
Abstract
Purpose:
In the first-in-human trial of ultrasonic propulsion, subjects passed collections of residual stone fragments repositioned with a C5-2 probe. Here, effectiveness and safety in moving multiple fragments are compared between the C5-2 and a custom (SC-50) probe that produces a longer focal beam and burst duration.
Materials and Methods:
Effectiveness was quantified by the number of stones expelled from a calyx phantom consisting of a 30-mm deep, water-filled well in a block of tissue mimicking material. Each probe was positioned below the phantom to move stones against gravity. Single propulsion bursts of 50 ms or 3 s duration were applied to three separate targets: 10 fragments of 2 different sizes (1–2 and 2–3 mm) and a single 4 × 7 mm human stone. Safety studies consisted of porcine kidneys exposed to an extreme dose of 10-minute burst duration, including a 7-day survival study and acute studies with surgically implanted stones.
Results:
Although successful in the clinical trial, the shorter focal beam and maximum 50 ms burst duration of the C5-2 probe moved stones, but did not expel any stones from the phantom's 30-mm deep calyx. The results were similar with the SC-50 probe under the same 50 ms burst duration. Longer (3 s) bursts available with the SC-50 probe expelled all stones at both 4.5 and 9.5 cm “skin-to-stone” depths with lower probe heating compared to the C5-2. No abnormal behavior, urine chemistry, serum chemistry, or histological findings were observed within the kidney or surrounding tissues for the 10 min burst duration used in the animal studies.
Conclusions:
A longer focal beam and burst duration improved expulsion of a stone and multiple stone fragments from a phantom over a broad range of clinically relevant penetration depths and did not cause kidney injury in animal studies.
Introduction
U
In a first-in-human trial of ultrasonic propulsion, stones were moved in 14 of 15 subjects using a commercial C5-2 probe. 2 The most promising results came from the six postlithotripsy cases. Four subjects reported passing an aggregate of over 30 stone fragments. Observations made during the trial suggested better efficiency in clearing fragments could be achieved with a different probe. The burst duration and required wait time between bursts for the C5-2 was limited by probe surface heating. In addition, the short focal extent of the acoustic beam potentially limited energy delivered at deeper depths. Lastly, the focal beam for the C5-2 probe was electronically steered to broaden its acoustic width and would miss small fragments during a portion of the burst.
To improve on the success of the clinical trial in clearing collections of stones, a custom probe (SC-50) was designed with the following: (a) a broad uniform acoustic field, (b) a long focal beam to cover clinically relevant depths, and (c) a longer burst duration that would nominally overheat the C5-2 probe. The goal of this study was to compare the effectiveness and safety of the custom SC-50 probe to that of the commercial off-the-shelf C5-2 probe used in the first human clinical trial. Effectiveness was evaluated by quantifying the ability of the probe to move a stone or stone fragments 30 mm against gravity in a tissue mimicking calyx phantom. Safety of the SC-50 was evaluated in an acute porcine animal study and 7-day porcine survival study.
Materials and Methods
Therapy probe
The principal differences in operation between the SC-50 (Sonic Concepts, Woodinville, WA) and C5-2 (Philips Ultrasound, Bothell, WA) probes are listed in Table 1. The C5-2 operates as both imaging and therapy transducer. The SC-50 requires a second, integrated, transducer for real-time image guidance (P4-2, Philips Ultrasound) (Fig. 1). The C5-2 allows the stone to be targeted anywhere in the image plane, but requires the operator select the location of each burst. The SC-50 has a fixed focus and the operator must align the stone within the target region. Burst duration for the C5-2 probe is capped at 50 ms. The driving electronics (VDAS-1; Verasonics, Redmond, WA) were not designed to sustain maximum output beyond 50 ms. If extending the burst were possible, probe surface heating would exceed the US Food and Drug Administration (FDA) limit of a 10° rise within several hundred milliseconds. Burst duration for the SC-50 was tested up to 3 s. The C5-2 probe couples directly to the skin while the SC-50 contacts the skin through a water-circulating coupling head.

