
Abstract
Objective:
We investigated the surgical efficiency and cutoff criteria to determine whether retrograde intrarenal surgery (RIRS) or supine miniaturized percutaneous nephrolithotomy (MPCNL) is appropriate for managing renal stones with a mean size >10 mm.
Materials and Methods:
Data of a single session RIRS or supine MPCNL were collected in a prospective, observational study. Change point analysis with a cumulative sum of ordered value of fragmentation efficiency and stone size was used to detect the point at which the statistical properties of a sequence of observation change.
Results:
A total of 310 RIRS and 66 MPCNL cases were included. No differences in patient characteristics were observed between the groups. Stone burden, fragmentation efficiency, stone distribution, and the presence of staghorn stones were higher in the MPCNL group than the RIRS group. Stone-free rates and complication rates were not different. The fragmentation efficiency increased to 40.4 mL/min, at which the stone size in the RIRS group was 19.1 mm. The efficiency was decreased after the peak point and became the same at the stone size 30 mm with 10 mm in RIRS group. The fragmentation efficiency in the MPCNL group continuously increased until the size of 35.1 mm.
Conclusions:
RIRS shows the highest efficiency at the maximal diameter of 19.1 mm and volume of 15,000 mm3. The acceptable level of stone size and volume for RIRS would be 30.0 mm and 27,000 mm3, respectively. However, MPCNL would be appropriate when surgeons want to get high surgical efficiency for renal stone >21.6 mm instead of RIRS.
Introduction
T
RIRS has gained much attention in the management of renal stones because of its minimal invasiveness. 4 The European Association of Urology guidelines recommend that RIRS should be the standard treatment option for medium-sized renal stones <20 mm. 5 In addition, the guidelines and some previous investigations allowed for the possibility that RIRS can be a good option for renal stones >20 mm depending on the surgeons' skill. 6 This controversy indicates that surgical efficiency would decrease with an increase in stone size. However, there is no analytic investigation on the upper limit of renal stones.
Basically, PCNL has been the treatment of choice for renal stones >20 mm because of its high stone-free rates. 7 However, MPCNL has been introduced to manage mid-to-large-sized renal stones, considering the lower risk of morbidities than those of conventional PCNL. 8 The MPCNL using 10 to 18F sheaths shows surgical outcomes comparable with those of conventional PCNL, and the surgical efficiency of MPCNL seems to be higher than that of RIRS. 8 There are few investigations for the comparison of the surgical efficiency between RIRS and supine MPCNL according to the stone diameters and other stone factors. This is because the surgical cases of supine PCNL are low than those of prone PCNL.
This study investigated the surgical efficiency of RIRS and supine MPCNL according to the stone diameters and other factors. In addition, the authors analyzed the cutoff criterion to determine whether RIRS or supine MPCNL is appropriate for managing renal stones >10 mm.
Materials and Methods
Subjects
Patients ≥20 years of age were included. The guidelines for active surgical removal of renal stones were followed by the European Association of Urology. 5 Individual identifiers were removed and the database was anonymously analyzed. Participants provided their written informed consent to participate in this study. The records of consecutive patients were prospectively included in the database. This study was approved by the Institutional Review Board of our institution.
Patients underwent a single session of RIRS or supine MPCNL when they had a main stone with a maximal diameter >10 mm, growing stones, high risk of stone formation, or SWL-resistant stones. Patients with hydronephrosis were included when there was no definite evidence of complete obstruction. Patients with febrile infection, bleeding disorders, bilateral stones, ureteral stricture, or other anatomical abnormalities were excluded. Patients were given a choice between these two surgical modalities of RIRS and MPCNL after enough explanation about advantages and disadvantages of them according to the European Association of Urology guideline. 5 A total of 310 cases of RIRS and 66 cases of MPCNL were included in a prospective observational study.
