
Abstract
Purpose:
Nephrolithiasis contributes significantly to the worldwide healthcare burden. Patient-reported outcome measures (PROMs) are widely recognized as important outcome measures for patient-centered care. We sought to summarize what is currently known about PROMs in urinary stone disease and to characterize use of PROMs in randomized controlled trials (RCTs) for nephrolithiasis.
Materials and Methods:
Health-related quality of life (HRQOL) in patients with nephrolithiasis is reviewed. A search of both MEDLINE and EMBASE databases for RCTs in nephrolithiasis was performed to assess utilization of PROMs in these trials. All searches were for articles published between 1990 and 2014. Two independent reviewers reviewed all abstracts to determine inclusion for full-text review, with disagreements reviewed by a separate arbitrator.
Results:
Validated methods for collecting PROMs include symptom diaries, pain scales, and validated HRQOL instruments. HRQOL is impacted in patients with nephrolithiasis and may be related to gender, proximity of a recent colic episode, or treatment modality. One validated instrument has been created in the nephrolithiasis population, while a treatment-specific questionnaire on ureteral stents has also been developed. PROMs are variably reported in RCTs for nephrolithiasis. Few trials utilize validated HRQOL instruments and none utilizes a disease-specific instrument.
Conclusions:
HRQOL is diminished in patients with urolithiasis, especially in times near to an acute stone event. Only one validated HRQOL instrument exists specific to nephrolithiasis. No validated instrument exists to assess the outcomes from different management options for renal and ureteral stones. Development of condition-specific PROMs instruments should aim to account for the heterogeneous and episodic nature of the disease and its treatment. Effective reporting of PROMs is lacking in the RCTs for nephrolithiasis. Future RCTs for urolithiasis standardize reporting of PROMs.
Introduction
N
Management strategies for active urinary stone disease, defined for the purposes of this article, as an existing renal or ureteral calculus are numerous and include observation, ureteroscopy and stone extraction or lithotripsy, extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), or open or laparoscopic stone surgery. Treatment decisions are based on patient and disease characteristics as well as physician and patient preference 5,6 While an abundance of literature exists in predicting elimination of urinary calculi based on stone properties, patient characteristics, and treatment modalities, there is a paucity of literature regarding patient's perspective into the success or failure of such treatments. As treatment decisions for patients with an active renal or ureteral calculus must be individualized, patient choice and therefore patient-reported outcome measures (PROMs) are important considerations in decision-making. We sought to evaluate the current status of PROMs assessment in nephrolithiasis, with a focus toward management of active urinary stone disease.
Traditional Outcome Measures in Nephrolithiasis
Classically, an “effective” treatment for ureteral or renal calculi rendered the patient stone free. However, as imaging modalities improved, identification of post-treatment fragments became more common. Thus, “stone-free rate” is at times a nebulous definition, as time to follow-up imaging and imaging modality can influence detection of residual stone fragments. 7 The concept of “clinically insignificant residual fragments” (CIRFs), often defined as residual fragments less than 4 mm in diameter, was introduced to help refine evaluation of treatment outcomes. These fragments are thought to be small enough to pass spontaneously. However, CIRFs may result in unplanned secondary treatment or contribute to future stone growth or recurrence rates. Thus, stone-free rates and CIRFs represent inexact outcome measures for evaluating treatment success in nephrolithiasis. 8
Given the complexities of treatment, patients may commonly require repeat treatments or multimodal therapy to achieve a satisfactory outcome. Such repeat interventions may lead to an increased risk of complications, rising medical costs, and higher time commitments of patients and providers. The efficiency quotient (EQ), introduced by Clayman, accounts for a varying number of interventions required to achieve the same goal. 9 However, the EQ is subject to the same pitfalls as stone-free rate and does not account for differences in treatment modalities.
Ultimately, such outcome measures are “stone centered,” with success being the outcome of the renal or ureteral calculus. However, medicine is witnessing a shift toward patient-centered outcomes, augmenting traditional outcome measures and encouraging patients to become active participants in decision-making. Therefore, more focus needs to be placed on the patient experience in assessing “success” of any treatment strategy.
Patient-Reported Outcomes: An Overview
Pain scales
Measurement of pain is limited by individual experience, while interpretation of pain may vary greatly between individuals. Validated pain scales may help to quantify the patient's experience with pain. Three common scales utilized for adults include the visual analog scale (VAS), numeric pain scale (NPS), and verbal rating scale (VRS). A VAS is shown as a 10 cm line with one extreme labeled as “no pain” and one labeled to describe intense pain (i.e., “worst pain imaginable”). Patients are simply asked to indicate where they feel their pain fits on the line. An NPS asks patients to rate pain by number, with lower numbers indicating lower pain. Finally, a VRS asks patients to rate pain based on common pain descriptors (i.e., “mild,” “moderate,” “severe”). While all three have been validated and show reproducible reliability, VAS and NPS have been shown to be more sensitive to changes in pain than VRS. 10 Because each pain scale possesses certain strengths and weaknesses, it is important not only to utilize a standardized pain scale in studying disease or treatment but also to indicate which type of scale was utilized.