Photographs of the SC-50 probe with the P4-2 imaging transducer:
The acoustic field also varied between the two probes. The focal beam, defined by where the pressure is half the peak, as measured with a hydrophone, is 1.0 mm wide in the image plane, 3.5 mm wide in the elevational plane, and 1 cm in depth for the C5-2 (Fig. 2a) (HGL-0085, Onda Corp., Sunnyvale, CA). 9 –11 To spread the energy over a larger region, the beam is electronically steered in width creating a strobing effect over a 3.5 × 5.0 mm beam cross section. The SC-50 insonifies a similar focal cross section, but uniformly, and which extends 8 cm (Fig. 2b) (Reson 4038; Teledyne Reson, Camarillo, CA). Both probes operated at a peak derated burst average intensity of 90 W/cm2 (FOPH 2000; RP Acoustics, Leutenbach, Germany). 12
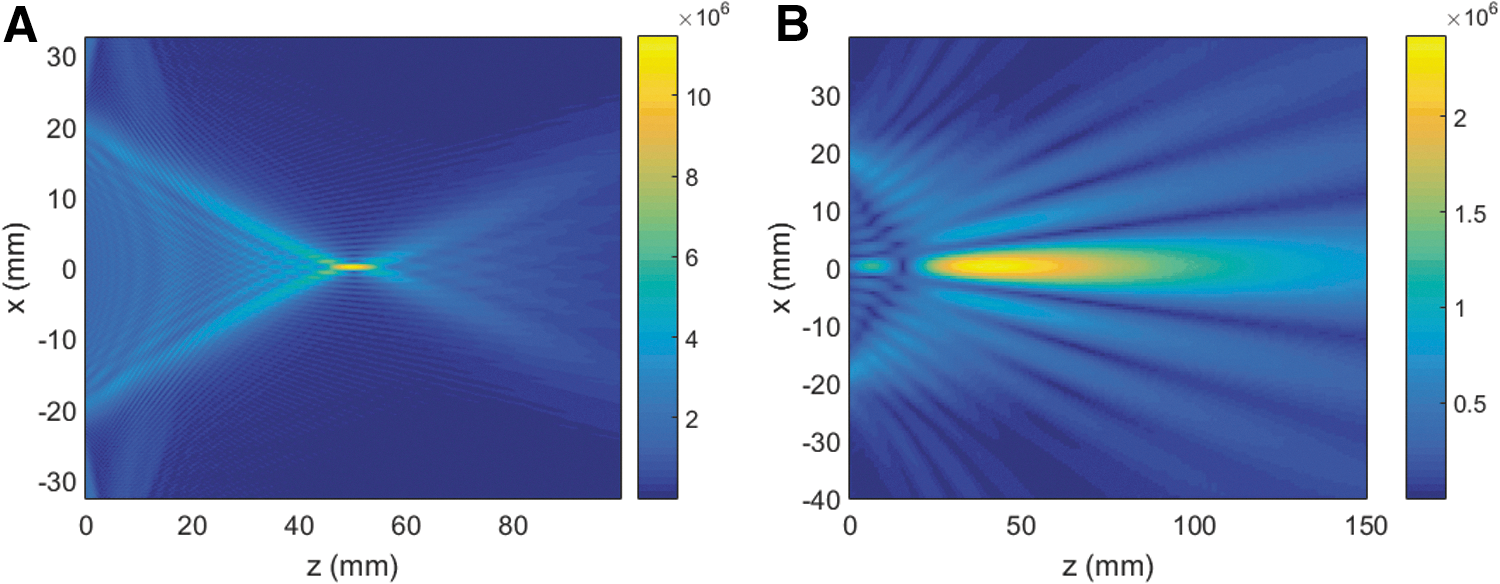
Comparison of the numerically simulated in-plane beam profile for the C5-2 probe
Effectiveness phantom
The phantom consisted of a water-filled well (12-mm diameter × 30-mm deep) in a block of tissue mimicking material, simulating a kidney calyx (Fig. 3). The tissue mimicking material was tuned to the attenuation and sound speed of human soft tissue. 13 The transducer was positioned below the phantom; the ultrasound was coupled through a 1.5 mm silicone sheet using ultrasound gel, simulating transmission through skin. Two phantoms were fabricated, and experiments were conducted at the peak focal depth of the two probes (4.5 cm) and at a focal depth representative of a larger body habitus (9.5 cm).