Surgical methods
All surgical procedures were electively performed by a single surgeon (S.Y.C.) at our institution, and all procedures were the same as those performed in previous investigations. 3,4 Patients underwent RIRS in the dorsal lithotomy position under general anesthesia. A 11/13F or 12/14F ureteral access sheath (Boston Scientific Corporation, Miami, FL or Cook Medical, Bloomington, IN) was usually placed in the ureter. A Flex-X2™ flexible ureteroscope (Karl Storz, Tuttlingen, Germany) was used. The stones were fragmented with laser fibers of 365 or 200-μm diameter (Trimedyne, Irvine, CA), and the laser power was set at 10 to 15 W. The pulse rates ranged from 5 to 25 Hz for fragmentation and dusting modes, respectively. In the cases of lower caliceal stones, the surgeon tried to reposition them to the upper calix using a stone basket. Trendelenburg position would be helpful to reposition the stones into the upper calix. When the stones were larger than the lower caliceal neck, the surgeon broke them using a laser fiber of 200-μm diameter. Then, the fragmented stones were repositioned into the upper calix and removed by a stone basket. The upper caliceal stones were basically fragmented using a laser fiber with 365 μm diameter.
Patients underwent MPCNL in the modified supine position under general anesthesia. The flank area was upholstered by a long gelform pad to 20° from the table and the spinal needle was inserted into the renal pelvis. A percutaneous nephrostomy tube was inserted into the central region or lower pole calix a day before MPCNL using ultrasound and fluoroscopic guidance by an experienced uroradiologist. Mean procedure time was 10 minutes, and there were no complications during percutaneous procedures. An 18F Ultraxx™ balloon dilator (Cook Medical) and a 15F miniature nephroscope (Richard Wolf, Knittlingen, Germany) were used to acquire the maximal visual field and surgical efficiency using a 550-μm laser fiber. The laser power was set at 70 W. The irrigation fluid enabled spewing out of the fragmented particles from the renal pelvis. The surgeon inserted a Double-J stent through the percutaneous nephrostomy (PCNL) tract during MPCNL and removed the nephrostomy tube at the end of surgery.
Double-J stents were routinely placed and removed 14 days postoperatively. Insertion of a Double-J ureteral stent was not performed in a limited number of patients when the stone volume was low and there was no ureter mucosa tearing or injury after surgery. Preoperative urine microscopy and urine culture were examined in all patients. If specific bacteria were identified from urine culture, the authors used the appropriate antibiotics preoperatively. Otherwise general prophylactic antibiotics were used for both groups.
Clinical parameters
Stone characteristics included stone composition, 24-hour urine collection, and CT scan images, which were performed preoperatively and 3 months postoperatively. The CT scans assessed stone size (mm), stone volume (mm3), average HUs, presence of hydronephrosis, stone location, and the number of stones. Stone volume was the sum of each stone volume (0.523 × length × width × height). The Seoul National University Renal Stone Complexity (S-ReSC) scores were calculated, and this score gave one point to all spaces, such as the renal pelvis, superior–inferior major calices, and anterior/posterior minor calices of the superior/middle/inferior calices. 9,10 Intra- and perioperative parameters included operative times (minutes), laterality, hospital days, etc. The operative times were defined as the time from endoscopic insertion into the urethra to the end of the surgery. Kidney, ureter, and bladder radiograph or low-dose noncontrast CT scans were performed to evaluate the presence of stones at postoperative 1, 14 days, and within 3 months. Clinical stone-free status was defined as absence of stones or any stones <2 mm. Fragmentation efficiency was calculated by the removed stone volume divided by the operative time. Patients were usually followed up at the postoperative clinic 2 weeks, 3 to 6 months, 12 months, and annually thereafter.
Statistical analyses
All parameters were presented as frequency or mean ± standard deviation. Comparative results were analyzed using independent t-test or Mann–Whitney U-test. Analysis of categorical variables was performed by the chi-square test or Fisher's exact test. Linear regression analysis was performed to show the relationship between fragmentation efficiency and the stone size. Multiple logistic regression analyses showed significant predictors to demonstrate the differences in stone-free status with surgery.
