
Abstract
Introduction:
Urological surgeries have contributed to the increasing prevalence of minimally invasive robotic procedures. Although factors influencing the adoption of robot-assisted radical prostatectomy have previously been identified, the explanation for the rapid rise in robotic partial nephrectomies remains unknown. Using a retrospective population-based sample, we attempt to determine hospital and surgeon-specific factors influencing a surgeon's decision to utilize robotic assistance for partial nephrectomies.
Materials and Methods:
A nationally representative weighted sample of all men who underwent a partial nephrectomy in the United States between 2003 and 2014 was identified within the Premier Hospital Database. Hospital, surgeon, and patient characteristics for each operation were analyzed. Descriptive statistics and a multivariate regression model stratified according to the Law of Diffusion of Innovation were performed.
Results:
A weighted sample of 14,890 nephrectomies was included in the study. Patient demographics were similar between the two groups. The adoption of robotic technology followed the Law of Diffusion of Innovation with the percentage of partial nephrectomies with robotic assistance increasing yearly, reaching 64.1% by 2013. Surgical volume was a significant factor driving the use of robotic assistance, with high volume surgeons (>5 partial nephrectomies/year) performing 23.2% more robotic partial nephrectomies per year than their low volume colleagues (< = 5 partial nephrectomies/year) from 2009 to 2013 (p < 0.001).
Conclusions:
This retrospective population-based study examines key factors influencing the diffusion of robotic technology for partial nephrectomies. Surgical volume and year of surgery were found to be the most significant factor in robotic adoption, with other patient and hospital-specific characteristics playing a minor role. Future studies are needed to correlate adoption rates with the clinical or cost-effectiveness of novel technologies within the medical field to determine whether rapid adoption is a patient-centered vs a clinician-centered decision point.
Introduction
T
Studies have shown that minimally invasive approaches in general, with or without robotic assistance, reported lower rates of blood loss, transfusion rates, and catheterization time. 2,3 However, the benefits of robotic over laparoscopic approaches for partial nephrectomies require additional study, given the absence of head-to-head randomized controlled trials comparing robot-assisted partial nephrectomies (RAPN) and Laparoscopic partial nephrectomies (LPN). Early meta-analyses reported comparable outcomes between LPN and RAPN, including operative times, estimated blood loss, conversion rates, complication rates, and number of positive margins, although a robotic approach was associated with decreased warm ischemia times. 4,5 Other studies have also found RAPN to be associated with higher costs, although these were partially offset by a shorter length of stay. 6 –9 Only recently, long-term outcomes of RAPN have become available with studies showing comparable 3- and 5-year recurrence-free survival rates between RAPN and LPN. 10,11
Although early meta-analyses did not indicate a clear advantage to a robotic approach, later studies have shown RAPN to have a significant advantage over LPN. A recent meta-analysis by Leow and colleagues, including 4919 patients, concluded that RAPN had lower rates of any or major complication scores, fewer positive margins, and shorter warm ischemia time. 12 A retrospective multi-institutional study by Zargar and colleagues comparing 1185 robotic partial nephrectomies and 646 laparoscopic partial nephrectomies with “Trifecta” as the primary outcome (a composite outcome of negative margin, no complications, and a warm ischemia time <25 minutes) found that a robotic approach achieved much higher trifecta rates compared to a laparoscopic approach (70% vs. 33%). 13 Another retrospective study by Ghani and colleagues, including 38,064 partial nephrectomies from the National Inpatient Sample, showed lower rates of intraoperative complications as well as higher hospital charges with robotic procedures. 14 Additional evidence suggests that patients undergoing RAPN are also less likely to be readmitted, although these patients also accumulated higher excess hospital charges. 15 In summary, although earlier evidence suggested equivocal results between RAPN and LPN, more recent studies have shown advantages to a robotic approach with partial nephrectomies, although these have been associated with higher costs to the healthcare system.