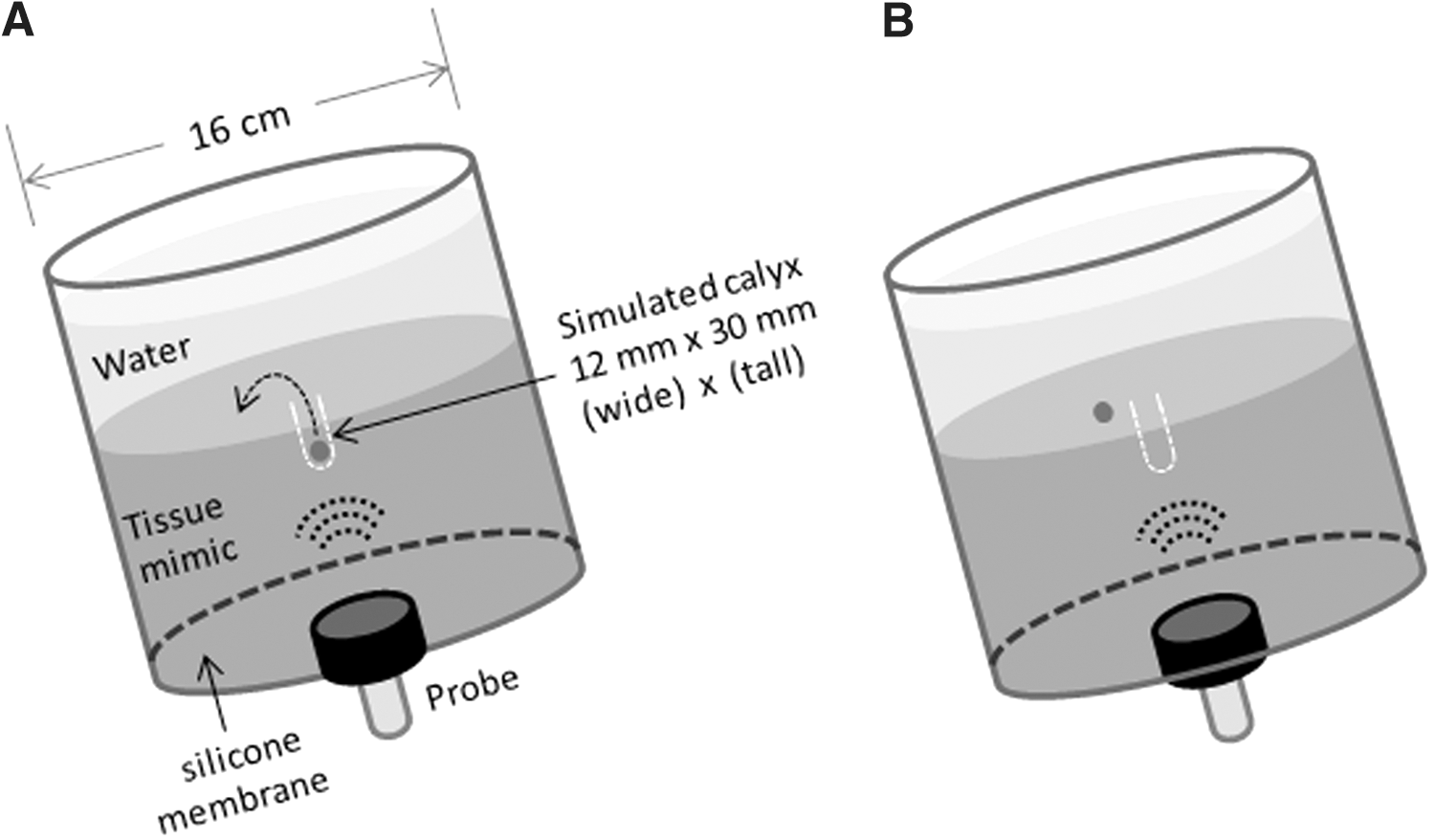
Diagram of the calyx phantom. Human calcium oxalate monohydrate stones were used as the treatment target. The stones were sifted using wire mesh into three separate groups: 10 fragments 1–2 mm in largest dimension, 10 fragments 2–3 mm in largest dimension, and one 4 × 7 mm stone.