Health-related quality of life
Measurements of qualitative outcomes, such as a patient's perception of their own health, can be even more difficult to measure than pain. The development of validated questionnaires, often referred to as “validated instruments,” has allowed for more objective assessments of quality of life. 11 Questionnaires provide a sense of disease burden or suffering. Questions are often organized in a way to assess several domains of a patient's life, such as physical or emotional functioning or mood. Instruments may be generic or disease specific. Generic instruments apply to a wide range of health conditions and focus on broad categories of functioning, such as pain, general well-being, and socialization. In contrast, disease-specific instruments are developed to focus on a single condition or a narrow range of conditions. 12 Ideally, such instruments should be accessible to and completed by patients to yield reproducible results and clinically significant changes over time. 13,14 Initial instruments may be shortened to distil content, eliminate redundancy, and reduce time taken to complete the questionnaire. 11
Questionnaires are often used to quantify disease burden to provide reference for initial management discussions and evaluate management success in follow-up. Such instruments also serve as valuable research tools. 11,13 Disease-specific instruments play a major role in care of urologic disease. As of 2010, there were 16 instruments specific for prostate cancer, 11 for benign prostatic hyperplasia, and 24 for urinary incontinence. 15 At present, however, there exists only one, recently introduced, health-related quality of life (HRQOL) instrument specific for nephrolithiasis, and one for patients with ureteral stents. 16,17
Other PROMs
Patients and practitioners alike may also find utility in quantifying other important aspects of the patient's journey. For kidney stones, this may include number of renal colic episodes, emergency department visits, or other measurable events such as hematuria or incontinence. Convalescence expressed in time taken to return to normal activities is commonly cited, especially in the realm of minimally invasive surgery. 18,19 Patient reporting of events may be hindered by patient compliance and recall bias. Patient diaries, which encourage prospective recording of events, can help to improve accuracy of patient reporting as has been shown in studies on incontinence. 20 Although not studied specifically in nephrolithiasis, a prospective diary from patients following an acute stone episode or lithotripsy could be important for accessing treatment success or guiding further therapies.
Patient-Reported Outcomes for Nephrolithiasis
While much discussion of PROMs has revolved around HRQOL, PROMs encompass any portion of the patient's experience with the condition in question, including self-reported pain scales, indications of frequency of events of interest (i.e., incontinence, renal colic, hematuria), time to return to “normal” activities (i.e., driving, exercise, work), or more detailed quality-of-life assessments (i.e., functioning on various physical or emotional scales). 21
The effect of nephrolithiasis on quality of life
Several studies have documented the impact of nephrolithiasis on HRQOL. As a disease-specific instrument for nephrolithiasis was released only in 2013, earlier studies relied on nonspecific instruments. The most common generic instrument is the SF-36, which is often considered the “gold standard” for measurements of general health and well-being. The instrument encompasses eight health domains (bodily pain, role-physical, physical functioning, general health, vitality, social functioning, role-emotional, mental health) with 36 items and can be completed in less than 10 minutes. 15
Several groups have shown decreased HRQOL in recurrent stone formers compared with either a cohort of healthy controls or general norms for the validated instrument in question. 22 –25 Importantly, patients in these studies were recruited from outpatient stone clinics and therefore may not adequately capture distress from acute stone events. Measuring PROMs in nephrolithiasis is challenging given the episodic nature of the disease. Other episodic illnesses have been studied in this manner, including migraines, asthma, Meniere's disease, epilepsy and angina. 26 –30 Similar to many of these conditions, patients with nephrolithiasis may be mostly asymptomatic with intermittent episodes of acute renal colic. Bensalah and colleagues showed that HRQOL measures differed based on the timing of most previous stone episode. Those patients with an acute renal colic episode within 1 month of evaluation had decreased emotional health, pain, and general health scores, while those with a more distant renal colic episode experienced only a decrease in general health. 23 Furthermore, recurrent renal colic episodes have been shown to impact HRQOL in multiple domains within the first month of an acute episode of colic and frequency of stone events also negatively impacts HRQOL. 22,23,31 However, even after a resolution of the acute episode, general health measures were still lower, indicating that recurrent stone formers appear to feel less well in themselves even at baseline. 23 Age, obesity, and mental illness have been shown to be significant predictors of poor HRQOL in recurrent stone formers and may serve as confounding factors in the assessment of HRQOL in nephrolithiasis. In addition, women appeared to be affected to a greater degree than men, especially in physical functioning and vitality domains. 23 –25,31 Although certain subsets of stone formers are at much higher risk for stone events, few studies have addressed specific phenotypes of recurrent stone formers. Modersitzki and colleagues evaluated the quality of life of cystine stone formers using SF-36. Cystine stone formers, compared with a noncystine group, were at higher risk for more frequent and severe stone events resulting in a greater negative impact on HRQOL compared with noncystine stone formers. 31
Treatments for stone disease also seem to influence HRQOL. Bensalah and colleagues showed treatment type can lead to variations in HRQOL, with PCNL and ureteroscopy (URS) affecting patients to a greater degree than SWL. In addition, the use of a stent in any procedure resulted in worse HRQOL scores. 23 Arafa and Rabah studied patients undergoing SWL specifically and found decreased HRQOL compared with controls. 32 Several studies have shown worse HRQOL scores in patients undergoing multiple interventions. 23,25 Furthermore, self-reported complications and visits to the emergency department are also associated with decreased HRQOL scores. 25 The success of stone treatments, as traditionally defined by stone-free rates, may also impact subsequent HRQOL of these patients. Sahin and colleagues evaluated the quality of life in patients with residual fragments after SWL. Patients with residual fragments <4 mm had a lower rate of symptomatic residual fragments requiring subsequent interventions and higher HRQOL scores in all eight domains at 3 months compared with those patients with larger residual fragments. 33 This study suggests a relationship between traditional measures of success and PROMs in nephrolithiasis, which merits further investigation.
