
Abstract
Objectives:
To evaluate a recently reported new bioadhesive system for the retrieval of small residual fragments (RFs) after intracorporeal lithotripsy, we systematically compared this system with coagulum lithotomy in retrograde intrarenal surgery.
Materials and Methods:
We extracted 30 human stone fragments (≤1 mm) in an ex vivo porcine kidney model using a flexible ureteroscope for three groups: (1) the novel bioadhesive, (2) autologous blood as a natural adhesive, and (3) (control group) a conventional retrieval basket. Each group consisted of 15 test runs. Outcomes were evaluated regarding the macroscopic stone-free rate (SFR), retrieval time, and number of ureteral passages.
Results:
For groups 1 and 2, a significant advantage in stone clearance, mean retrieval time, and number of retrievals was detected compared to the control group (p = 0.001). The time and number of retrievals were significantly lower in group 1 (10:36 minutes, p = 0.001) than in group 2 (26:12 minutes, p = 0.001), with shorter clotting time and better visibility.
Conclusions:
These data show the general feasibility of intrarenal RF embedding to improve the SFR. Our data furthermore suggest the superiority of the artificial bioadhesive embedding agent over the application of native blood. Further in vivo studies and other research are necessary to confirm the adhesive's effect in patients.
Introduction
T
Interventions for the treatment of stones aim to achieve a high stone-free rate (SFR) in a single intervention. 3 However, residual fragments (RFs) may occur in a substantial number of patients, similar to after RIRS. 4 RF after RIRS, PNL, or shock wave lithotripsy has been shown to have an essential impact on the stone recurrence rate in several follow-up studies. 5 –7 Notably, there is still disagreement regarding the size definition and relevance of these “clinically insignificant residual fragments” after interventional stone treatment. 8 Considering the newest evidence, however, low-risk stone formers might have a tremendous benefit on complete stone clearance. 9
Therefore, novel approaches to RIRS such as coagulum lithotomy (also called the “glue clot technique” in endoscopy) have been developed to improve the SFR in patients with a large stone burden. 10 In coagulum lithotomy, autologous blood is applied over the scope's working channel to embed fragments that are too small or numerous for active retrieval. However, Cloutier and colleagues stated that this method has some important disadvantages; it requires an injection time of 5 minutes, followed by a waiting time of 5–10 minutes. Furthermore, the visibility is instantly impaired after the blood injection. Thus, the “glue clot technique” for RIRS has not been disseminated internationally, and it is not mentioned in current guidelines. 3
Based on the idea of internal embedding and retrieval of RF, we developed a bioadhesive system for endoscopic use. 11,12 The concept consists of two biocompatible fluids that are applied through a catheter system, which form a gel in the collection system and embed the stone fragments. Conventional graspers can be used to retrieve the gel–stone complex. The bioadhesive system's efficacy has been reported previously. 11
In this study, we compared the efficacy of endoscopic coagulum lithotomy 10 with RIRS, combined with the novel bioadhesive system, against conventional stone retrieval in a standardized setting. To obtain comparable results, the materials and methods were based on those of a previous study design. 11 Furthermore, to our knowledge, this is the first study that evaluates the efficacy of coagulum lithotomy in endoscopy in a comparative test trial.
Materials and Methods
Experimental setting
All experiments were performed in an ex vivo porcine kidney model, as described previously.
11
One kidney (for each test) of a female domestic pig was placed at the bottom of a 33 cm × 68 cm × 11 cm plastic basin and fixated using a retractor ring (Lone Star® Retractor System 3304G; Cooper Surgical, Trumbull, CT), which was attached to the plastic basin (Supplementary Fig. S1; Supplementary Data are available online at
Termination of trial run after 45 minutes due to impossibility to extract the targeted fragments.
Our study protocol (including the use of human urinary stones and human blood samples) was approved by our local ethics committee. All experiments were conducted according to the ethical standards determined by the Declaration of Helsinki 1964 and its later additions.
