
Abstract
Introduction and Objective:
With the peritoneum acting as a natural surface for lymphatic reabsorption, transperitoneal robot-assisted radical prostatectomy (tRARP) is thought to be associated with a lower incidence of symptomatic lymphoceles (SLs) compared with its extraperitoneal counterpart (eRARP) when bilateral pelvic lymph node dissection (BPLND) is performed. In this study, we aim to determine if there is a difference in SL formation and characteristics between the two approaches.
Materials and Methods:
We retrospectively reviewed the records of patients who underwent eRARP or tRARP and BPLND by a single surgeon at a tertiary care academic center from July 1, 2003, to May 31, 2016. Patients with a history of prior pelvic radiotherapy, concomitant inguinal hernia repair, RARP without BPLND, or nonadenocarcinoma of the prostate were excluded. The resulting eRARP and tRARP groups were propensity matched for age, body mass index (BMI), American Association of Anesthesiologists (ASA) score, D'Amico risk classification, and pathological lymph node (LN) count.
Results:
A total of 3183 RARPs were performed during this time period. After applying exclusion criteria and propensity score matching, 671 patients remained in each group. No statistically significant differences were noted between the groups with regard to age, BMI, ASA, pre-RARP prostate-specific antigen, D'Amico risk classification, biopsy and pathological Gleason sum score, pathological T stage, or margin status. The tRARP group had a higher clinical T stage (p = 0.0015), length of stay (LOS; p = 0.005), pathological N stage (4.92% vs 1.36%, p = 0.0002), and high total LN count (7.22 ± 5.54 vs 5.78 ± 4.18 LNs, p < 0.0001). The eRARP group had higher operating room times (197.4 ± 48.96 minutes vs 192.2 ± 44.12 minutes, p = 0.04) and estimated blood loss (218.4 ± 152.0 mL vs 179.9 ± 119.4 mL, p < 0.0001). No differences were noted in the frequency of SL formation [eRARP: 19/671 (2.83%) vs tRARP: 10/671 (1.49%), p = 0.09] or any clinical characteristics of the SL. Logistic regression analysis showed no effect of LN count (p = 0.071), pathological N stage (p = 0.111), or both combined (p = 0.085) on SL formation.
Conclusions:
In this cohort, the rate and clinical characteristics of SL were similar among patients treated with eRARP or tRARP and BPLND. The low event rate of SL in each group and trends favoring higher SL with LN yield and pN1 disease in the tRAPR group may deem the study underpowered to make definitive conclusions.
Introduction
T
In contrast, the goal of eRARP is complete avoidance of the peritoneal cavity by performing the entire procedure in the space of Retzius. Potential advantages of eRARP include the avoidance of adhesiolysis in patients with prior abdominal surgeries, decreased postoperative ileus, decreased risk of visceral injuries, and averting the formation of new intraperitoneal adhesions.
tRARP also has several advantages, including a larger working space, greater ease of performing pelvic lymph node dissection (PLND), less operative time required for port placement, and perceived lower risk of epigastric artery injury. Thus, it has become the more commonly used approach by North American trained urologists. With the peritoneum acting as a natural surface for lymphatic reabsorption, many surgeons believe that tRARP may have a lower incidence of lymphocele formation.
To lessen the risk of lymphoceles, surgeons who are familiar with both eRARP and tRARP techniques may preferentially opt for the latter when bilateral pelvic lymph node dissection (BPLND) is also performed. Given that there has been a recent stage migration of prostate cancer, 1,2 possibly resulting from the recognition of overdiagnosis and overtreatment of low-risk disease, 3,4 increased enthusiasm for active surveillance in low-risk disease, 5 and novel biomarkers and imaging modalities, 6 –8 this may, in turn, further decrease enthusiasm for the performance of eRARP over tRARP.
Despite these claims, no group has directly compared the rate and clinical characteristics of symptomatic lymphocele (SL) formation after BLND in patients who have undergone tRARP or eRARP. In this study, we compare the incidence of this complication among patients who have undergone both procedures in a large, prospectively maintained surgical cohort. Patient and disease characteristics were recorded as was information related to the clinical characteristics and treatments of the SL.
Materials and Methods
Subjects having undergone RARP at the University of Rochester Medical Center by a single surgeon (J.V.J.) from July 1, 2003, through May 31, 2016, were identified from the Department of Urology quality assurance database. Institutional Research Subjects Review Board approval was obtained before initiation of data collection or analysis.