In addition to expected impact of nephrolithiasis on physical parameters, recurrent nephrolithiasis also appears to significantly impact patient mood. Depressive symptoms and nephrolithiasis are associated in up to 30% of recurrent stone formers. 34 Interestingly, one study has shown an increase in symptomatic nephrolithiasis in patients who had stressful life events (i.e., death in family, marriage, accident, personal illness, etc.) within a year of their episode and raise questions of causality of nephrolithiasis and mood. 35
Nephrolithiasis is now widely recognized as an increasingly common problem in children. 36 Accordingly, in an emerging field, there is little known regarding HRQOL in children with nephrolithiasis, and disease-specific HRQOL instruments relating to nephrolithiasis have not been validated in children. One compelling study assessed HRQOL in bladder exstrophy patients, a condition with well-documented lifelong morbidity, and utilized children from the pediatric stone clinic as a comparison group. 37 Children with nephrolithiasis scored worse on physical functioning and overall HRQOL using the pediatric-specific Pediatric Quality of Life Inventory, revealing a high impact of HRQOL on these children, even when compared with a population with a significant congenital abnormality. Notably, assessment of HRQOL in children is layered with additional complexity as validated HRQOL instruments are often age specific and may be administered to children, their parents, or both depending on the instrument utilized. 38
Measuring patient-reported outcomes in nephrolithiasis
Similarly, patients may only experience symptoms following an intervention. Thus, when evaluating quality of life in nephrolithiasis, one must consider that results may be influenced by timing of a stone event. Development of disease-specific questionnaires can often provide perspective that may be otherwise missed by the general health instruments such as the SF-36 utilized in the above literature. For instance, SF-36 has been shown to be a poor instrument for longitudinally following patients with nephrolithiasis. 39
Currently, there is a paucity of disease-specific instruments for nephrolithiasis. Joshi and colleagues were the first to attempt to address this need by introducing the Ureteral Stent Symptom Questionnaire (USSQ) after it had long been recognized that indwelling ureteral stents have a significant detrimental impact on HRQOL. 17 This validated questionnaire has been used in numerous studies to evaluate the impact of ureteral stents on HRQOL as well as to assess management of ureteral stent symptoms with either medical therapy or ureteral stent modifications. 40 –42 Of note, the USSQ should be viewed as an intervention-specific as opposed to disease-specific questionnaire, as it focuses on stent-related symptoms and thus could be applicable to a patient with a ureteral stent for any indication.
Penniston and Nakada have created the Wisconsin Stone QOL instrument, the first tool to attempt to evaluate HRQOL in general for stone formers. This questionnaire was developed with rigorous methodology within the setting of recurrent stone formers identified in the author's stone clinic. On internal validation, those patients with active stone disease scored worse than patients currently stone free. 16 The development of a disease-specific urolithiasis questionnaire is an important step in the evaluation of PROMs in nephrolithiasis although additional study is warranted. While the Wisconsin Stone QOL instrument is valid among recurrent stone formers, further investigation into the evaluation of PROMs in the acute setting or in comparison of different management strategies is needed. Furthermore, the spectrum of “nephrolithiasis” is quite varied and heterogeneous as the presentations of ureteral and renal calculi can vary greatly. As such, development of instruments to evaluate these subsets of stone disease would be useful.
PROMs in Current Urolithiasis Literature
Given the importance of PROMs in accessing overall patient outcome and the difficulty in measuring such outcomes, we sought to critically and systematically review the current practice of evaluating PROMs in randomized controlled trials (RCTs) pertaining to nephrolithiasis. RCTs are classically the “gold standard” of comparing various treatment options in medicine and offer a prime opportunity to prospectively capture PROMs at the onset of randomization. In the management of active urinary stone disease, RCTs can be divided into three comparisons: observation vs surgical or dissolution therapy for renal stones, medical expulsive therapy (MET), and surgical therapies. Given the uncertainty regarding treatment effectiveness as measured by traditional methods in literature surrounding both MET 43 –45 and various surgical modalities, 46 especially when comparing SWL and URS, we feel reporting and comparing PROMs may offer useful insight into patient-centered benefits seen among these various therapeutic options.
To accomplish this review, we performed EMBASE and MEDLINE searches on RCTs for nephrolithiasis from 2000 to 2015, including full-text articles that focused on primary treatment for nephrolithiasis, as opposed to adjunct treatment options such as alpha-blockers after lithotripsy. MeSH search terms for “nephrolithiasis” and “ureteral calculus” were utilized, as were terms for treatment modalities of “percutaneous nephrostomy,” “lithotripsy,” “ureteroscopy,” “tamsulosin,” “adrenergic alpha-antagonists,” and “calcium-channel blockers.” While we acknowledge the importance of assessing urinary stent symptoms, we considered ureteral stenting an adjunct treatment and thus beyond the scope of this review. A total of 395 abstracts were identified in the initial search. Of these, 106 abstracts were identified by the authors to be further explored. Forty-two articles were excluded as no full text was available and one excluded as it was not a true RCT. No duplicates were noted and a total of 63 full-text articles were reviewed, including two studies identified in additional searches before 2000. PROMs assessments were characterized in all trials, including prospective patient diaries for symptom reporting, validated pain scales, and validated HRQOL instruments. Figure 1 displays use of PROMs in observational, surgical and medical trials for nephrolithaisis.