Temperature measurement
Probe surface heating was measured using a thermocouple (75 μm type T; Omega Engineering, Stamford, CT). 13 For the C5-2, the thermocouple was secured to the probe surface with the junction aligned near probe center. For the SC-50, the thermocouple was affixed to the silicone membrane and the probe positioned so that the thermocouple aligned with the therapy beam. In both cases, the thermocouple was connected to a data acquisition system (USB-9162 module carrier and NI-9213 input module; National Instruments, Austin, TX), and temperature data were recorded through a LabVIEW interface. Both thermocouples were calibrated against a digital thermometer with certification of traceability to the National Institute of Standards and Technology (Fluke 52-II; Fluke Corp., Everett, WA).
Preclinical safety studies
The C5-2 was shown safe in animal studies and reported previously. 3,8 Here, we report two animal safety studies with the SC-50. Both studies were approved by the Institutional Animal Care and Use Committee at the University of Washington. Analysis of injury was performed by a board certified veterinary pathologist blinded to the exposure conditions. Our intent with the animal studies was to establish safety under extreme conditions beyond what would be used clinically. With the continuous 10 min exposure that was planned, the small diameter (5 cm) of the SC-50 probe would have resulted in skin injury due to the elevated spatial average intensity. 14 –16 Therefore, a 7 cm diameter probe with reduced spatial average intensity at the skin surface was used. The pre-SC probe operated with the same peak focal pressure and peak focal intensity as the SC-50, delivered over twice the focal volume. Both the acute and survival animal studies were conducted with the 10-minute continuous dose exposure where each burst consisted of 25 ms of on time followed by 25 ms of silence (50% duty cycle).
Survival study
Nine domestic pigs were included in the study with six exposed to ultrasonic propulsion (a single site within one kidney), one sham exposed, and two nontreated controls. No stones were implanted for this study, and the endpoint was day 7 postexposure. Urine and blood were evaluated with serum chemistry, hematology, and coagulation parameters from samples collected on day 0, before and after the ultrasonic propulsion exposure, and on day 7. A full necropsy was conducted on day 7. Tissue samples within the kidney and surrounding tissues were collected for all pigs. The samples were fixed in 10% neutral buffered formalin, embedded in paraffin, and sectioned and stained with hematoxylin and eosin (H&E).
Acute study
A single 2–5 mm calcium oxalate stone was implanted in the collecting system of both kidneys of four pigs by retrograde ureteroscopy, or abdominal incision and access through the ureter. Three animals (six kidneys) were ultrasound exposed; one animal was used as a control with no exposure. The sonographer used ultrasound imaging to align and trap the stone in one location for the 10 min exposure. Ultrasound images were observed during exposure to look for echogenicity, which would indicate cavitation and possible injury. At the end of exposure, the abdomen was opened, the kidneys carefully extracted, and the kidney filleted open to identify and mark the location of the stone for injury evaluation.