Among this group, data were collected on men who underwent BPLND. Men who had prior pelvic radiotherapy, nonadenocarcinoma prostate cancer, or concomitant inguinal hernia repair were excluded. Biopsies performed at institutions outside were reviewed internally by a team of pathologists at our institution. Patients were divided into two cohorts based on whether they had received eRARP or tRARP. The resulting groups were propensity matched as already described.
As a formal part of every post-RARP follow-up visit, a summary form is completed, documenting whether the patient had any post-RARP complications, adverse functional outcomes, diagnostic imaging studies, or postoperative adjuvant treatments. For these patients who are seen in a follow-up clinic, a dedicated departmental information analyst reviews all clinical visit forms in concert with progress notes, emergency department visits at our institution, documented patient telephone encounters, and scanned documents received from consulting physicians or those who have accepted transfer of care.
Clinical parameters and perioperative characteristics were compared between the groups. The rate of SL formation and clinical characteristics related to each SL were also collected. For the purposes of this study, SL was defined as a pelvic fluid collection identifiable by medical imaging, at least 3 cm in maximal diameter, and located adjacent to the site of the PLND. It must have been diagnosed during work-up for post-RARP pelvic pain or pressure, urinary retention, weakness/malaise, high drain output, leg edema/pain/weakness, or infection in patients who underwent PLND.
Asymptomatic lymphoceles were not recorded. Imaging studies were only performed postoperatively when clinically indicated, as already noted. Hospital charts and imaging studies of patients coded as having post-RARP lymphoceles, abscesses, pelvic fluid collections, infected hematomas, or infected seromas were reviewed to determine if these were SLs. Maximal axial area of SL was calculated from CT scan information in the anteroposterior axis using the formula for the area of an ellipse: Aellipse = πab, where a and b are the lengths of the semimajor and semiminor axes, respectively. For cases of patients with multiple lymphoceles, data related to size and treatment thereof were only recorded for the largest.
Surgical technique
Trocar access during tRARP begins with abdominal insufflation using a Veress needle and all trocars are placed under direct vision. A 12-mm assistant trocar is placed 8–10 cm cephalad to the right anterior superior iliac spine. An 8-mm camera trocar is placed just below the umbilicus and three other 8-mm working trocars are placed in a W configuration, with care taken to avoid injury to the inferior epigastric vessels. An additional 5-mm assistant trocar is placed 4 cm lateral and cephalad to the camera trocar. Our technique for obtaining access during eRARP has been previously published. 9
In general, indications for performing PLND were a risk of LN metastases >1% by the Memorial Sloan Kettering Prostate Cancer Risk Nomogram. The anatomical template used to perform PLND for patients in both groups comprised the external iliac artery (laterally), the superficial circumflex vein (caudally), the node packet posterior to the obturator nerve (deep), and bifurcation of the common iliac artery (cephalad). All visible lymphatic tributaries were secured with Hem-o-lok® clips (Teleflex Medical, Research Triangle Park, NC). All patients received subcutaneous heparin pre- and postoperatively. This was administered to the lower abdomen, posterior aspect of arm, or anterior thigh, as dictated by patient preference.
Statistical analyses
Patients were propensity score matched 1:1 using logistic regression. The dependent variable was surgical technique (tRARP or eRARP) and independent variables were age, body mass index (BMI), American Association of Anesthesiologists (ASA) score, D'Amico risk classification, and total number of lymph nodes (LNs) removed. For all continuous variables, the two-sample t-test was used to compare differences between groups. For categorical variables, Pearson's chi-square test or Fisher's exact tests were used as appropriate. Logistic regression analysis was performed to determine if the rate of SL formation would change if LN count, the presence of pN1 disease, or both variables in combination were controlled for. All tests were two-sided, with p ≤ 0.05 considered statistically significant. Statistical analyses were implemented with SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
A total of 3183 men underwent RARP for localized prostate cancer during the aforementioned time period. Patients were excluded for the following reasons: prior pelvic radiotherapy, 10 nonadenocarcinoma of the prostate, 4 concomitant inguinal hernia repair during RARP (50), no PLND performed (1083), and unilateral PLND performed during RARP (38). Patients were then divided into two groups based upon whether they underwent eRARP (n = 671) or tRARP (n = 1326). After propensity matching, both groups consisted of 671 patients (Fig. 1).