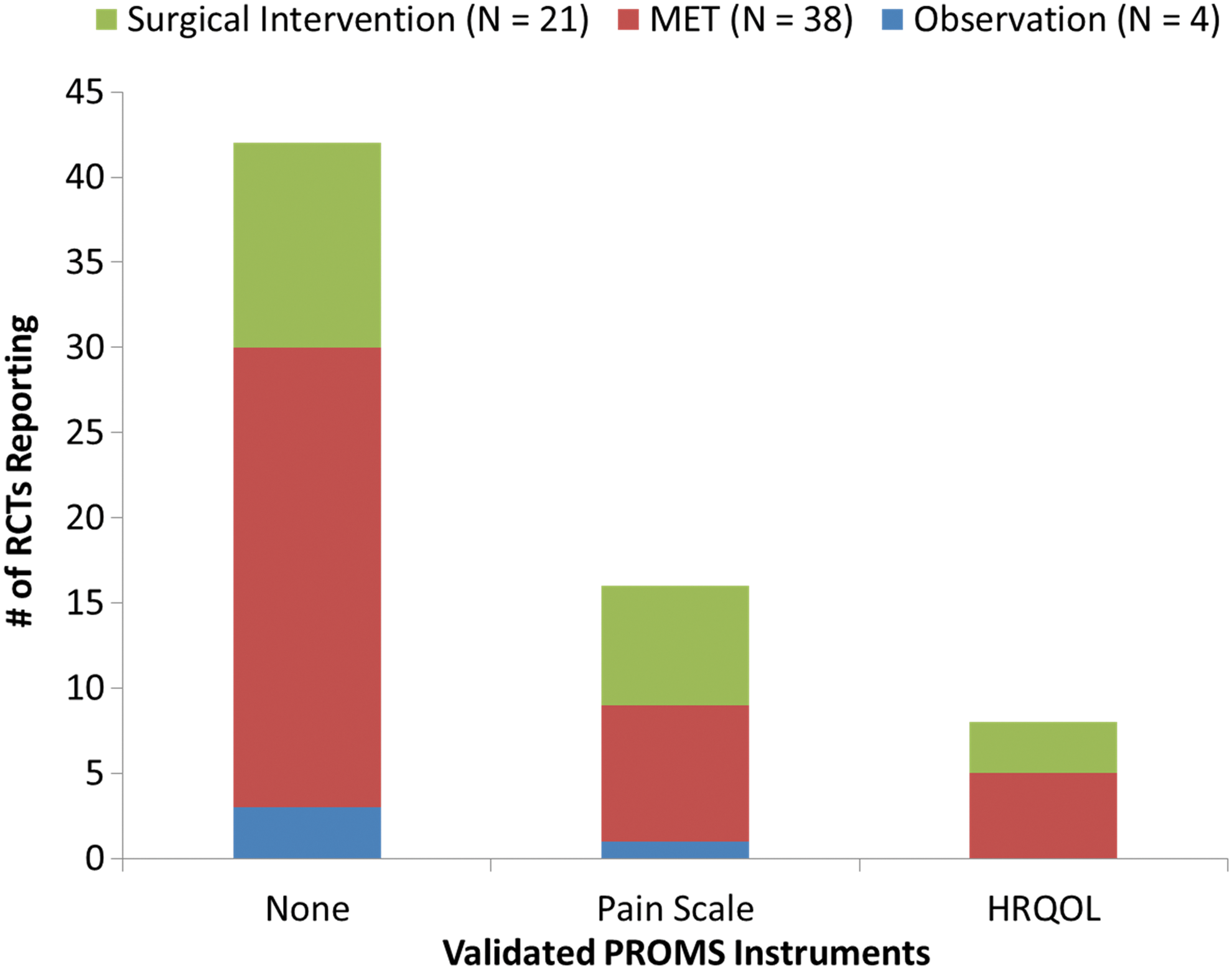
Use of validated PROMs instruments (pain scales, HRQOL instruments) in RCTs for observation, MET, and surgical intervention. HRQOL = health-related quality of life; MET = medical expulsive therapy; PROMs = patient-reported outcome measures; RCT = randomized controlled trial.
Observation vs treatment
Few studies exist pertaining to observational or medical management of asymptomatic nephrolithiasis. Four studies found in our review are summarized in Table 1. Importantly, as observational management is intended to take into consideration the adverse impact of treatment modalities balanced against the risk of future symptoms, one would expect at least a secondary focus on PROMs in this cohort of studies, which is not the case. While no studies utilized validated pain scales, one study did utilize a validated HRQOL instrument.
1. Keeley Jr, FX, Tilling K, Elves A, et al. Preliminary results of a randomized controlled trial of prophylactic shock wave lithotripsy for small asymptomatic renal calyceal stones. BJU Int 2001;87:1–8.
2. Yuruk E, Binbay M, Sari E, et al. A prospective, randomized trial of management for asymptomatic lower pole calculi. J Urol 2010;183:1424–1428.
