of potential biomarkers for the early detection of AKI has been described by quantifying levels of kidney injury molecule-1, neutrophil gelatinase-associated lipocalin, N-acetyl-glucosaminidase, and liver-type fatty acid-binding protein levels after PCNL, with increased levels of the markers compared with normal controls. 23
Angiotensin II plays a role in maintaining circulating volume in response to stressors and volume depletion. The concern with anesthesia in patients continuing RAAS inhibitors include arterial hypotension following anesthesia induction secondary to uncompensated venous pooling of blood. 24 Withholding RAAS inhibitors may result in exaggerated pressure and heart responses to noxious stimuli and may result in increased risk of atrial fibrillation. 25 While our study demonstrated no significant differences in mean perioperative SBP between patients continuing or holding RAAS inhibitors, prior studies have demonstrated more frequent hypotension in patients who continue these drugs and undergoing noncardiac surgery. 26 The hypotension was more profound in patients requiring concurrent diuretic therapy, however, there was no increase in the incidence of more serious adverse outcomes, including myocardial infarction and postoperative renal dysfunction. Moreover, should postinduction hypotension present, generally, minimal pressor requirements and intravenous fluids are necessary to achieve normotension.
From a medication reconciliation standpoint, the potential of inadvertently prescribed drug discontinuation during the perioperative period warrants discussion. Medical errors, including unintended discontinuation of chronic medications, are common when transitioning from inpatient discharge to the outpatient setting. 8 With respect to ACE-I and ARBs in patients undergoing PCNL, our data support continuation of these drugs without a significant impact on perioperative renal function.
The strengths of our study include a large number of patients in our cohort. Medication administration was determined by examining the electronic medication administration record for accuracy. We obtained prolonged follow-up to 1 year postoperatively. A few limitations of this study warrant discussion. First, our cohort is derived from a single institution with charts retrospectively reviewed, which may not be representative of practices at other healthcare institutions. Second, our dataset did not include information as to why the anesthesia provider held or continued a RAAS inhibitor (i.e., history of hypertension, heart failure, chronic kidney disease, diabetes, proteinuria, etc.). It may be safe to omit the medication in certain circumstances and not safe for other indications. Our data compare changes in creatinine levels and GFR, which may not accurately represent true renal functional changes after PCNL. We did not have information on whether additional nephrotoxic medications, such as any nonsteroidal, were administered during a patient's postoperative hospitalization. It is possible that the administration of these other potentially nephrotoxic medications influenced the decision of whether to administer RAAS inhibitors. On average, the duration of action of most ACE-Is and ARBs is 24 hours (Lisinopril, benazepril, losartan) and for those patients asked to stop their medication on the morning of surgery, the drug likely had no significant effect during surgery and the postoperative period. However, the duration of action of some RAAS inhibitors approaches 36–48 hours (ramipril, telmisartan). Therefore, if patients were instructed to stop their RAAS inhibitor a day before their procedure, in theory some medications may still exert renal protective effects and alter some of the renal function data. We also did not include data on multiple tracts, intraoperative blood loss, and need for transfusion. Scenarios where these findings were present would indicate volume depletion and the effect of RAAS inhibitors may exaggerate renal function responses. Finally, despite matching patients, we were unable to completely control for selection bias. It is possible that those patients at highest risk for acute injury did not receive a RAAS inhibitor and this may have hidden the true detrimental effects of these medications. Our findings are hypothesis generating, and a more powerful scientific conclusion could be reached by conducting a prospective, blinded, randomized placebo-controlled trial of postoperative RAAS inhibitor use among this select group of patients undergoing PCNL. The addition of assessing biomarkers suggestive of renal injury or nuclear medicine imaging may also be of benefit.
Ultimately, the decision of whether to hold a patient's ACE-I or ARB during the post-PCNL recovery period necessitates an individualized approach. A partnership between urologists, anesthesiologists, and internists is required for safe and consistent outcomes, particularly for the patients with multiple medical comorbidities.
Conclusion
Our results indicate it is likely safe to continue RAAS inhibitors in patients undergoing PCNL during their operative hospitalization. Continuation of these medications resulted in relatively stable GFR in the short and long-term period, while avoiding significant blood pressure changes. Administering these medications during a patient's inpatient course may prevent errors in medication reconciliation at the time of hospital discharge.
Footnotes
Disclosure Statement
No competing financial interests exist.