Change point analysis is a tool for determining whether a change has taken place, and it shows the occurrence of changes in fragmentation efficiency and the timing of the change. The change point analysis procedure used the cumulative sum (CUSUM) of the ordered value of fragmentation efficiency and stone size to detect the point at which the statistical properties of a sequence of observation change in mean and/or variance. According to the increase in stone size, the CUSUM curves of RIRS would be expected to have a decreasing pattern and the surgical efficiency of MPCNL would be higher that of RIRS in the removal of larger stones at a certain point. Therefore, a density plot would show the cutoff point of the maximal diameter to classify patients into MPCNL and RIRS. Receiver operating characteristic curve analysis was performed to present the cutoff value of the maximal diameter based on the maximal Youden's index (sum of the sensitivity and specificity), and its 95% bias-corrected and accelerated confidence interval (CI) was estimated from 1000 bootstrapping samples. In addition, the curve estimation regression models were analyzed to determine which regression model of a linear, quadratic, or cubic equation would best describe the change in the fragmentation efficiency according to the stone volume. Statistical significance was considered at p < 0.05. Statistical analyses were performed by IBM SPSS Statistics version 20 (IBM, Inc., Chicago, IL) and R version 3.2.1 (
Results
Patient characteristics
No differences in mean age, sex, body mass index, comorbidities, renal function, or stone composition were observed between the two groups (Table 1). Prestenting was performed in a limited number of RIRS cases (12 cases). Stone burden was significantly higher in the MPCNL group than in the RIRS group. Fragmentation efficiency, area of stone distribution (S-ReSC), and the presence of staghorn stones were higher in the MPCNL group than in the RIRS group. Stone-free rates and the complication rates were not different between the two groups. During the supine MPCNL procedure, endoscopic combined intrarenal surgery using flexible cystoscopes and ureterorenoscopes was performed in 6 cases and 20 cases, respectively. The surgeon performed tubeless MPCNL except in a single case. A 16F nephrostomy tube was placed in a single case until postoperative 1 day and removed without any complication.
BMI = body mass index; GFR = glomerular filtration rate; PCNL = percutaneous nephrolithotomy; RIRS = retrograde intrarenal surgery; S-ReSC = Seoul National University Renal Stone Complexity.
The S-ReSC scores were 3.1 ± 2.1 and 4.4 ± 3.4 (p = 0.013), the stone volumes were 5360.8 ± 6345.2 and 7910.6 ± 9734.5 mm3 (p = 0.031), the estimated blood loss was 1.7 ± 13.8 and 76.0 ± 148.0 mL (p < 0.001), the percentages of the presence of a staghorn stone were 18.8% and 37.0% (odds ratio [OR] = 2.5, 95% CI 1.07, 6.05, p = 0.048), and the percentages of the presence of lower pole stones were 68.8% and 87.0% (OR = 3.0, 95% CI 1.11, 8.30, p = 0.040) in the RIRS and MPCNL groups, respectively.
The estimated blood loss was 1.7 ± 13.8 mL for the RIRS group and 76.0 ± 148.0 mL for the MPCNL group (p < 0.001). In RIRS cases, measurement of postoperative hemoglobin was not a routine process; therefore, hemoglobin drop of the RIRS group was not demonstrated. The mean hemoglobin drop in the MPCNL group was 0.90 ± 1.196 g/dL. Transfusion was performed in a single case of the MPCNL group.
Cutoff stone size and volume
As shown in Figure 1A and B, the stone density plot shows that the maximal diameter cutoff level was 16.5 mm (bias-corrected and accelerated 95% CI 13.50, 22.50), which showed the highest Youden's index for which the area under the curve was 0.802 (95% CI 0.740, 0.864). Higher stone size with a cutoff level >16.5 mm was correlated to a harder stone.