Embedding techniques
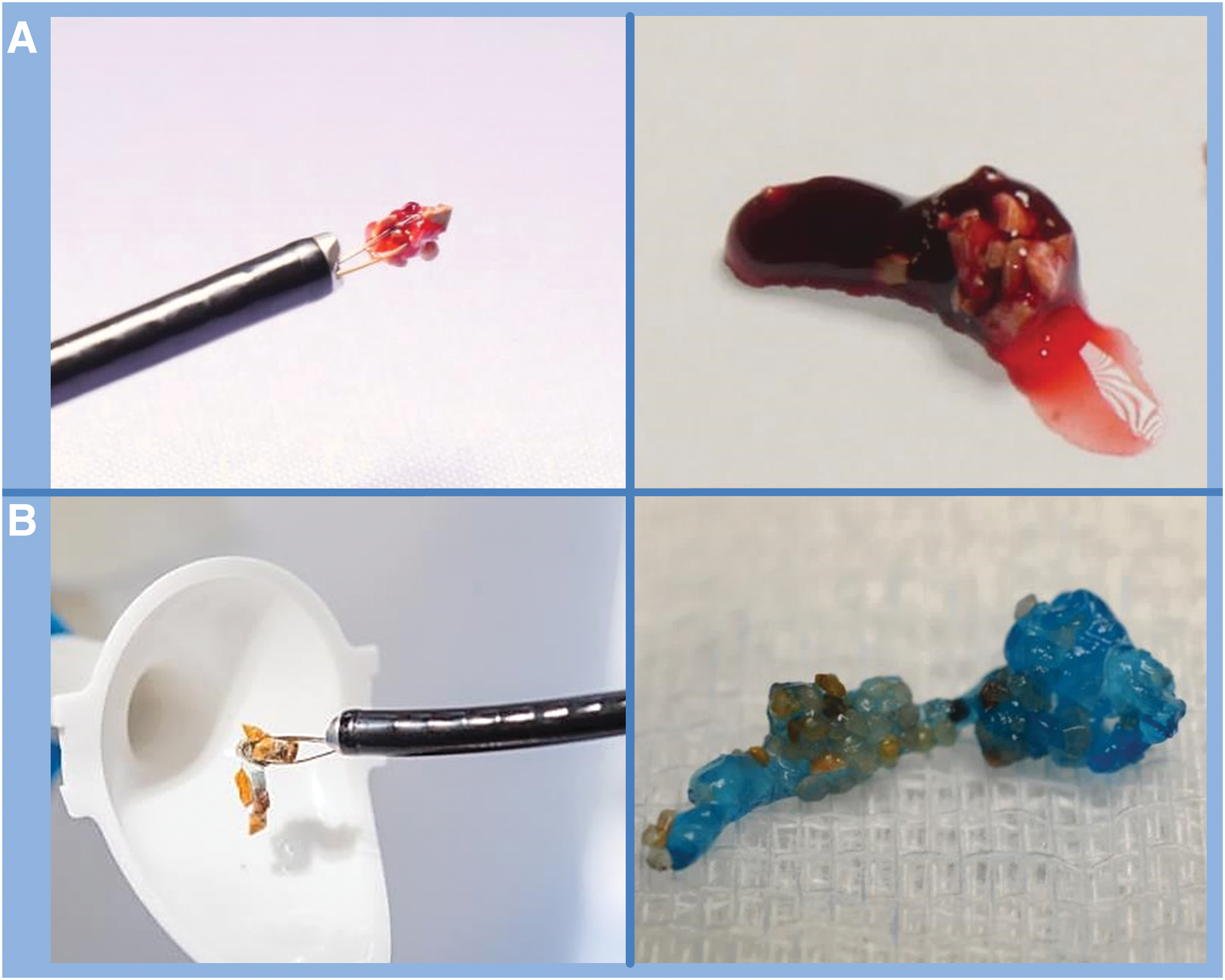
To evaluate the value of different embedding techniques, we performed 45 trial runs. For 15 kidneys (group 1), we used a novel, polysaccharide-based, two-component bioadhesive system. 11 The first component was applied using a thin FLEXguard® catheter with a 3F outer and 2F inner diameter. The catheter was introduced to the renal pelvis through the scope's working channel and placed close to the stone fragments. Component 1 was applied in liquid form around the calices and its volume was determined based on local distribution of the stone fragment. To better visualize component 1, we dyed it blue. Afterward, component 2 was administered in a predefined 20 mL volume over the scope's working channel. The combined components substrated and created an adhesive lump that incorporated the stone fragments.