Studies have also shown that adoption of RAPN has been rapid, with Ghani and colleagues reporting an annual increase in utilization of 45.4% compared to 7.9% and 6.1% for open and laparoscopic approaches in 2010. 14 Other institutional studies have shown that robotic assistance is rapidly becoming the predominant modality for partial nephrectomy (PN). 15,16
Given the swift incorporation of robotic assistance in urological practice, the main factors driving a clinician's decision to utilize robotic technology become an important practice-based question. Although our group has previously described the relevant factors for robotic adoption into radical prostatectomies, 17 the same analysis has not yet been done for RAPN, which are commonly performed for low-stage renal tumors. The purpose of this study is to describe the adoption pattern of robot-assisted technology for partial nephrectomies and determine the relevant hospital and surgeon-specific factors affecting a surgeon's decision to utilize robotic assistance in performing a PN.
Materials and Methods
Study cohort
This is a retrospective population-based study utilizing the Premier Hospital Database (Premier, Inc., Charlotte, NC), a nationally representative sample capturing 20% of all inpatient admissions. All hospital admission data were deidentified before analysis, and institutional review board exemption was granted from our institution. We identified all men receiving a PN using the International Classification of Diseases, Ninth Revision (ICD-9) code (55.4, partial nephrectomy). The study period extended from January 1, 2004 to December 31, 2013, to capture the primary period of robotic diffusion in the United States. The Premier Database contains comprehensive billing data for each patient, which was utilized to identify and separate out open, laparoscopic, and robotic procedures. This was done using a detailed review of the charge description master (CDM) for each patient, which details specific operating room supplies unique to robotic procedures. The CDM was also used to generate a robotic variable indicating which hospitals had an available da Vinci robot; observations were dropped from the analysis if we were unable to confirm the presence or absence of a robot using the CDM.
Physician volume and adoption
The Premier database also contains unique physician identifiers, allowing us to quantify each individual attending's annual surgical volume. These data were used to categorize surgeons into low- and high-volume surgeons based on clinical reasoning. The surgical volume categories were defined according to clinical experience; “low-volume” was defined as five or fewer partial nephrectomies annually, and “high-volume” was defined as greater than five cases per year. Our outcome variable was defined as the percentage of nephrectomies that were performed robotically each year for an individual surgeon.
Patient and hospital characteristics
We evaluated baseline patient characteristics that had the potential to influence the decision to utilize robotic surgery, including age (<40, 41–50, 51–60, 61–70, >70), race (White, Black, Hispanic, Other), and insurance status (Medicare, Medicaid, Private Insurance, Other). To account for baseline health status, we calculated the Charlson Comorbidity Score, a measure of a patient's illness that is predictive of 10-year mortality rates. 18 We also examined relevant hospital characteristics, including number of beds (<200, 200–399, ≥400), type (teaching or non-teaching), location (urban or rural), and region (Midwest, Northeast, South, West).
Statistical analysis
A descriptive summary of patient and hospital characteristics was performed for patients undergoing robot-assisted and nonrobot-assisted nephrectomies (either open or laparoscopic procedures). Chi-squared tests using the Rao–Scott correction factor were performed on baseline patient characteristics to examine the correlation between explanatory variables and type of surgical approach (open, laparoscopic, robotic) for nephrectomies. We limited the analysis to surgeons performing partial nephrectomies at hospitals with an available robot and examined yearly trends in adoption rates of robotic nephrectomies over time, defined as the percentage of partial nephrectomies performed robotically, averaged across all surgeons.
We then constructed multivariate linear regression models to determine relevant factors for robot-assisted PN adoption such as academic vs community settings, urban vs rural populations, hospital size, volume of surgical cases, and region. These multivariate linear regression models were stratified by different time periods according to the Law of Diffusion of Innovation, including the innovator, early adopter, and early majority phases. By definition, the innovator, early adopter, and early majority time periods correspond to when 2.5%, 16%, and 50% of the population have adopted a novel technology, respectively. 8,15,16 Only surgeons practicing at hospitals with available da Vinci surgical systems were included in the regression analysis.