The kidney and intervening tissues were evaluated by eye for gross injury. A 2 × 2 cm sample centered on the treatment site within the kidney was extracted for microscopic evaluation. Cutting along the center of the treatment region, one half was fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned and stained with H&E. The second half was embedded in a mold in optimum cutting temperature medium by submerging it in isopentane cooled on dry ice. Frozen sections were stained with Nicotinamide adenine dinucleotide (NADH) diaphorase to identify potential thermal injury. 17 Even with NADH staining, thermal injury to the sinus might be difficult to distinguish. Therefore, samples were compared to excised kidney sinus exposed to a soldering iron tip for 3 s and then fixed or embedded the same way.
Results
Effectiveness
The results for effectiveness in moving fragments out of a 30 mm deep well against gravity are summarized in Table 2. The results were similar for the two probes using a 50 ms burst duration; no stones were expelled with the C5-2 and only 2%–3% were expelled at the shallowest depth with the SC-50. This is the maximum burst duration for the C5-2 probe. At a burst duration of 3 s, 100% of stones were expelled at both treatment depths with the SC-50. The temperature rise at the interface of the probe and the silicone membrane was <0.5°C for both durations with the SC-50 probe compared to 2°C for the 50 ms duration with the C5-2.
Figure 4 shows representative images of stone movement by the two probes at the two burst durations. With the 50 ms burst duration, the stone and stone fragments are moved by both probes, but a shorter distance than 30 mm. There is also a decrease in the ability to move stones between the 4.5 and 9.5 cm depths. All stones are moved greater than 30 mm with SC-50 probe operating with a 3 s burst duration, with a similar expulsion distance for both the 4.5 and 9.5 cm cases.

Representative still images of the distribution of 2–3 mm stone fragments for each of the three test conditions. The calyx was positioned above the tissue mimic for visualization. Stones were moved in all cases.