3. Elderwy AA, Kurkar A, Hussein A, et al. Dissolution therapy versus shock wave lithotripsy for radiolucent renal stones in children: A prospective study. J Urol 2014;191:1491–1495.
4. Sener NC, Bas O, Sener E, et al. Asymptomatic lower pole small renal stones: Shock wave lithotripsy, flexible URS, or observation? A prospective randomized trial. Urology 2015;85:33–37.
SWL = extracorporeal shock wave lithotripsy; NHP = Notthingham Health Profile; OBS = observation; PCNL = percutaneous nephrolithotomy; PRO = patient-reported outcomes; SFR = stone-free rate; URS = ureteroscopy.
Medical therapy
Management of ureteral calculi includes options for expectant management, MET, SWL, or URS. 47 MET, while previously well accepted as efficacious in patients with ureteral calculi, has recently been called into question with the results of the SUSPEND trial. 44,45 The reporting of PROMs in 38 trials pertaining to MET is summarized in Table 2. Primary outcome measures in all studies were appropriately related to the stone expulsion rate. All studies collected patient-reported side effects of medications. However, rarely were these done so in a prospective or validated manner. Only five studies did so in a prospective manner using a patient-maintained diary at the onset of randomization. Eight studies utilized some form of validated pain scale, although variation of pain scales would likely make comparative assessments between studies difficult. Ultimately, five studies utilized validated instruments for HRQOL. One study utilized the International Index of Erectile Function as the trial compared tamsulosin and tadalafil for MET. Thus, the applicability of this instrument for assessing nephrolithiasis symptoms specifically may be called into question. Only Sur and colleagues captured PROMs by prospective patient diary as well as validated pain and HRQOL instruments, as the brief pain inventory utilized assesses both pain and HRQOL. 48 None of the three pediatric studies utilized prospective patient diaries, pain scales, or validated HRQOL instruments.
1. Cooper JT, Stack GM, Cooper TP. Intensive medical management of ureteral calculi. Urology 2000;56:575–578.
2. Dellabella M, Milanese G, Muzzonigro G. Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. J Urol 2003;170:2202–2205.
3. Porpiglia F, Ghignone G, Fiori C, et al. Nifedipine versus tamsulosin for the management of lower ureteral stones. J Urol 2004;172:568–571.
4. Dellabella M, Milanese G, Muzzonigro G. Medical-expulsive therapy for distal ureterolithiasis: Randomized prospective study on role of corticosteroids used in combination with tamsulosin-simplified treatment regimen and health-related quality of life. Urology 2005;66:712–715.
5. Dellabella M, Milanese G, Muzzonigro G. Randomized trial of the efficacy of tamsulosin, nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral calculi. J Urol 2005;174:167–172.
6. Resim S, Ekerbicer H, Ciftci A. Effect of tamsulosin on the number and intensity of ureteral colic in patients with lower ureteral calculus. Int J Urol 2005;12:615–620.
7. Liatsikos EN, Katsakiori PF, Assimakopoulos K, et al. Doxazosin for the management of distal-ureteral stones. J Endourol 2007;21:538–541.
8. Erturhan S, Erbagci A, Yagci F, et al. Comparative evaluation of efficacy of use of tamsulosin and/or tolterodine for medical treatment of distal ureteral stones. Urology 2007;69:633–636.
9. Pedro RN, Hinck B, Hendlin K, et al. Alfuzosin stone expulsion therapy for distal ureteral calculi: A double-blind, placebo controlled study. J Urol 2008;179:2244–2247.
10. Porpiglia F, Fiori C, Ghignone G, et al. A second cycle of tamsulosin in patients with distal ureteric stones: A prospective randomized trial. BJU Int 2009;103:1700–1703.
11. Agrawal M, Gupta M, Gupta A, et al. Prospective randomized trial comparing efficacy of alfuzosin and tamsulosin in management of lower ureteral stones. Urology 2009;73:706–709.
12. Aydogdu O, Burgu B, Gucuk A, et al. Effectiveness of doxazosin in treatment of distal ureteral stones in children. J Urol 2009;182:2880–2884.
13. Ferre RM, Wasielewski JN, Strout TD, et al. Tamsulosin for ureteral stones in the emergency department: A randomized, controlled trial. Ann Emerg Med 2009;54:432–439, 439.e1.
14. Hermanns T, Sauermann P, Rufibach K, et al. Is there a role for tamsulosin in the treatment of distal ureteral stones of 7 mm or less? Results of a randomised, double-blind, placebo-controlled trial. Eur Urol 2009;56:407–412.
15. Sun X, He L, Ge W, et al. Efficacy of selective alpha1D-blocker naftopidil as medical expulsive therapy for distal ureteral stones. J Urol 2009;181:1716–1720.
16. Al-Ansari A, Al-Naimi A, Alobaidy A, et al. Efficacy of tamsulosin in the management of lower ureteral stones: A randomized double-blind placebo-controlled study of 100 patients. Urology 2010;75:4–7.
17. Vincendeau S, Bellissant E, Houlgatte A, et al. Tamsulosin hydrochloride vs placebo for management of distal ureteral stones: A multicentric, randomized, double-blind trial. Arch Intern Med 2010;170:2021–2027.
