
Abstract
Introduction and Objective:
Recently there has been interest in a dusting technique for lithotripsy during ureteroscopy (URS) utilizing high-frequency and low-pulse energy (HiFr-LoPE) settings. We assessed a 120-W holmium laser that permits high-frequency (>50 Hz) dusting.
Materials and Methods:
Consecutive URS cases performed by a single surgeon using the P120H (Lumenis, San Jose, CA) were reviewed. Lithotripsy was performed using HiFr-LoPE settings (50–80 Hz/0.2–0.5 J [10–40 W]). Residual fragments (RFs) were determined on postoperative radiography, ultrasonography, or CT. Complications were classified using the Clavien–Dindo grade.
Results:
URS was performed on 82 renal units (71 patients). Renal stones constituted the majority (73%), including four partial staghorn stones. Mean stone size and density (HU) were 12.5 mm (SD 8.7; range 5.0–50.0) and 993 (SD 353; range 230–1580), respectively. Ureteral access sheath was used in 15 (21%) patients. Mean total laser energy per case was 5.2 kJ (range 0.1–42.1). Dusting was exclusively performed in 84% of cases. Postoperative stents were placed in 91% (41% string). Zero-fragment and ≤2 mm RF rates were 62.1% and 74.2%, respectively. There were 11 complications (13%) (grade 1 = 5, grade 2 = 6). The emergency department visit rate was 5.6%. There were no hospitalizations or reinterventions.
Conclusions:
Refinements in laser technology have expanded methods to ablate urinary stones. Outcomes utilizing a dusting technique demonstrated acceptable RF and complication rates. However, not all stones are amenable to dusting, and further study is needed to define the optimal role of this technique during laser lithotripsy.
Introduction
I
Dusting during URS utilizes laser settings of high-frequency and low-pulse energy (HiFr-LoPE) to ablate stones into submillimeter fragments. 8 With this strategy, fragments are left in situ for spontaneous passage, thus avoiding the need for retrieval. Despite increasing interest in dusting, there is limited literature on this methodology. 9 One reason is that the first generation of Ho:YAG lasers was unable to utilize very low-pulse energies or high-pulse frequencies to permit an efficient dusting technique. The aim of our study is to report the clinical application of a new high-power 120 W Ho:YAG laser for URS lithotripsy, designed to improve a dusting technique. We examined our initial experience using this new technology for patients undergoing URS lithotripsy.
Discussion of Technology
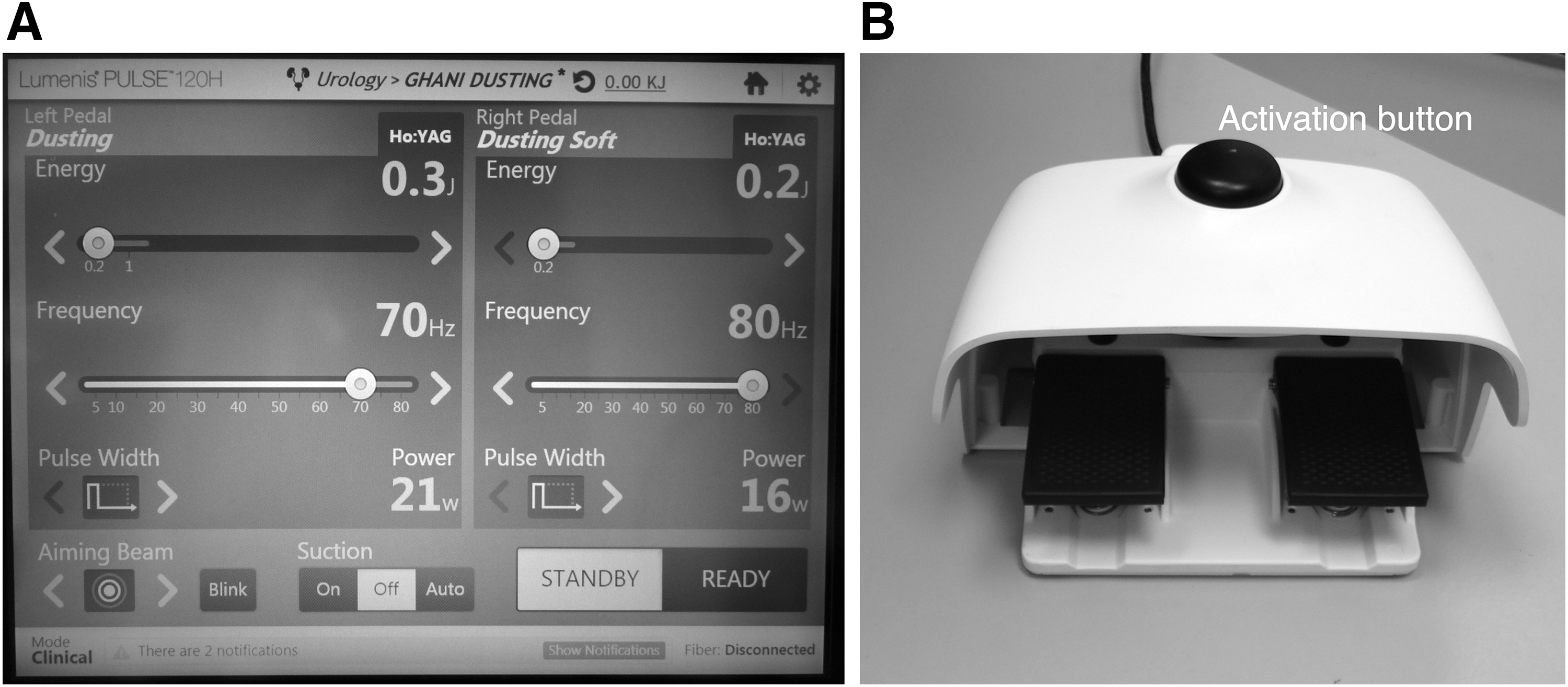