For these analyses, we applied survey weighting to generate a nationally representative sample. All statistical tests were two sided and an α level of <0.05 was considered statistically significant. All analyses were performed using Stata 14 Statistical Software (College Station, TX).
Results
Within this study, a total of 16,592 partial nephrectomies were performed on men between the years of 2004 and 2013. Of these observations, the presence or absence of a robot at the admitting hospital could be determined for 14,890 observations, all of which were included in the study. The baseline characteristics of these patients are described in Table 1, which showed no significant differences between patients who did and did not receive robotic assistance.
PN = partial nephrectomy.
Diffusion of robot-assisted nephrectomies
There was a progressive increase in the adoption of robotic assistance for partial nephrectomies in the United States from 2004 to 2013, similar to earlier findings of rapid diffusion of robotic technology for radical prostatectomies. 1 Throughout this entire period, from 2004 to 2013, 32% of PN cases were performed robotically. According to the Law of Diffusion, the innovator, early adopter, and early majority phases for the technological adoption of RAPN occurred from 2004 to 2005, 2006 to 2008, and 2009 to 2013, respectively (Fig. 1). The percentage of partial nephrectomies performed robotically grew steadily from 1.3% to 2.3% during the innovator phase and then quickly quadrupled during the early adopter phase from 3.7% to 12.1%. By the end of the early majority phase in 2013, the percentage of PNs performed with robotic technology had increased to 64.1%.
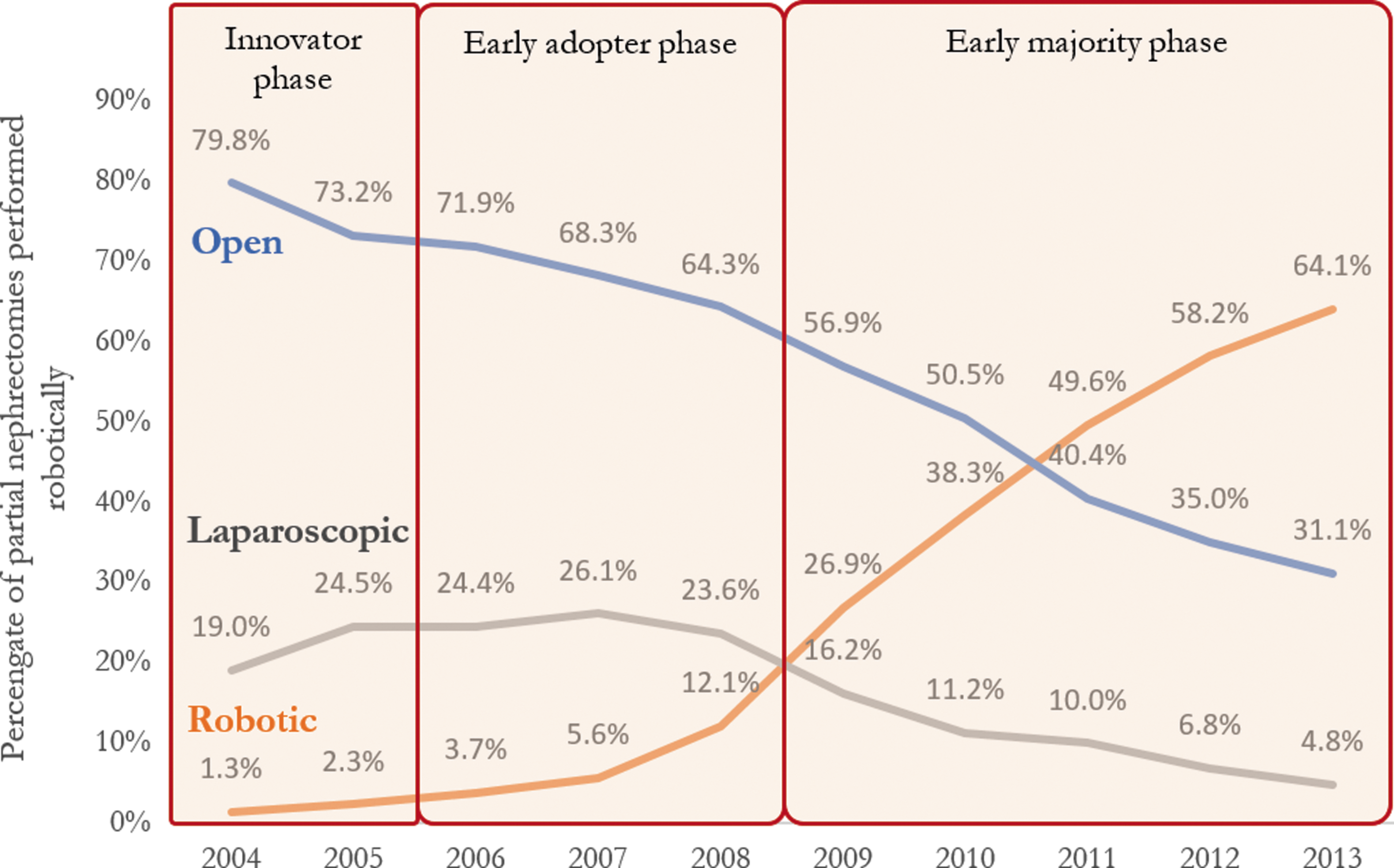
Trends in the adoption rates of robotic partial nephrectomies in the United States from 2004 to 2013, stratified by the corresponding phases of the Law of Diffusion of Innovation.