18. Abdel-Meguid TA, Tayib A, Al-Sayyad A. Tamsulosin to treat uncomplicated distal ureteral calculi: A double blind randomized placebo-controlled trial. Can J Urol 2010;17:5178–5183.
19. Kaneko T, Matsushima H, Morimoto H, et al. Efficacy of low dose tamsulosin in medical expulsive therapy for ureteral stones in Japanese male patients: A randomized controlled study. Int J Urol 2010;17:462–465.
20. Gurbuz MC, Polat H, Canat L, et al. Efficacy of three different alpha 1-adrenergic blockers and hyoscine N-butylbromide for distal ureteral stones. Int Braz J Urol 2011;37:195–200.
21. Itoh Y, Okada A, Yasui T, et al. Efficacy of selective alpha1A adrenoceptor antagonist silodosin in the medical expulsive therapy for ureteral stones. Int J Urol 2011;18:672–674.
22. Ye Z, Yang H, Li H, et al. A multicentre, prospective, randomized trial: Comparative efficacy of tamsulosin and nifedipine in medical expulsive therapy for distal ureteric stones with renal colic. BJU Int 2011;108:276–279.
23. Tsuzaka Y, Matsushima H, Kaneko T, et al. Naftopidil vs silodosin in medical expulsive therapy for ureteral stones: A randomized controlled study in Japanese male patients. Int J Urol 2011;18:792–795.
24. Mokhless I, Zahran AR, Youssif M, et al. Tamsulosin for the management of distal ureteral stones in children: A prospective randomized study. J Pediatr Urol 2012;8:544–548.
25. Erturhan S, Bayrak O, Sarica K, et al. Efficacy of medical expulsive treatment with doxazosin in pediatric patients. Urology 2013;81:640–643.
26. Jayant K, Agrawal R, Agrawal S. Tamsulosin versus tamsulosin plus tadalafil as medical expulsive therapy for lower ureteric stones: A randomized controlled trial. Int J Urol 2014;21:1012–1015.
27. Alizadeh M, Magsudi M. The effect of tamsulosin in the medical treatment of distal ureteral stones. Glob J Health Sci 2014;6:44–48.
28. Balci M, Tuncel A, Aydin O, et al. Tamsulosin versus nifedipin in medical expulsive therapy for distal ureteral stones and the predictive value of Hounsfield unit in stone expulsion. Ren Fail 2014;36:1541–1544.
29. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: A multicentre, randomised, placebo-controlled trial. Lancet 2015;386:341–349.
30. Sur RL, Shore N, L'Esperance J, et al. Silodosin to facilitate passage of ureteral stones: A multi-institutional, randomized, double-blinded, placebo-controlled trial. Eur Urol 2015;67:959–964.
31. Kumar S, Jayant K, Agrawal S, et al. Comparative efficacy of tamsulosin versus tamsulosin with tadalafil in combination with prednisolone for the medical expulsive therapy of lower ureteric stones: A randomized trial. Korean J Urol 2014;55:196–200.
32. Devi NM, Monica KS, Medhabati M. Tamsulosin vs naftopidil in medical expulsive therapy for ureteral stones: a randomized controlled study. Ind Med Gaz 2015;5:187.
33. Lal S, Charak K, Chakravarti S, et al. Efficacy of nifedipine and alfuzosin in the management of distal ureteric stones: A randomized, controlled study. Indian J Urol 2014;30:387–391.
34. Gandhi HR, Agrawal C. The efficacy of tamsulosin vs. nifedipine for the medical expulsive therapy of distal ureteric stones: A randomised clinical trial. Arab J Urol 2013;11:405–410.
35. Gupta S, Lodh B, Singh AK, et al. Comparing the efficacy of tamsulosin and silodosin in the medical expulsion therapy for ureteral calculi. J Clin Diagn Res 2013;7:1672–1674.
36. Ibrahim AK, Mahmood IH, Mahmood NS. Efficacy and safety of tamsulosin vs. alfuzosin as medical expulsive therapy for ureteric stones. Arab J Urol 2013;11:142–147.
37. Kumar S, Kurdia KC, Ganesamoni R, et al. Randomized controlled trial to compare the safety and efficacy of naftopidil and tamsulosin as medical expulsive therapy in combination with prednisolone for distal ureteral stones. Korean J Urol 2013;54:311–315.
38. Ahmed A.-f. A.-m., Al-sayed A.-y. S. Tamsulosin versus alfuzosin in the treatment of patients with distal ureteral stones: Prospective, randomized, comparative study. Korean J Urol 2010;51:193–197.
Pediatric patients.
BPI = Brief Pain Inventory; EQ-5D = EuroQOL questionnaire; IIEF-5 = International Index of Erectile Function (trial utilized tadalafil); NPS = numeric pain scale; SER = stone expulsion rate; SF-36 = short form 36; TTSE = time to stone expulsion; VAS = visual analog scale.
Surgical interventions
As previously mentioned, URS and SWL are both options for patients with ureteral calculi failing expectant management or MET. In addition, both modalities are options for smaller renal stones, while PCNL as well as laparoscopic or open stone surgeries may be considered for larger renal calculi. Table 3 summarizes 21 trials found in our review comparing surgical modalities for management of ureteral or renal calculi. Primary outcome in all trials was stone-free rate, except one trial for which primary outcome was not specified. Seven trials specified patient symptom collection, although prospective collection of patient symptom diaries was not specified in any trial. Likewise, seven trials utilized validated pain scales. Finally, validated HRQOL instruments were utilized in only three of the studies. While patient satisfaction was noted in several studies and is an important aspect of patient care, the accuracy and precision of such an assessment must be scrutinized, especially in the setting of a physician-delivered binary (i.e., “yes/no”) response, as opposed to a graduated system of measurement such as a Likert scale. Neither of the two pediatric studies in this group utilized validated pain or HRQOL instruments.