We used a 120 high-power Ho:YAG system (Pulse 120H; Lumenis, Inc.). High-power Ho:YAG lasers are able to operate at pulse frequencies of >40 Hz. 10 Energy settings achievable with the Pulse 120H range from 0.2 to 6 J, with repetition rates varying from 5 to 80 Hz (i.e., pulses of energy/second). This is the first Ho:YAG laser that permits frequencies >50 Hz. In this evaluation, we began dusting in the ranges of 0.2 to 0.5 J, with frequencies between 50 and 80 Hz. The P120H has the ability to program surgeon-specific laser settings and a dual pedal footswitch to interchange between two different laser settings instantaneously without the need for a pause in the system activation (Fig. 1). Pulse energy and frequency settings can be adjusted to provide a dusting effect dependent on stone size and composition. We utilized it so that preset settings included dusting for hard stones (i.e., >1000 HU–70 Hz × 0.3 J [21 W]), dusting for soft stones (<1000 HU–80 Hz × 0.2 J [16 W]), and fragmentation (8 Hz × 1.4 J [11 W]) (Fig. 1). All cases were performed using a short pulse width mode. Preset values for the pulse energy were chosen based on our experience of using dusting technique with a 100 W laser.
Initial Case Series
We reviewed all consecutive URS cases performed by a single surgeon (K.R.G.) using the Pulse 120H at the Ann Arbor Veterans Affairs Healthcare System. All cases were recorded on an institutional review board approved database and assessed for stone size (maximum dimension in single plane), location, stone density (HU), and use of staged procedures, UAS, and postoperative stenting. Flexible URS was performed using an Olympus URF-P6 ureteroscope. All patients had documented urine cultures before surgery. Patients with urine infection were treated with culture-directed antibiotics with documented negative culture before surgery, and all patients received perioperative intravenous prophylaxis. Holmium laser lithotripsy was begun utilizing HiFr-LoPE settings of 70–80 Hz × 0.2–0.3 J (16–21 W) depending on the hardness of the stone, with intraoperative adjustments to settings ranging from 30 to 80 Hz and 0.2 to 0.5 J (10–40 W). Higher power settings such as 80 Hz × 0.5 J (40 W) were utilized toward the end of lithotripsy for undertaking a popcorn technique in the renal calix. We used a 200 μm laser fiber; ball-tip for renal stones (Flexiva Trac tip, Boston Scientific, MA), and flat tip for ureteral stones. Laser settings and outputs were prospectively recorded within the system and collated for this evaluation. All patients who were stented were prescribed an alpha-adrenergic antagonist and continued this for 3 days after stent removal.
Stone clearance was determined on postoperative radiography (KUB), ultrasonography (US) or CT, 4 to 6 weeks after surgery (if staged procedure then after the second procedure). CT was performed for patients who were morbidly obese, had large renal stone volume (>1.5 cm), or infection stones. Complications were classified using the Clavien–Dindo grade.