For the second set of 15 kidneys (group 2), blood was used as a natural adhesive agent, as reported by Cloutier and colleagues 10 All blood samples were obtained from human probands. The international normalized ratio and bleeding time (Ivy method) of the used blood samples were in the normal range. A blood sample of 10 mL was applied through the scope's working channel and the working channel's outlet was placed near the stone fragments. Before beginning this study, we performed a prestudy that confirmed adequate clotting of human blood in a porcine kidney and determined the optimum volume of blood. According to Cloutier and colleagues, stones were not retrieved until after a 10-minute waiting period to ensure sufficient clotting. 10 For both adhesive techniques, saline irrigation was ceased during the application of the respective embedding agent, as well as during the clotting period.
In the control group (group 3), stones were retrieved from 15 porcine kidneys using a commercial grasping device.
Stone and clot extraction
All trial runs were performed using a flexible ureteroscope (Cobra Vision®; Richard Wolf, Knittlingen, Germany) and an NGage® (Cook Medical) open-tip basket for extraction. Constant saline irrigation was applied as is usual for ureteroscopic procedures. A single experienced surgeon who initially evaluated the biocompatible adhesive in our previous study performed all trials. 11 Sufficient breaks between completed procedures were taken to ensure that the test results were not influenced by fatigue. The bioadhesive lumps were retrieved until no blue-dyed remains were detected endoscopically in the targeted kidney; similarly, blood clots were removed and irrigation was performed until no blood clots remained. Stone fragments were simply grabbed with the basket and retrieved.
Endpoints
SFR was evaluated endoscopically and macroscopically by organ autopsy; the kidneys were classified as “stone free” or “not stone free.” Time was recorded at catheter insertion (group 1), blood application (group 2), or insertion of the extraction basket (group 3). The time was stopped until the surgeon endoscopically rendered the kidney “stone” or “lump/clot” free, or after 45 minutes.
Statistical evaluation
Endpoints were evaluated using Wilcoxon's rank-sum testa (baseline comparison of weight of probes, and comparison of all nonparametric endpoints) and Fishers’ exact testb (binary parameters). See also Results section below. All statistical computations were performed using IBM SPSS Statistics (IBM SPSS Statistics for Windows, Version 23.0; IBM Corp., Armonk, NY). The test used in each case is indicated by superscript letters. p Values <0.05 were considered to be significant.
Results
We achieved endoscopically and macroscopically complete stone clearance in 100% of kidneys in groups 1 and 2, and 60% of kidneys in the control group. The results of trial runs 1 through 15 and 31 through 45 have been reported previously. 11 There was a significantly higher rate of complete stone clearance in the trial runs using the biocompatible adhesive compared with our control group (p = 0.17b). The overall mean weight of the stone probes was 0.032 g, and a significant difference in stone weight between the different groups was not present (Table 1 a).
The retrieval time of the biocompatible adhesive group was significantly faster compared with the control group (average: 10 minutes 30 seconds; mean = 36:56 minutes; p = 0.001a), and significantly faster than the group using blood (mean = 26:12 minutes; p = 0.001a). The blood group also showed a significantly faster retrieval time than the control group (p = 0.003a), although achieving a 100% “stone-free” rate. When adding the waiting time of 10 minutes until sufficient blood coagulation was achieved, however, the time benefit disappeared.
The average number of retrieval attempts ranged between 3 and 30, with an average of 8.46 tries in the bioadhesive group compared to an average of 22.30 in the blood group and 27.13 in the control group. Therefore, there was a significantly lower number of attempts in the bioadhesive group compared to both other groups (p = 0.001a). The number of retrievals in the blood group was significantly lower than that in the group without an adhesive (p = 0.004a).