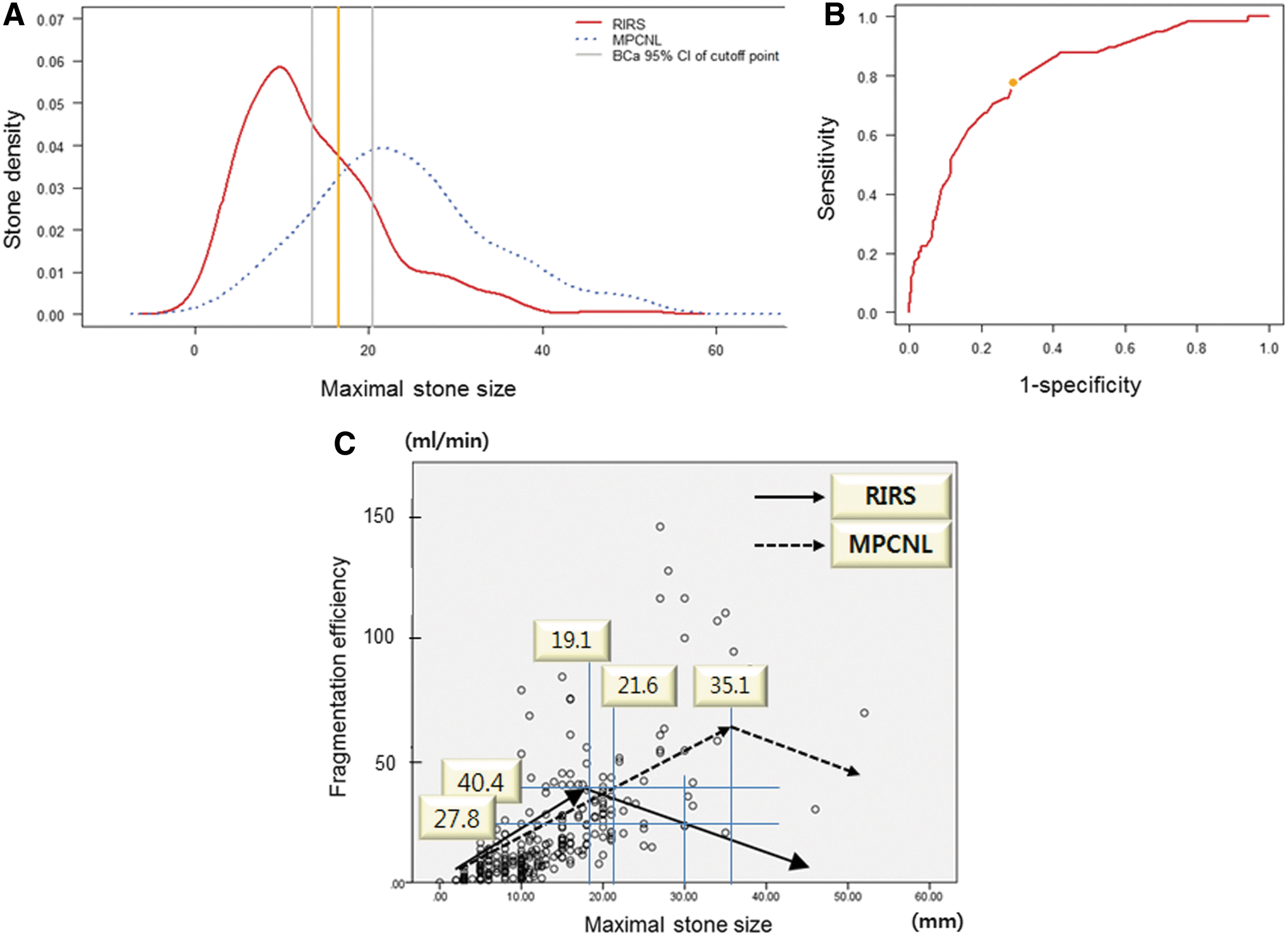
Density plot of the maximal stone size between RIRS and MPCNL.
Figure 1C shows the scatter plot of the fragmentation efficiency in the RIRS and MPCNL groups when the cases without any remnant stones were included. The fragmentation efficiency in the RIRS group was increased to 40.4 mL/min, at which point the maximal diameter was 19.1 mm, and then the fragmentation efficiency started to decrease. Fragmentation efficiency for 10 and 30 mm renal stones was the same at around 27.8 mL/min. Fragmentation efficiency in the MPCNL group was increased to 40.4 mL/min, at which point the maximal diameter was 21.6 mm, which was higher than the maximal diameter of 19.1 mm in the RIRS group. Fragmentation efficiency in the MPCNL group increased continuously with the increase in maximal diameter up to 35.1 mm.