Relevant factors for robotic assistance utilization for partial nephrectomies
For our multivariate linear regression analysis, we examined the percentage of partial nephrectomies performed robotically by individual surgeons within the innovator, early adopter, and early majority phases, according to the Law of Diffusion of Innovation (Table 2). During the innovator phase, we found no variables to be predictive of robotic assistance for PNs. During the early adopter phase, which contains the steepest period of growth in technological adoption, both surgical volume and year of surgery were significant predictors of robotic adoption. High-volume surgeons (>5 PN/year) were 7.0% more likely to perform their PN robotically compared to their low-volume colleagues (≤5 PN/year) (p = 0.049), and the utilization of robotic assistance for partial nephrectomies increased by 4.6% with each passing year (p < 0.001). These factors were reenforced during the early majority phase, during which a majority of surgeons utilized robotic assistance. Surgical volume and year of surgery continued to be strong predictive variables, with high-volume surgeons performing 23.2% more PNs robotically (p < 0.001) than their low-volume colleagues and a concurrent increase in robotic assistance by 8.6% (p < 0.001) with each progressive year from 2009 to 2013. Interestingly, hospitals in the Northeast performed 16.7% fewer robotic partial nephrectomies compared to their Midwest counterparts.
Surgeon adoption is defined for each individual surgeon as the number of robotic partial nephrectomies divided by the total number of partial nephrectomies in a particular year. Results of the multivariate regression analysis are reported in percent changes relative to the reference value.
Statistical significance: * p < 0.05, ** p < 0.001.
Ref. = reference.