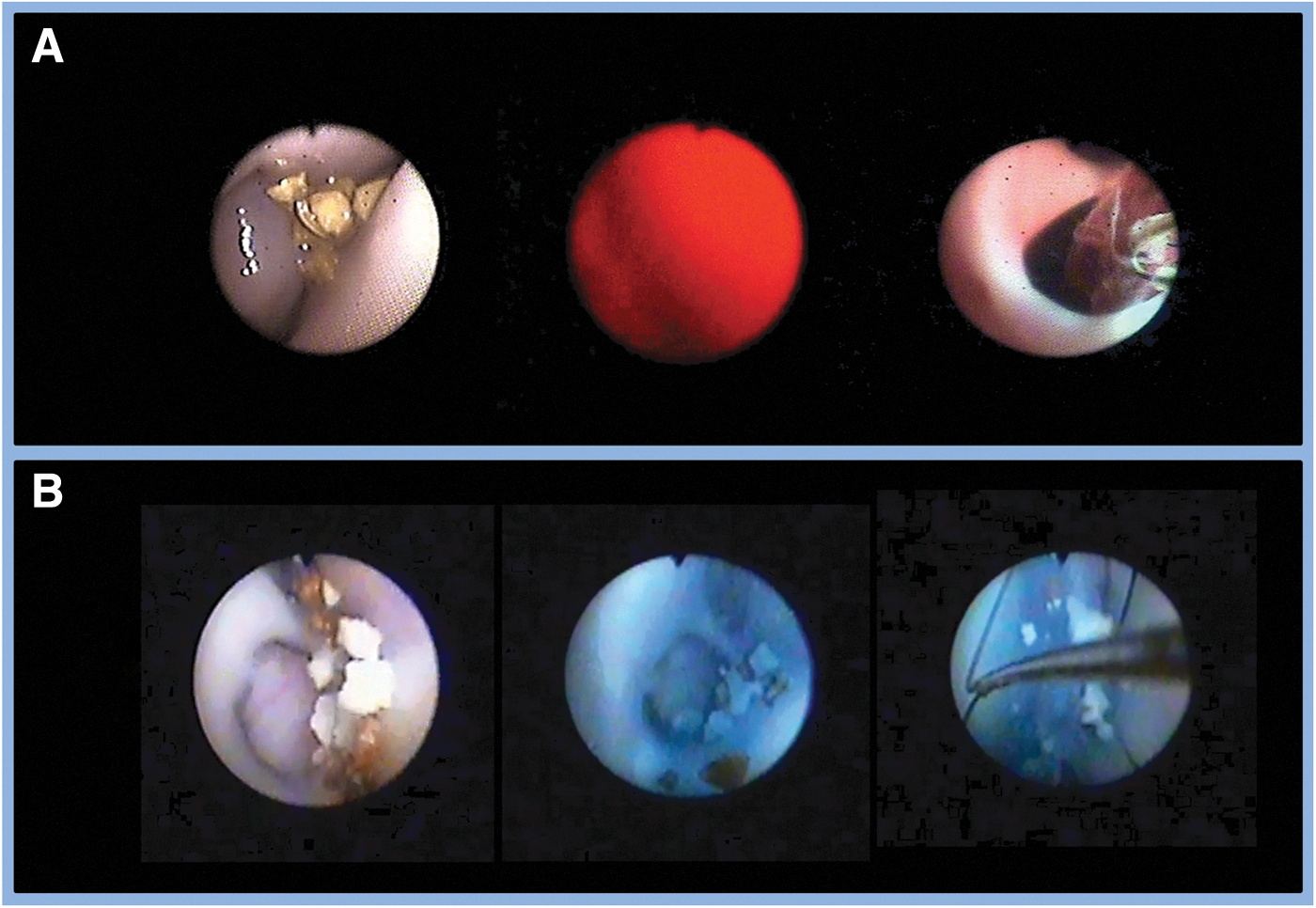
Application of the biocompatible adhesive system was feasible and endoluminal lumps were well detected (Fig. 2). In addition, the lump formation and the fragments that were embedded within it were easily visible (Fig. 1). No significant adhesions to tissue, graspers, and access sheaths were reported.