Figure 2 shows the estimation regression models of the change in the fragmentation efficiency according to the stone volume. The R 2 values of the linear and the quadratic equations for RIRS were 0.461 and 0.519, respectively (p < 0.001) and the R 2 values of the linear and the quadratic equations for MPCNL were 0.444 and 0.492, respectively (p < 0.001). The quadratic equations best described the change in the fragmentation efficiency of RIRS and MPCNL according to the stone volume, and the equations are as follows:

The estimation regression models. The R
2 value of the linear and the quadratic equations for RIRS was 0.461 and 0.519, respectively
Y (fragmentation efficiency of RIRS) = −0.0000005 X 2 + 0.0139 X + 4.4784
Y (fragmentation efficiency of MPCNL) = −0.0000001 X 2 + 0.0107 X + 18.4385
Although the maximal stone diameter was the same (30 mm), the fragmentation efficiency showed a downward curve as the stone volume increased from 15,000 to 27,000 mm3 (Fig. 2A). The operative time was 99.5 ± 43.5 and 115.6 ± 53.6 minutes, within the acceptable range, when the maximal stone size was 20.0 and 25.0 mm and 25.1 and 30.0 mm.
Predictors of high fragmentation efficiency and stone-free status
Multiple logistic regression analyses showed that significant predictors of the stone-free status were maximal stone size (OR = 0.956, 95% CI 0.932, 0.982, p = 0.001), the presence of diverticular stone (OR = 0.219, 95% CI 0.078, 0.618, p = 0.004), and the total number of stones (OR = 0.905, 95% CI 0.835, 0.981, p = 0.016).
Multiple logistic regression analyses showed that significant predictors of high fragmentation efficiency >40.4 mL/min were maximal stone size (OR = 1.162, 95% CI 1.111, 1.216, p < 0.001), S-ReSC (OR = 3.591, 95% CI 1.621, 7.954, p = 0.002), and the surgical method of MPCNL (OR = 3.591, 95% CI 1.621, 7.954, p = 0.002) (Table 2).
CI = confidence interval; MPCNL = miniaturized percutaneous nephrolithotomy; OR = odds ratio; RIRS = retrograde intrarenal stone surgery; SWL = extracorporeal shockwave lithotripsy; URS = ureteroscopic stone surgery.
There were no differences in significant predictors of the stone-free status and high fragmentation efficiency >40.4 mL/min according to the presence of lower pole stones.
Discussion
To the best of our knowledge, this is the first study to investigate the cutoff level for determining the appropriate surgical method between RIRS and MPCNL using continuous variables of fragmentation efficiency. The cutoff level of 20 mm has been recommended for PCNL in patients with renal stones. 5 However, none of the previous studies have provided reasonable evidence for determining the cutoff level of renal stone diameter for MPCNL or RIRS.
Previous investigations showed that RIRS can be a good option for renal stones >20 mm. 6 The authors analyzed 310 cases of RIRS after excluding 50 cases during the learning curve in this study. 4 The authors think that the increase in fragmentation efficiency has an upper limit while performing RIRS. Therefore, change point analysis of the fragmentation efficiency may be appropriate to show the point at which any change has taken place. In this study, the maximal stone diameter at the highest fragmentation efficiency was 19.1 mm in the RIRS group. The fragmentation efficiency at the diameter of 10 and 30 mm was similar to each other at around 27.8 mL/min. That may mean that RIRS would be acceptable at the diameter up to 30.0 mm. One more thing about the size criterion of RIRS is that although the maximal stone diameter was the same (30 mm), the fragmentation efficiency of the quadratic equations showed a downward curve as the stone volume increased from 15,000 to 27,000 mm3 (Fig. 2A), which means that stone volume was a better predictor of the fragmentation efficiency required in RIRS than the stone diameter.
A previous study showed that larger stone volume, higher HUs and the absence of preoperative stenting were significant predictors of longer operation during RIRS. 11 However, this study showed different predictors of the fragmentation efficiency. In the univariate and multivariate analyses, the location of stone was not the significant factor for high fragmentation efficacy and the surgical success. These findings might be affected by our surgical methods. As mentioned earlier in the Materials and Methods section, the surgeon tried to reposition them to the upper calix using a stone basket. Finally, the maximal stone size, number of sites involved (S-ReSC), and the operation methods were the independent risk factors for predicting high fragmentation efficiency and surgical success. Therefore, the authors recommend stone size of 30 mm and stone volume of 27,000 mm3 as acceptable upper cutoff values of RIRS.