1. Meretyk S, Gofrit ON, Gafni O, et al. Complete staghorn calculi: Random prospective comparison between extracorporeal shock wave lithotripsy monotherapy and combined with percutaneous nephrostolithotomy. J Urol 1997;157:780–786.
2. Peschel R, Janetschek G, Bartsch G. Extracorporeal shock wave lithotripsy versus ureteroscopy for distal ureteral calculi: A prospective randomized study. J Urol 1999;162:1909–1912.
3. Albala DM, Assimos DG, Clayman RV, et al. Lower pole I: A prospective randomized trial of extracorporeal shock wave lithotripsy and percutaneous nephrostolithotomy for lower pole nephrolithiasis-initial results. J Urol 2001;166:2072–2080.
4. Verze P, Imbimbo C, Cancelmo G, et al. Extracorporeal shockwave lithotripsy vs ureteroscopy as first-line therapy for patients with single, distal ureteric stones: A prospective randomized study. BJU Int 2010;106:1748–1752.
5. Pearle MS, Nadler R, Bercowsky E, et al. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopy for management of distal ureteral calculi. J Urol 2001;166:1255–1260.
6. Al-Kohlany KM, Shokeir AA, Mosbah A, et al. Treatment of complete staghorn stones: A prospective randomized comparison of open surgery versus percutaneous nephrolithotomy. J Urol 2005;173:469–473.
7. Pearle MS., Lingeman JE, Leveillee R, et al. Prospective, randomized trial comparing shock wave lithotripsy and ureteroscopy for lower pole caliceal calculi 1 cm or less. J Urol 2005;173:2005–2009.
8. Lee YH, Tsai JY, Jiaan BP, et al. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopic lithotripsy for management of large upper third ureteral stones. Urology 2006;67:480–484.
9. Salem HK. A prospective randomized study comparing shock wave lithotripsy and semirigid ureteroscopy for the management of proximal ureteral calculi. Urology 2009;74:1216–1221.
10. Basiri A, Zare S, Tabibi A, et al. A multicenter, randomized, controlled trial of transureteral and shock wave lithotripsy—which is the best minimally invasive modality to treat distal ureteral calculi in children? J Urol 2010;184:1106–1109.
11. Deem S, Defade B, Modak A, et al. Percutaneous nephrolithotomy versus extracorporeal shock wave lithotripsy for moderate sized kidney stones. Urology 2011;78:739–743.
12. Lopes Neto AC, Korkes F, Silva 2nd, JL, et al. Prospective randomized study of treatment of large proximal ureteral stones: Extracorporeal shock wave lithotripsy versus ureterolithotripsy versus laparoscopy. J Urol 2012;187:164–168.
13. Uguz S, Senkul T, Soydan H, et al. Immediate or delayed SWL in ureteric stones: A prospective and randomized study. Urol Res 2012;40:739–744.
14. Fang YQ, Qiu JG, Wang DJ, et al. Comparative study on ureteroscopic lithotripsy and laparoscopic ureterolithotomy for treatment of unilateral upper ureteral stones. Acta Cir Bras 2012;27:266–270.
15. Yang Z, Song L, Xie D, et al. Comparative study of outcome in treating upper ureteral impacted stones using minimally invasive percutaneous nephrolithotomy with aid of patented system or transurethral ureteroscopy. Urology 2012;80:1192–1197.
16. Karami H, Mazloomfard MM, Lotfi B, et al. Ultrasonography-guided PNL in comparison with laparoscopic ureterolithotomy in the management of large proximal ureteral stone. Int Braz J Urol 2013;39:22–28.
17. Sabnis RB, Ganesamoni R, Doshi A, et al. Micropercutaneous nephrolithotomy (microperc) vs retrograde intrarenal surgery for the management of small renal calculi: A randomized controlled trial. BJU Int 2013;112:355–361.
18. Mokhless IA, Abdeldaeim HM, Saad A, et al. Retrograde intrarenal surgery monotherapy versus shock wave lithotripsy for stones 10 to 20 mm in preschool children: A prospective, randomized study. J Urol 2014;191:1496–1499.
19. Li S, Liu TZ, Wang XH, et al. Randomized controlled trial comparing retroperitoneal laparoscopic pyelolithotomy versus percutaneous nephrolithotomy for the treatment of large renal pelvic calculi: A pilot study. J Endourol 2014;28:946–950.
20. Kumar A, Kumar N, Vasudeva P, et al. A prospective, randomized comparison of shock wave lithotripsy, retrograde intrarenal surgery and miniperc for treatment of 1 to 2 cm radiolucent lower calyceal renal calculi: A single center experience. J Urol 2015;193:160–164.
21. Garg M, Singh V, Sinha RJ, et al. Prospective randomized comparison of open versus transperitoneal laparoscopic ureterolithotomy: Experience of a single center from Northern India. Curr Urol 2013;7:83–89.