In group 3, retrieval of small and very small stone fragments was strenuous, and in some cases, the stones were impossible to retrieve.
In group 2, human blood was a potent embedding agent (Fig. 1). However, visibility was poor and it was impossible to observe clot formation and embedded fragments (Fig. 2). Clot extraction was feasible; however, continuous irrigation was necessary to achieve satisfactory visibility. Upon complete clot retrieval, visibility remained severely impaired. Therefore, complete clot evacuation was crucial to ensure stone clearance; adhesion to tissue was present, but it was surmountable with targeted irrigation and mechanical manipulation in all cases.
Discussion
In this study, we used an ex vivo porcine kidney model to systematically evaluate two different embedding techniques compared with the standard approach, using a commercially available grasper. Our results demonstrated that the application of an embedding agent to evacuate small RFs seems to be feasible to achieve an excellent SFR. In our study, we reached total stone clearance in 100% of cases when using the adhesive, showing that it has a clear advantage over the conventional method of collecting single fragments using an extraction device alone.
Considering the current trends in urolithiasis therapy, new techniques must be developed to overcome challenges such as RFs after RIRS or prolonged operation times due to high stone burden. An important step toward this goal has already been made with the recent development of new laser systems and miniaturized scopes. 13 However, suitable retrieval methods to endoscopically evacuate small RFs after lithotripsy remain unavailable, and the retrieval of these fragments is often difficult. This might result in negatively impaired SFRs, complications, and long operation times. To solve this problem, different approaches have been discussed. Based on a technique called coagulum lithotomy, which is used during open pyelolithotomy, 14 stone embedding agents seem to be a promising approach to address this issue. Similar to “coagulum”-based fragment retrieval methods, a modified strategy for the use of embedding agents in RIRS was reported in various studies. 10,15,16 However, due to a delay in operation time caused by the time necessary to achieve clotting as well as impaired visibility due to injected blood, this promising technique has not been disseminated.
In a recent study, 11 we presented a new artificial bioadhesive for the intraoperative embedding of small kidney stone fragments to achieve a high SFR. This new agent aimed to achieve superiority over the previously described glue clot techniques using autologous blood 16,10 and solve the shortcomings of the glue clot technique.
In this study, in terms of efficiency, both adhesive agents showed superiority over the control group in the number of ureteral passages and operation time needed. The time advantage in group 1 (human blood) has yet to be critically seen since the waiting time of 10 minutes must be added to the total surgery time. Adding this time would not only diminish the time benefit in our study to a point of no significance but also consume it entirely, making the procedure on average as long as that of procedures that do not use an adhesive agent. Although this could be accepted to reach full stone clearance, the disadvantage is more severe in cases in which multiple applications of adhesive are necessary, for example, those with a high stone burden. Since repeated application of autologous blood as a coagulant is only feasible once the previous clots have been completely evacuated, to regain full visibility, the additional waiting time would significantly elongate the procedure, making a risk-benefit assessment unfavorable for blood-based embedding. In this context, the artificial bioadhesive shows a clear benefit over both groups, not only in terms of significantly faster evacuation time but also in the short waiting time before extraction. Since the artificial adhesive does not negatively influence visibility, repeated application is feasible, and a parallel application to stone deposits in various calices is possible. Inadvertently embedded larger stone fragments do not hamper Holmium laser lithotripsy. Another advantage was also noticed in terms of the number of necessary ureteral passages. The bioadhesive group had significantly fewer passages than the blood and control groups. Although the blood group required fewer passages than the control group, a high number was still required. This may be due to the necessity of evacuating not only one clot with embedded stones but also multiple clots formed by the injection of 10 mL of blood, which led to a higher number of passages. To reduce this number, we discussed leaving blood clots partly in situ, since small clots would not significantly impair the patient outcomes. However, we dismissed this approach for two reasons: first, detection of stones within the glue clot is endoscopically not possible with sufficient sensitivity, and second, the visibility necessary to endoscopically determine a “stone-free” kidney is only available after all clots have been evacuated. These data suggest that the bioadhesive used in this study has a clear advantage in terms of practicality and efficiency.