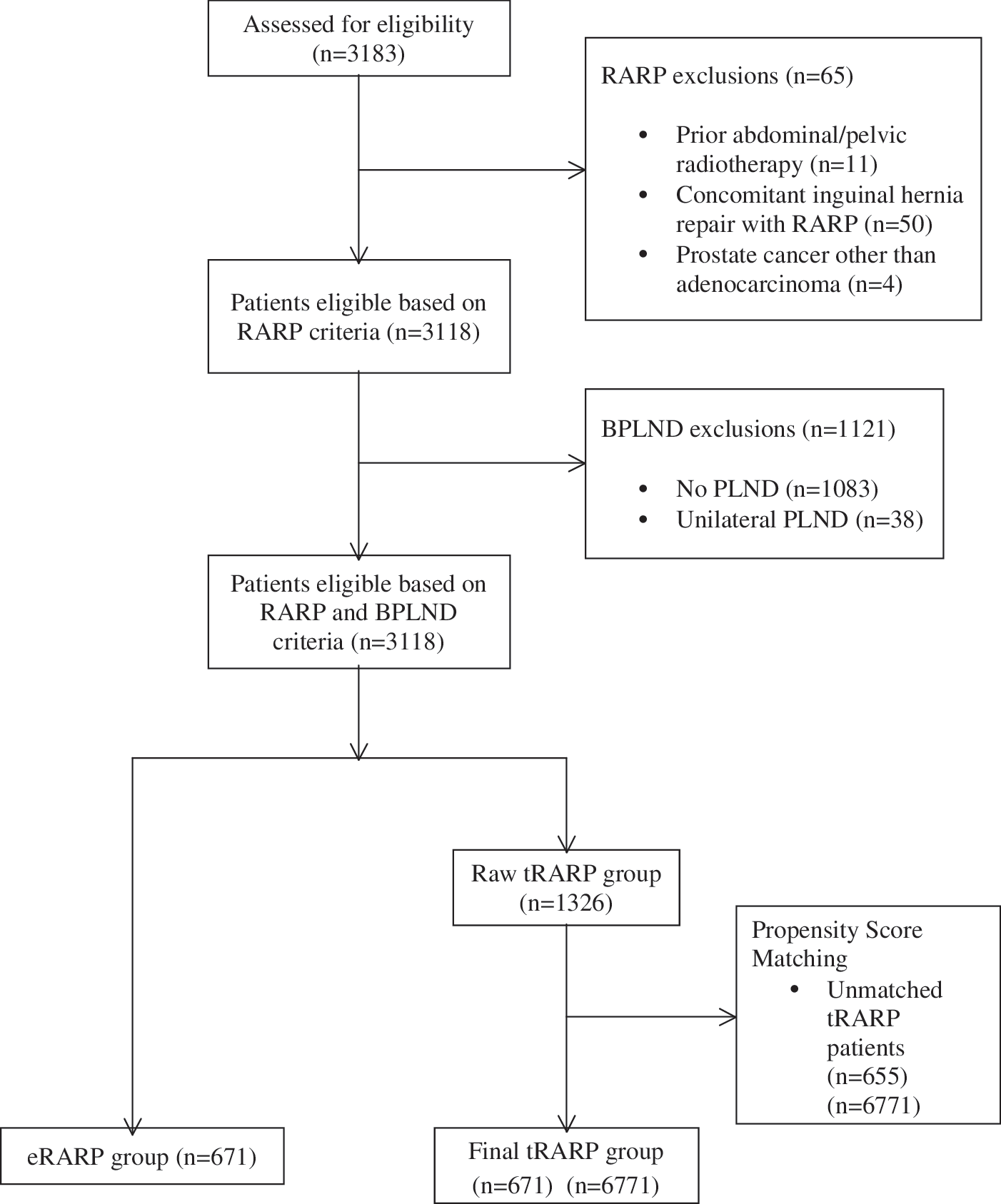
Flow diagram of patients participating in the study. BPLND = bilateral pelvic lymph node dissection; eRARP = extraperitoneal RARP; PLND = pelvic lymph node dissection; RARP = robot-assisted radical prostatectomy; tRARP = transperitoneal RARP.