MPCNL could achieve a higher surgical efficiency than RIRS. This could be because of the shorter skin-to-stone distances, the larger diameters of the access tracts, and easier access to lower pole stones during MPCNL than those during RIRS. The authors performed supine MPCNL using an 18F balloon sheath to maximize surgical efficiency. This size enabled us to use a 550-μm laser fiber with 70 W laser power, which maximized the fragmentation power. In addition, almost all stones between 1 and 5 mm could be removed by the irrigation fluid without use of the forceps or the baskets, which was helpful to shorten the operative time. The authors called it the vacuum-cleaner effect.
Previous studies showed that MPCNL would be appropriate only for mid-sized renal stones. 3 However, MPCNL using an 18F balloon sheath with appropriate devices would be a good substitute for conventional PCNL to remove large stones with a higher safety profile and less discomfort with a tubeless procedure if surgeons can endure a longer operative time than that for conventional PCNL. Unfortunately, there has been little evidence regarding the discrepancy in surgical outcomes between the conventional PCNL vs prone or supine MPCNL, and prone vs supine MPCNL. In this study, the fragmentation efficiency in the MPCNL group increased continuously with the increase in maximal stone size up to 35.1 mm. Therefore, conventional PCNL or a combined endoscopic procedure 12 can be appropriate for renal stones >35.1 mm. During the supine MPCNL procedure, endoscopic combined intrarenal surgery using flexible cystoscopes and ureterorenoscopes was performed in 6 cases and 20 cases, respectively. In Korea, ancillary use of a flexible cystoscope or a flexible ureterorenoscope cannot be charged for the patient as the surgery cost. Therefore, surgeons may be reluctant to use the flexible scopes for removing remnant stones during MPCNL. A flexible cystoscope is less fragile than a flexible ureterorenoscope and the careful handling of the flexible cystoscope can be helpful even in a small-volume center.
Although there has been controversy on the advantages and disadvantages of supine PCNL over prone PCNL, previous studies showed comparable stone-free rates and complication rates between supine and prone PCNL. 13 –15 However, comparison between both of them was not the main topic in this study. The authors wanted to provide the concept of fragmentation efficiency for the reasonable choice of surgical methods and removed the pain scores in the analysis, because our previous study reported that pain scores at postoperative first day were comparable in both groups. 3 Therefore, the pain scores could not be one of the main factors for determining the surgical method between RIRS and supine MPCNL.
This study had some limitations. First, there were fewer MPCNL cases than RIRS cases. However, the authors had experienced several hundreds of conventional PCNL cases and the surgical cases after the learning curve were included. Second, there may be other factors including difference in surgeon's skill, the equipment and accessories, and anatomical factors, such as a narrow infundibulopelvic angle, narrow ureteropelvic junction, or the location of colon. These factors can affect the choice of the appropriate surgical method. Third, operations of this study were performed by a single surgeon. If the operations were performed by many surgeons in multiple centers, the results would be more reliable. However, the risk of bias because of interobserver discrepancy in a multicenter study would be increased as well. 16 Especially, the instruments, equipment, and operation room setting for stone surgery must be quite different among the centers. Therefore, the results of a single surgeon (S.Y.C.) were evaluated to eliminate confounding factors because of differences of surgical methods and devices. Although there are several limitations, this study is valuable as it suggests an appropriate methodology to determine the cutoff criterion of the fragmentation efficiency between RIRS and supine MPCNL using continuous variables of stone diameter and volume.
Conclusions
This study shows that the fragmentation efficiency can be maximized when the surgical option of RIRS and MPCNL is appropriately selected. Stone volume was the better predictor of fragmentation efficiency required in RIRS than stone diameter. RIRS showed the highest efficiency at the maximal diameter of 19.1 mm and the volume of 15,000 mm3. The acceptable level of stone size and volume for RIRS would be 30.0 mm and 27,000 mm3, respectively. However, MPCNL would be appropriate when surgeons want to get high surgical efficiency for renal stone >21.6 mm instead of RIRS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.