Discussion
This study examines the distinct similarities and differences between the adoption pattern of robot-assisted partial nephrectomies compared to robot-assisted laparoscopic prostatectomy, which has been previously described in the literature. 17 In addition, we examined national trends in robotic PN from 2004 to 2013. While Ghani and colleagues found that a majority of partial nephrectomies still utilized an open approach in 2010, we found that by 2013, a clear majority of PNs (64.1%) were performed robotically (Fig. 1). 14 According to our findings, trends in technological diffusion occurred a year later for RAPN compared to RALP, likely due to several factors. 19,20 We theorize that unlike RALP adoption, which was initially driven by marketing and patient demand, RAPN adoption was most likely driven by RALP surgeons now familiar with the robotic platform, utilizing it for the more complex PN. Although our study is currently limited to partial nephrectomies, this is a potential topic for future research. 21,22 The reasons for doing so reflect the advantages of using robotics for RAPN, including magnification and greatly improved dexterity for accurate intracorporeal suturing, allowing surgeons to overcome the technical challenges inherent with laparoscopic partial nephrectomies. 23,24 Unlike RALP, where the initial adoption occurred in academia, for RAPN there was no predilection toward academic providers. 17 At first, this may seem surprising, but perhaps by the time RAPN adoption was in full swing, urologists both in the private and academic settings were comfortable with the robotic platform.
The adoption of both RAPN and RALP behaved according to the Law of Diffusion of Innovation, which is a principle that describes the process and speed at which new technological advances are disseminated into society and has been validated across a wide range of disciplines. 25 –28 During the innovator phase, no variables were significant factors in robotic adoption, likely due to only a few surgeons adopting an extremely novel technique. Both surgical volume and year of surgery were significant variables during the early adopter phase, which is characterized by the incorporation of new technology by key opinion leaders. 29 –31 The early majority phase is characterized by surgeons who tend to adopt a new technology only after it has been effectively and consistently demonstrated by others in the field. Our analysis showed that during this phase, surgical volume had both a significant and large-magnitude effect, indicating that volume is the most influential factor in RAPN adoption. The highest-volume providers were more likely to adopt robotic assistance than the low-volume surgeons, indicative of increasing consolidation of robotic procedures among providers with the highest volumes, mirroring trends seen in RALP. 32 By the end of the early majority period, RAPN had achieved a majority share in PN, with a similar trend previously seen in RALP. 17
Given that the highest-volume providers are most likely to adopt novel surgical techniques, focusing efforts on addressing this cohort of high-volume surgeons is essential in affecting the dissemination of technological innovation in surgical care. Ultimately, evidence-based clinical medicine requires us to carefully assess whether large-scale adoption of novel technology is appropriate by establishing a relationship between the rate of technological adoption and demonstrated clinical safety or efficacy through randomized controlled trials.
Limitations
This retrospective population-based analysis is not without limitations. Although our dataset has the advantage of capturing 20% of all inpatient admissions, these data were obtained through hospital sampling and may be subject to sampling bias, although survey weighting was used to mitigate this effect. Second, this analysis relied on CDM data to determine whether a procedure was performed open, laparoscopically, or robotically, as well as the presence or absence of a da Vinci robot, both of which were key components of our analysis. The reliability of this outcome variable is dependent on the accuracy of CDM coding, which may be less accurate than ICD-9 coding. Finally, the Law of Diffusion of Innovation is traditionally applied to binary outcomes, where a person has either adopted or refused to adopt a novel technology. In contrast, the adoption of robotic technology is a continuous rather than binary variable, with surgeons performing a percentage of their caseloads robotically instead of an all or nothing approach.
Conclusion
This retrospective population-based study sheds new evidence on the process and key factors influencing the diffusion of robotic technology for partial nephrectomies, which has not been previously described. We show that uptake of robotic technology acted according to the Law of Diffusion, with a rapid increase in adoption occurring from 2006 to 2008 with 64% of partial nephrectomies performed robotically by 2013. The incorporation of robotic technology into the performance of partial nephrectomies occurred concurrently with consolidation toward high-volume surgeons, which were overwhelmingly more likely to utilize robotic technology. Finally, this study demonstrated that high-volume surgeons are important drivers of adoption of robotic technology into urology. These findings would be complemented by future studies correlating adoption rates with clinical outcomes or the cost-effectiveness of novel technologies within the medical field to determine whether rapid adoption is a patient-centered vs a clinician-centered decision point.
Footnotes
Author Disclosure Statement
No competing financial interests exist.