Preclinical safety studies
Survival study
No animal displayed adverse clinical signs. There were no macroscopic findings in tissues below the skin. No echogenicity was observed on ultrasound during exposure to indicate cavitation. All blood and urine values were within the range and variability of the control animals. There were no microscopic findings associated with the experimental use of the investigational device within the kidney or intervening subdermal tissue (as shown in Fig. 5). This was determined from 38 treated kidney sections, 47 other treated tissue sections, and 65 control or sham tissue sections. There was mild thermal skin injury in three animals treated with the pre-SC probe, one that remained at sacrifice.
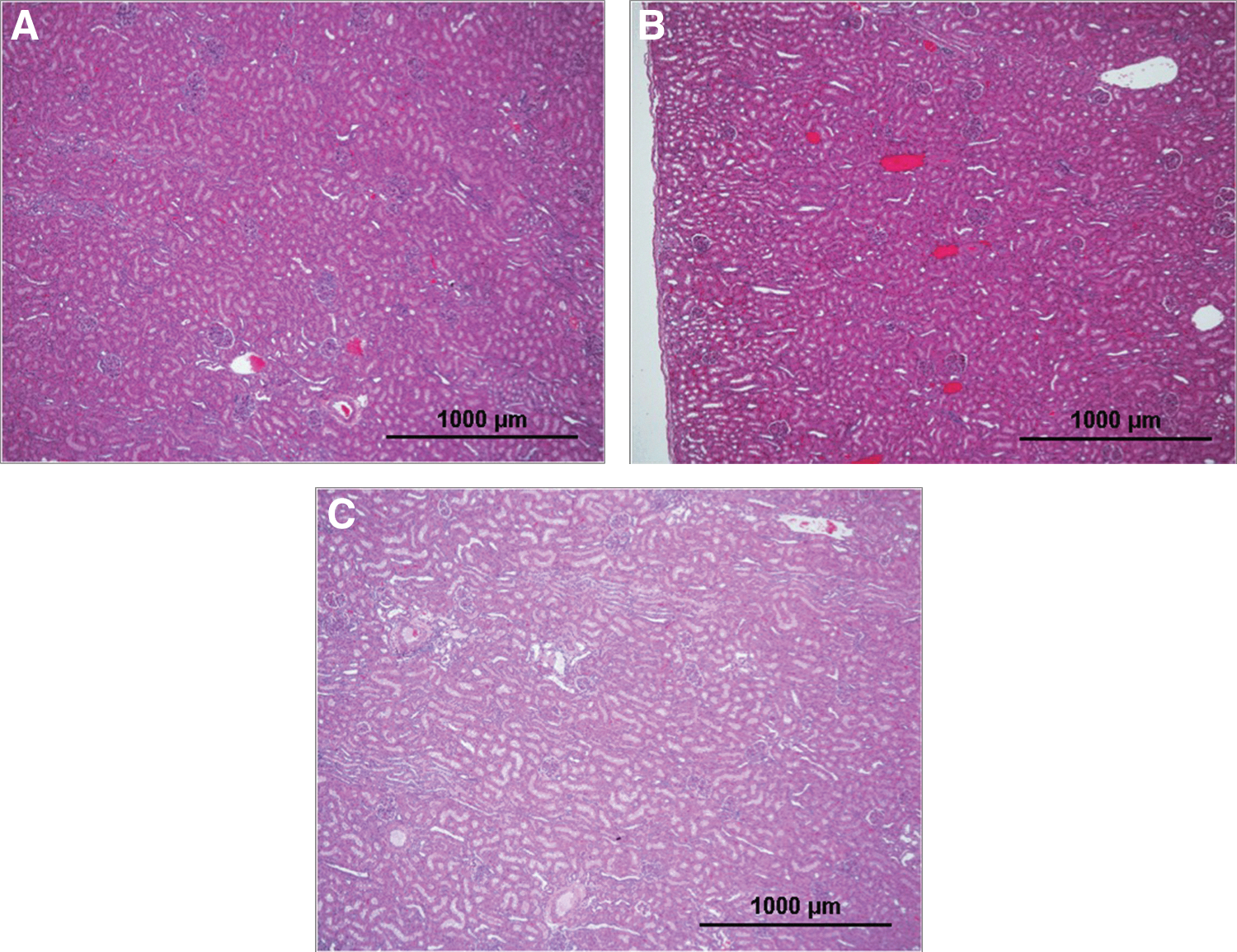
H&E stained histology slides from the survival safety study of clinical simulation using a continuous 10-minute exposure at 50% duty cycle. Slide
One animal within the treatment group was euthanized on day 2 for what was attributed post mortem as mucus plug in the trachea. A sham animal received similar concern, was febrile to 40.6° C, but recovered with antibiotics and anti-inflammatory medications. Neither was considered associated with the investigational treatment.
Acute study
Acute study data showed no additional risk of injury associated with the presence of a stone. No echogenicity indicative of cavitation was observed during imaging. Gross evaluation showed wire perforations in all kidneys in which stones were implanted with ureteroscopy. Histological evaluation under H&E staining showed evidence of focal traumatic injury in the renal pelvis and nearby tissues in all animals, which was associated with surgical implantation. This injury was distinct from device-related injury, which, if present, was expected in the mid-cortex or medullary regions, and to show evidence of cavitation, coagulation, and necrosis. Microscopic damage was only observed in the NADH-stained tissue that was exposed directly to a soldering iron intended to produce a positive thermal control (Fig. 6).