Results
Over an 8-month period, URS was performed on 82 renal units (71 patients). Renal stones constituted the majority of cases (73%), including four patients with partial staghorn stones. Table 1 provides patient characteristics, including stone size, location, and stone density (HU). The mean stone size ranged from 5 to 50 mm. The majority of patients were male because of the Veteran patient population at our center. Solitary stones were noted in 63 patients (77%). Bilateral URS was performed in five patients, whereas a further six had staged procedures. UAS was used in 15 patients (21%), primarily to keep low intrarenal pressures for patients with large stone volume or risk of infection.
F = female; Ho:YAG = holmium:yttrium aluminum garnet; L = left; M = male; R = right.
Table 2 provides a summary of patient outcomes. The total mean operative time was 53 minutes (range 22–115). For stone sizes of <1, 1–2, and ≥2 cm, mean operative times were 48, 56, and 60 minutes, respectively. The mean laser energy usage was 5.2 kJ (range 0.1–42.1). This amounts to ∼5.4 minutes of laser firing if a setting of 0.2 J × 80 Hz is used for a case. Dusting settings of HiFr-LoPE was used exclusivey in 60/71 patients (84%). The remaining 16% were cases wherein a dusting technique could not be completed as stone factors such as composition, location, or retropulsion required use of standard fragmentation. When dusting specific cases were analyzed, the average laser energy was 6.7 kJ. Compared with fragmentation specific cases, the amount of laser energy used during dusting cases was not statistically significant (p > 0.05). Most cases were performed successfully using a 200 μm fiber, with only one surgery requiring a second laser fiber during the case because of fiber degradation.
ED = emergency department; HiFr-LoPE = high-frequency and low-pulse energy.
Postoperative stents were used in 91% of cases, of which 41% were on patients using self-extraction strings. The mean follow-up was 102 days (range 51–159). Stone clearance was determined using CT, combination KUB/US, or US alone in 21%, 62%, 17%, respectively. The complete stone-free rate (SFR) was 62.1%, and the ≤2 mm residual fragment (RF) rate was 74.2%. If confined to assessing stone clearance after treatment of renal stones, the complete SFR was 67.4%. In the group that received CT to assess stone clearance (patients with complex stones), the complete SFR was 39%, whereas the <2 mm RF rate was 69%. In the KUB/US and US alone groups, the SFR was 66.7% for both and the <2 mm RF rate was 83.3% and 73.3%, respectively.
There were 11 (13%) complications, Clavien–Dindo grade 1 = 5 and grade 2 = 6. These included three patients with unplanned visits for stent pain (one visited the emergency department [ED]), two patients who visited the ED for pain because of a passing RF, four patients who had urinary tract infection, one patient with pyelonephritis, and one patient who had pain from a perinephric hematoma (stone treated in a caliceal diverticulum). In total, four of these patients (5.6%) had an ED visit, but no hospitalization or procedures were required. No patients required an unplanned surgical intervention and no patients had new onset postoperative hydronephrosis on repeat imaging.
Discussion
In this study, we demonstrated the feasibility and safety of a new Ho:YAG system specifically designed to permit a dusting approach during URS lithotripsy. Dusting (HiFr-LoPE) was performed using high frequencies (>50 Hz), which were previously unobtainable in earlier generations of Ho:YAG systems. We also found that a 200 μm laser fiber adequately coped with the energies delivered by this system. The complication rates were low and no different to current literature using a variety of URS strategies. 11,12
Evidence surrounding the efficacy of a dusting approach in comparison with fragmentation and retrieval for URS stone surgery is limited. In the only randomized trial comparing laser lithotripsy strategies, Schatloff and colleagues demonstrated that after “exhaustive lithotripsy technique and spontaneous passage” for ureteral stones, patients had a significantly higher unplanned visit rate than patients undergoing active retrieval of fragments. 13 Patients underwent lithotripsy using a fragmentation setting and not HiFr-LoPE dusting. Nevertheless, the SFRs between the two techniques were not statistically different.