Operative cases in this series performed from 2003 to 2007 were predominately eRARP and from 2010 to 2016 were mainly tRARP. The period from 2008 to 2009 was a transition period where the two approaches were used relatively interchangeably. Whether a patient underwent eRARP or tRARP was at the discretion of the surgeon.
Patient and disease characteristics are shown in Table 1. No statistically significant differences were noted between the groups with regard to age, BMI, ASA score, pre-RARP prostate-specific antigen (PSA), biopsy Gleason sum score, or D'Amico risk classification. Patients in the tRARP group had higher clinical T stage compared with those in the eRARP group (p = 0.0015).
Continuous measurements: Age, BMI, pre-RARP PSA. Categorical variables: ASA score, Biopsy Gleason sum, Clinical T stage, D'Amico risk.
ASA = American Association of Anesthesiologists; BMI = body mass index; eRARP = extraperitoneal RARP; RARP = robot-assisted radical prostatectomy; SD = standard deviation; tRARP = transperitoneal RARP.
Surgical and pathological data are shown in Table 2. The eRARP group had a longer operating room (OR) time (197.4 ± 48.96 minutes vs 192.2 ± 44.12 minutes, p = 0.04), higher estimated blood loss (EBL; 218.4 ± 152.0 mL vs 179.9 ± 119.4 mL, p < 0.0001), and shorter length of hospital stay (LOS; p = 0.005). Pathological Gleason sum score, pathological T stage, and margin status were similar between the groups. The tRARP group had a higher incidence of pN1 disease (p = 0.0002) and more total LNs removed per BPLND (7.22 ± 5.54 vs 5.78 ± 4.18 LNs, p < 0.0001). No differences were noted in the rate of SL formation between the groups [eRARP 19/671 (2.83%) vs tRARP 10/671 (1.49%), p = 0.09]. Of 655 patients who were dropped from the study after propensity score matching, 13 developed SLs (1.98%). No differences were noted in the rate of SL formation between this group and the eRARP group (p = 0.41) or the tRARP group (p = 0.63).
Continuous measurements: OR time, EBL, total LNs removed. Categorical variables: LOS, path. Gleason sum, Path. T stage, Path. N stage, margin status, presence of SLs.
EBL = estimated blood loss; LN = lymph node; LOS = length of hospital stay; OR = operating room; SL = symptomatic lymphocele.
Tables 3 –5 present a logistic regression analysis to determine if controlling for total LN count alone, pathological N stage alone, or both variables in combination would change the rate of SL formation. When controlling for total LN count through this method, a trend was noted favoring a higher rate of SL formation in the eRARP group, but this difference was not statistically significant (Table 3; p = 0.071). Controlling for pN1 disease showed a similar trend (Table 4; p = 0.111) as did controlling for both variables together (Table 5; p = 0.085), but these too were not statistically significant.
Table 6 outlines the characteristics of the SLs themselves. No differences were noted in the time from RARP to diagnosis of SL, presenting symptoms or laterality. All SLs were diagnosed by CT (i.e., none by ultrasound, MRI, or other imaging studies). No significant differences were noted in the size of the SL, hospital admission rates for SLs, or LOS if the patient was admitted to hospital. Treatments of the SL were similar between the groups. None of the patients in this series required formal surgical drainage (with or without peritoneal window) of their SL. When a percutaneous drain was placed, drain removal time and use of sclerosing agents were similar.
JP = Jackson-Pratt; NYD = not yet diagnosed.
Discussion
SLs can be associated with significant morbidity. The absorptive peritoneal surface is thought to decrease the risk of lymphocele formation following lymphadenectomy and has led to several technical modifications to RARP in an attempt to reduce its incidence. 10,11 In this study, we compared the rate and clinical characteristics of SLs in a large group of patients undergoing eRARP or tRARP who were propensity score matched for six key preselected patient and disease-related covariates.