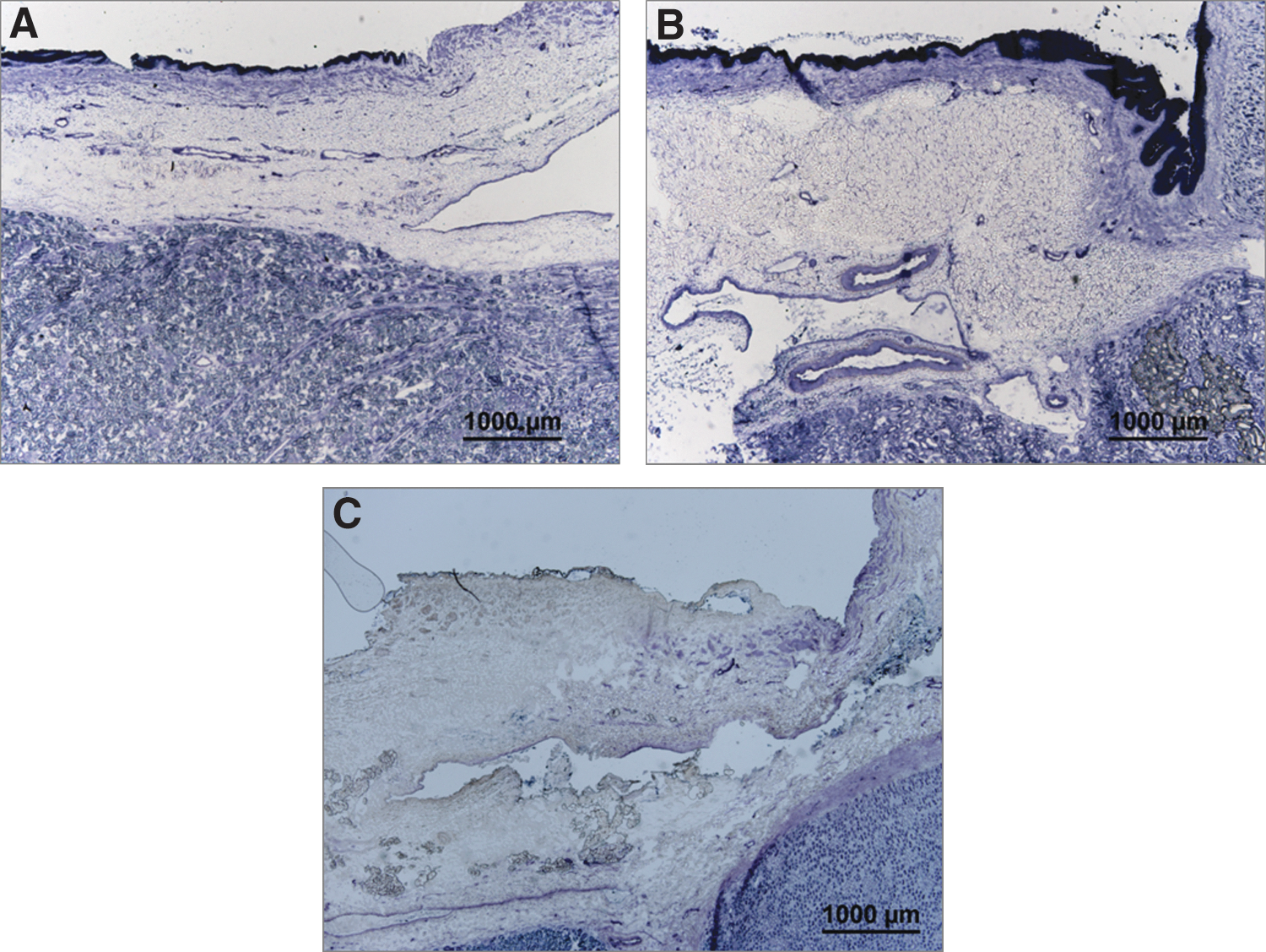
Nicotinamide adenine dinucleotide (NADH) diaphorase histology slides from the acute safety study with the stone present. Slide
Discussion
This study compared two ultrasonic propulsion probes. The C5-2 probe used in the first feasibility studies of repositioning stones in humans has the benefit of an off-the-shelf component, that can be used for both pushing and imaging, with the ability to target the stone anywhere in the image field. 2 The results reported for this study demonstrate the SC-50 probe provides the benefit of sustaining longer burst durations. Both probes moved stones, but neither was effective at expelling stones out of the 30 mm deep well without increasing the burst duration from 50 ms, the maximum output of the C5-2, to 3 s, an option only available with the SC-50. The longer focal beam of the SC-50, extending 8 cm vs 1 cm with the C5-2 probe, provides the benefit of similar effectiveness across a broad range of body habitus, as demonstrated by the ability to clear all stones at both 4.5 and 9.5 cm. The same exposure applied in an extreme dose of 10 minutes continuously (instead of 3 s bursts) did not cause thermal or cavitation injury to the kidney or intervening subdermal tissues in a porcine animal model.