In a recent survey of Endourology Society members, HiFr-LoPE dusting settings were utilized by 67% of respondents. 6 The dusting technique is a growing trend and is becoming more popular among endourologists, and this highlights why our study is relevant to contemporary practice. When using a fragmentation and retrieval method, previous studies have shown that complete SFRs for renal stones based on CT follow-up approach only 54% to 62%. 14,15 Our study is a descriptive report assessing the utility and outcomes when using a new Ho:YAG system for HiFr-LoPE dusting, and although our stone clearance rates may be in this range, we are not able to assess which strategy is superior. However, we feel our results suggest at least noninferiority compared with SFR data on retrieval, with the advantage of less UAS use. Utilizing a dusting strategy offers an attractive alternative to basket extraction by sparing patients possible morbidity associated with the routine use of an UAS. In a prospective evaluation of UAS use in 359 patients, severe ureteral wall injury was noted in 13.3% of patients. 16
Laboratory studies have assessed some of the scientific rationale around a HiFr-LoPE setting during laser lithotripsy. HiFr-LoPE in comparison with conventional fragmentation results in fragments that are much smaller in size. 17,18 Sea et al. found that with increasing pulse energies, the degree of fragmentation and retropulsion also increased. 17 The smallest sized fragments were seen with the lowest pulse energy (i.e., 0.2 J/pulse). Traxer and colleagues discovered that for a given power level (total Watt), low-frequency/high-pulse energy settings led to a better fragmentation efficiency than HiFr-LoPE, but may produce bulky debris the removal of which can be time consuming. 18
A limitation of our report is the lack of direct comparison with conventional lithotripsy strategies such as fragmentation and retrieval. We used a variety of imaging modalities and acknowledge that if all patients had CT follow-up, the SFRs may differ. A longer follow-up period would allow assessment of any unknown long-term consequences of using high-frequency/energy settings. From our clinical experience so far, we have not encountered any, although the effect of such settings on heat generation during lithotripsy is under investigation by our group. Also, although it was our impression when using ultrahigh frequencies that stone breakdown was faster, we did not assess this in a controlled manner. Features such as the dual lithotripsy mode and technology that allows surgeon-specific/stone density-specific settings may result in more efficacious lithotripsy. One drawback of the 120 W system is that it requires a 46 amp power outlet, which may not be available in every operating room. This, along with its higher capital cost, may limit its adoption in some centers. Nevertheless, a recent survey by Dauw et al. 6 demonstrated that 41% of urologists already use high-power holmium lasers, suggesting these barriers may not be significant.
Given the ability to ablate stones into submillimeter fragments, we now offer staged URS and dusting as an alternative to percutaneous nephrolithotomy for stones measuring ≥2 cm, especially in patients at high risk for a percutaneous approach. Although we did not have full staghorn stones in our series, we consider these challenging for a dusting technique. Based on our experience of utilizing this Ho:YAG system, we have devised an intraoperative algorithm for dusting renal stones (Fig. 2). We use 0.2 J × 80 Hz (16 W) as our initial setting for dusting. Settings are then adjusted based on the relationship between stone density and presence of retropulsion. As a result of our experience, the preset system settings in the P120H now incorporates 0.2 J × 80 Hz as the initial setting for dusting. One factor to consider, for small stones, HiFr-LoPE settings, may lead to retropulsion and, therefore, minimal ablation efficiency. With fragmentation, while retropulsion may occur, if the laser is used to pin the stone against the tissue wall and accurately target the stone, ablation is effective in creating smaller fragments for retrieval. Another option in a calix is to switch to a high-frequency popcorning technique (such as 80 Hz × 0.5 J) to further degrade stones into submillimeter fragments, which may be more efficient than using poorly selected dusting settings. Our current protocol is to prescribe an alpha-adrenergic antagonist, regardless of whether a stent is placed, for 4 weeks to facilitate spontaneous fragment passage after URS.