However, the study has specific limitations due to the experimental setup. First, the surgeon was not blinded when performing the experiments; this was not possible due to the study design. Furthermore, the anatomy of a porcine kidney is partially different from that of the human kidney. We evaluated only one grasping device, and a potential increase of the surgeon's routine while performing the trial runs must be considered. Requirements regarding the biocompatibility of the adhesive are not addressed in this study. First, in vitro tests using urothelium cell lines proofed biocompatibility. However, as the biocompatibility has to be proven in vivo, we are planning further studies on this issue. Therefore, an in vivo animal study is intended in which the adhesive system is left behind purposely in the collecting system of domestic pigs. Also, all test runs were performed in ex vivo porcine kidneys with no interaction with blood and urine. Therefore, new in vivo animal trials and patient studies are required to address these issues. After the adhesive has been approved for clinical use, several important points have to be addressed in first clinical studies. Herein, the efficiency of the adhesive system should be proved, and adverse events like renal colic due to possible residual adhesive lumps and the need of routine ureteral stenting after application of the adhesive system have to be assessed.
Conclusions
This study shows the feasibility of different kidney stone embedding techniques in endoscopy and addresses the issue of complete stone clearance after intracorporeal lithotripsy. Our results in an ex vivo porcine kidney model furthermore suggest the superiority of an artificial bioadhesive as an embedding agent over the application of autologous blood due to a significantly lower operation time and a decreased number of necessary ureteral passages. In addition, the artificial bioadhesive showed good practicability for intraoperative application. Correlation of these findings to the use in humans is still unknown and needs further clarification in studies.
Footnotes
Acknowledgments
The study was supported by research grant from the Germany Ministry of Education and Research BMBF (031A387) and own institutional funding. IRB approved protocol number: 296/15 leading ethics committee (Ethik-Kommission der Albert-Ludwigs-Universität Freiburg, Germany). German Clinical Trial Register ID: DRKS00010243 (approved WHO primary register).
Authors’ Contribution
D.S.S., protocol/project development, assisted surgery in ex vivo model, data collection and management, data analysis, and article and figure writing/editing. M.S., data analysis, article editing, and assisted surgery. D.S., article editing and assisted surgery. R.P., article editing and assisted surgery. M.B., article editing, assisted surgery. K.R., protocol/project development and developed chemical composition. I.G., protocol/project development and developed chemical composition. U.W., data analysis and supervision. A.M., protocol/project development and article and figure writing/editing, supervision. S.H., protocol/project development, article and figure writing/editing, supervision, and performed surgery in ex vivo model.
Ethical Approval
The study was approved by our local ethics committee and was therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave their informed consent to provide stone material prior to their inclusion in the study. Number 296/15, Ethics Committee of the University Medical Center Freiburg.
Author Disclosure Statement
M.S., consultant contract with Schoelly GmbH, Denzlingen, Germany, and NeoTract, Inc., Pleasanton, USA (both unrelated to this work). U.W., advisory board, Dr. Kade Pharmazeutische Fabrik GmbH, Berlin, Germany (unrelated to this work). A.M., consultant contract with Schoelly GmbH, Denzlingen, Germany (unrelated to this work). In addition, M.S., A.M., I.G., and K.R. hold the patents AU002013387207A1, CA000002910164A1, CN000105283140A, EP000002988682A1, EP000002796101B1, EP000002796101A1, KR102016004322A, US020160074561A1, and WO002014173468A1, all issued to the Albert Ludwig University of Freiburg and the Fraunhofer Society for the Advancement of Applied Research and covering the technology of the novel bioadhesive system reported in this study. None of the other authors has any conflict of interest or financial ties to disclose.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.