There are limitations to this effectiveness study as no simulation completely replicates the clinical situation. This study specified the ability to move the stone greater than 30 ms as a measure of success, which was not necessary in the clinical trial where repeated smaller movements caused stones to pass. Future phantoms will continue to measure the effectiveness of additional features, refine the design, and form a basis for training. 18,19 We anticipate that the longer broader exposure of the SC-50 probe will make alignment and operation faster and easier, and its benefits even more dramatic in clinical use.
Limitations in interpretation of the safety study results include lack of dose escalation and slightly exceeding known skin exposure limits to test a greater exposure at the kidney. The survival animal study was designed as a dose ranging study, but lower exposures were not conducted when kidney injury was not observed at the extreme case of treating one tissue location with 10 minutes of continuous bursting. The lack of injury at the extreme exposure was consistent with lack of injury reported previously in a dose ranging study for the C5-2 probe. 20 The mild skin injury seen in three animals was believed due to the spatial averaged time averaged intensity (ISATA) at the skin surface. ISATA >3 W/cm2 can cause thermal injury by absorption of ultrasound within the skin, and is the limit imposed on ultrasound physiotherapy devices for FDA marketing clearance. 14 –16 The pre-SC probe exposure operated near, but above, the 3 W/cm2 limit. To mitigate the potential for injury, clinical exposure with the SC-50 probe will be limited to individual bursts up to 5 s in duration. This will be followed by twice the burst duration in off time, resulting in a maximum ISATA of 1.5 W/cm2, which is half the FDA limit. In addition, the probe will be moved, not held fixed, throughout a clinical treatment to follow the moving stones.
Conclusions
We have developed a custom probe for ultrasonic propulsion that allows for longer duration bursts with a broad uniform focal beam over greater depths. This probe was shown to be safe in animal studies and appears more effective in phantom studies than the probe used previously in human trials. The new probe was designed to facilitate passage of postlithotripsy fragments, but the data support this probe also moving a large stone. The FDA approved investigational use of this probe in humans. A randomized clinical trial of the safety and effectiveness of expelling postsurgery fragments and a feasibility study of moving obstructing stones in the Emergency Department are underway.
Footnotes
Acknowledgments
We appreciate the help of our colleagues at the University of Washington (UW) Center for Industrial and Medical Ultrasound, UW and Madigan Urology Departments, and the NIH NIDDK Program Project DK043881. Specifically, we would like to thank UW student Lei Kapaku for help with measurements, UW Emergency Department Physician M. Kennedy Hall, and Urology Resident Phil May for helping design the clinical trials, and research coordinator Alana Clark for help in directing the studies to justify IRB approval of the trials. This work was supported by the National Space Biomedical Research Institute through NASA NCC 9-58, National Institute of Diabetes and Digestive and Kidney Diseases grant P01 DK043881, and the Madigan Army Health System Department of Urology residency program. Some of this material is the result of work supported by resources from the VA Puget Sound Health Care System, Seattle, WA.
Author Disclosure Statement
Bailey, Cunitz, Dunmire, and Sorensen have consulting agreements with and equity in SonoMotion, Inc. which has licensed this technology from the University of Washington. The remaining authors have no competing financial interests.