The incidence of lymphocele formation following RARP and PLND is variable. A recent systematic review reported a rate of SLs ranging from 0% to 8%, with a node count ranging from 3 to 24. 12 Orvieto and colleagues found a 51% incidence of lymphoceles when all patients underwent a postoperative CT scan and a 15.4% incidence of SLs at a mean follow-up of 10.8 weeks. No surgical clips were used to control lymphatic channels during node dissection. 13 Lee and colleagues found a 20.5% (41/200) incidence of lymphoceles in patients after eRARP when all patients (symptomatic and asymptomatic) underwent postoperative CT or MRI. 14
While several groups have compared outcomes of eRARP with tRARP, they generally calculate complications as a group and not individually, some making no mention of lymphocele formation. In studies reporting on lymphoceles, it is often difficult to determine whether they were SLs. Furthermore, studies comprising an eRARP cohort have been much smaller than ours. Horstmann's group compared eRARP and tRARP with only 103 and 67 patients in each group, respectively. 15
Stolzenburg published a large series of patients who underwent eRARP and found the rate of SLs to be 3.8%. It is unclear how many of these patients underwent PLND and these patients were not compared with another group undergoing tRARP. 16 Mundhenk and colleagues compared a group of patients who underwent tRARP with another group that underwent open radical prostatectomy and found a higher incidence in the latter group (8.0% vs 0.8%). 17 A meta-analysis was performed comparing outcomes of eRARP and tRARP, but this included only one randomized control and five case–control studies (comprising 842 patients), and complications were only noted by their Clavien-Dindo grade, therefore no conclusions about SLs could be drawn. 18
The current article is a retrospective cohort study and is thus subject to selection bias. In our database, patients who underwent eRARP generally had lower-risk disease compared with those who underwent tRARP. 19,20 One possible explanation is that the majority of eRARPs were performed earlier in the series when patients, in general, presented with lower-risk disease. Second, there has been a shift at our institution in recent years to only perform eRARP in patients with a low risk of nodal metastasis due to concern that PLND with eRARP may be associated with a higher rate of SLs. The selection biases in techniques chosen in different eras are evident as one of the limitations of such retrospective analyses.
In an attempt to mitigate some of these discrepancies, the two groups were propensity score matched. After its application, pre-RARP PSA, biopsy Gleason sum, and D'Amico risk classification were similar, whereas clinical T stage and pN1 disease remained higher in the tRARP group.
The PLND templates were theoretically the same for eRARP or tRARP, but in practice, PLND during eRARP seems to be more challenging due to limitations imposed by the peritoneal surface with the cephalad aspect of the dissection. Thus, a lower LN yield was noted in the eRARP group, even after attempting to control for this through propensity score matching. The LN count may also be affected by specimen assembly (multiple samples vs one packet) and intraobserver variability in counting; over the course of the study, many different pathologists were involved in specimen assessment and reporting (>20).
Whether the number of LNs removed during PLND or the presence of pN1 disease has an effect on lymphocele formation is a matter of debate. 13,14,21,22 We used logistic regression modeling to determine if these covariates (either alone or in combination) could have affected the rate of SLs between our groups, and our models showed no clear association. Thus, more confidence can be placed on the comparison made between these two groups, which differed in the rate of these two covariates. It is possible that with such small numbers, logistical regression modeling analyses might not compensate sufficiently in this regard.
OR time and EBL were both higher in the eRARP group, which is likely a by-product of these procedures being performed earlier in the series, or impacted by the surgeon's learning curve. Creation of the extraperitoneal space and trocar placement require more time when compared with the transperitoneal technique. LOS was shorter in the eRARP group and this is consistent with other studies published by our group and others. 20,23,24 This may be due to fewer gastrointestinal (GI) complications (ileus, Ogilvie's, etc.) stemming from lack of bowel manipulation and adhesiolysis during eRARP. 20
As noted in Table 6, no differences were demonstrated in any of the clinical characteristics or treatments of SLs themselves. Our study is the first to compare these types of data between the two approaches. Despite this, our sample size for this complication (n = 29) is quite small and may lack the statistical power to detect significant differences. Furthermore, patients who did not follow-up at our institution may have had SLs that were unaccounted for, thus affecting our observed SL rates.
Conclusions
Our review showed no statistically significant difference in the rate of SL formation between the eRARP and tRARP groups after propensity score matching and controlling for LN count and pN1 disease through logistic regression. The clinical features of the SLs themselves were also similar. A transperitoneal approach does not seem to protect from the development of SLs, as previously thought.
Footnotes
Acknowledgments
The authors would like to thank Ingrid Mikk, Bonita Powell, and Mary Kay Winchell.
Author Disclosure Statement
No competing financial interests exist.