Pediatric patients.
SWL immediate vs delayed.
LSS = laparoscopic stone surgery; NS = not specified; OSS = open stone surgery; SF-36 = short form 36 (RAND); SF-8 = short form 8.
HRQOL instruments in RCTs for nephrolithiasis
While stone-free status was appropriately the primary outcome for the vast majority of these studies, only 9 of the 63 studies reviewed utilized a validated HRQOL instrument as part of the secondary outcome assessment. Of these instruments, the EuroQOL questionnaire was utilized most commonly, in three studies, indicating the heterogeneity in choice of instruments by researchers. For surgical procedures, most studies showed a significant improvement in HRQOL compared with preoperative assessment, although little difference was noted when comparing differences in HRQOL between groups. Likewise, the majority of studies evaluating MET or observational management for nephrolithiasis failed to show a difference in HRQOL between study groups. These findings may indicate no true difference in HRQOL outcomes between study groups. However, the sensitivity of general domain instruments to capture significant changes in nephrolithiasis-specific parameters is unknown. As noted previously, the validity of following HRQOL of patients with nephrolithiasis longitudinally with the SF-36 has been called into question. 39
Whether the same is true for other general HRQOL instruments is unknown, although the need for utilization of nephrolithiasis-specific HRQOL instruments in future RCTs for nephrolithiasis is underscored by the above findings.
PROMs Reporting in RCTs for Active Urinary Stone Disease: A Summary
Of the 63 trials reviewed, 42 (67%) did not utilize any validated PROMs in secondary outcomes. Validated pain instruments were utilized in 15 (24%) studies while other validated HRQOL instruments were only utilized in 8 (13%) studies. Studies for MET and surgical intervention showed similar rates of both pain and HRQOL instrument utilization. Therefore, PROMs do not appear to be systematically assessed in most RCTs for active urinary stone disease, which has implications in the interpretation of the results of RCTs in the context of patient experience.
PROMs in Nephrolithiasis: How Can We Do Better?
Current knowledge of HRQOL in patients with nephrolithiasis is derived from small single-institution studies. The Patient-Reported Outcomes Measurement Information System (PROMIS) is a multi-institutional, multidisciplinary study group with the aim to evaluate PROMs across a wide range of health conditions. 49 This initiative could be a powerful tool in the understanding of HRQOL in nephrolithiasis.
HRQOL instruments may be used as both clinical and research tools. For instance, a urologist may assess success of treatment after a transurethral resection of the prostate using the International Prostate Symptom Score, while a researcher may use the same instrument to compare different treatment modalities. 50 Only one disease-specific questionnaire currently exists, validated in patients presenting to a multidisciplinary kidney stone clinic. Aside from the obvious research applications, development of future disease-specific questionnaires with focus on acute stone events and/or treatment modalities could serve multiple clinical functions. Such instruments could be utilized to assess failure of MET by symptoms or be applied, once validated, to help guide management decisions for minimally symptomatic stones in the kidney. Applying the current Wisconsin Stone QOL questionnaire in a kidney stone prevention clinic could help the clinician and patient assess and balance dietary or medical preventative measures against current stone risk.
PROMs assessments have been applied in varying degrees to comparative research trials for treatment modalities of nephrolithiasis. Utilization of existing PROMs as well as development of new, disease- or even treatment-specific instruments will help to provide a more robust understanding of treatment effects in patients with nephrolithiasis. Although performed prospectively, assessment of pain, renal colic events, and treatment or medication side effects are limited by recall bias if only performed at certain follow-up interval points. Prospectively maintained symptom diaries could help to alleviate this recall bias. Furthermore, comparison of pain or other symptoms between patients is limited by patient perception and definitions of pain. Thus, secondary outcome measures could be improved by application of standardized instruments or pain scales to evenly compare outcomes between patient groups. Finally, an appropriately designed instrument could provide comparative analysis to differing treatment modalities, such as SWL and URS, where primary outcomes in RCTs have been shown to be equivalent.
Conclusions
Nephrolithiasis results in significant distress, pain, and measurable decline in quality of life during a stone-related event. Furthermore, recurrent stone formers appear to have more subtle decreases in HRQOL even between stone-related events. The heterogeneity of urolithiasis and variety of management strategies require an individualized approach depending on patient presentation, physician experience, and hospital resources. To this end, measurement of patient-reported outcomes is essential to assessing management success and patient satisfaction. However, reporting of PROMs in the current urolithiasis literature, especially for comparative effectiveness studies, is lacking in both frequency and rigor. One validated instrument for HRQOL in urolithiasis currently exists as an important asset in evaluating recurrent stone formers. However, the utility of this instrument in evaluating treatment outcomes remains to be proven. Based on our review of the current literature surrounding PROMs in nephrolithiasis, we can make several recommendations: (1) Given the impact of an acute stone-related event on HRQOL, clinicians may wish to utilize pain scales or standardized instruments to monitor management success. (2) Investigators should strive to report PROMs in a standardized, easily interpretable manner, especially during RCTs for urinary stone disease. Such reporting could involve patient diaries of key events, standardized pain scales, and/or validated HRQOL instruments. (3) Current PROMs instruments should be further studied and refined. Additional PROMs instruments may prove useful in assessing specific aspects of the heterogeneous spectrum of nephrolithiasis, including acute management, surgical intervention, and preventative measures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.