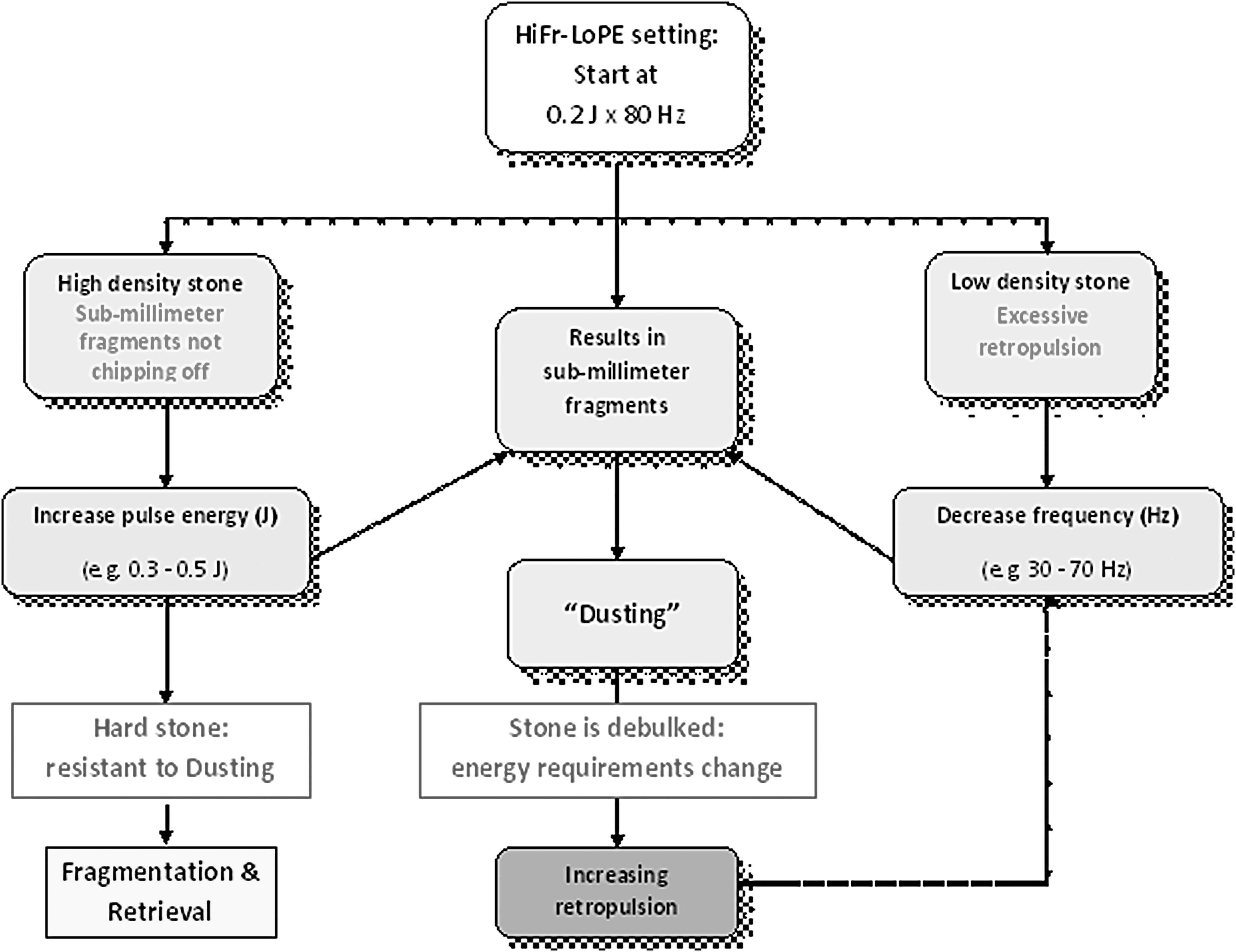
Schematic diagram outlining strategies for adjusting laser settings when utilizing a HiFr-LoPE dusting technique for renal stones during ureteroscopy. HiFr-LoPE = high-frequency and low-pulse energy.
The P120H, like other new generation holmium systems, allows alteration of the pulse width into short and long modes. Pulse width is the length of time during a pulse of energy where the amplitude of power is greater than 50% of maximum power. 10 In vitro studies show that a longer pulse width has a beneficial effect on dusting technique by decreasing retropulsion. 19 We did not assess the effect of pulse width as all our cases were done using short pulse width. However, there is emerging data to suggest that a longer pulse width has a protective effect on the fiber tip and reduces tip degradation and burnback. 7 The assessment of pulse width on dusting forms the basis of future work from our group.
In summary, we report the first outcomes on the utility of a 120 W Ho:YAG system that has been designed for stone dusting. We show that refinements in laser technology have expanded the ability to ablate urinary tract stones incorporating surgeon-specific settings and ultrahigh-pulse frequencies to open a new era for the dusting technique. If SFRs utilizing dusting are equivalent with retrieval, dusting may offer advantages of lower use of UAS, and thereby help reduce routine ureteral stenting or dwell times after URS. However, we found that not all stones were feasible for a dusting technique, and further study is needed to optimally define the role of this technique during holmium laser lithotripsy.
Footnotes
Author Disclosure Statement
Dr. Ghani is a consultant for Lumenis and Boston Scientific. No funding was received for this study.