
Abstract
Objective:
The aim of this study is to describe (urodynamically) the effect of the use of a 6-branch autologous suburethral sling, made with absorbable sutures and vas deferens, to support the bladder neck and urethra during robot-assisted laparoscopic prostatectomy (RALP) to improve early urinary continence (EUC) recovery.
Materials and Methods:
Retrograde leak point pressure (RLPP) was intraoperatively evaluated, by means of retrograde perfusion sphincterometry (RPS), in 77 patients (mean age ± standard deviation [SD]: 65.64 ± 7.23 years, mean body mass index ± SD: 26.69 ± 3.89) scheduled to undergo RALP at our institution. RLPP was evaluated before (RLPPb) and after pneumoperitoneum induction (RLPPp). RLPP was then evaluated after urethrovesical anastomosis (RLPPa) and after proper sling tensioning (RLPPs), with the aim to obtain the same pressure as after pneumoperitoneum induction. EUC recovery, defined as the use of no pad, was assessed 10 days, 30 days, and 6 months after catheter removal.
Results:
RPS and proper autologous 6-branch sling positioning were feasible in all patients, without perioperative complications and negligible impact on overall operative time. Pneumoperitoneum induction increased, similarly, RLPP in all patients. An important decrease of sphincteric capability was evident after prostate removal and the following urethrovesical anastomosis, while proper sling tensioning allowed for restoration of sphincteric apparatus capability to its presurgical status (mean RLPPs 40.84 cmH2O vs RLPPp 40.39 cmH2O, p = 0.942). EUC recovery within 10 days after catheter removal was achieved in 59 (77%) patients and progressively improved over time.
Conclusions:
RPS, intraoperatively performed during RALP, allows for precise evaluation of the impact of the surgical procedure on sphincteric apparatus competence. Moreover, the use of the 6-branch suburethral sling, in association with RPS, allows for restoration of the proper supporting system to the urethral sphincter, similar to the preoperative condition, offering the basis for EUC recovery after radical prostate surgery.
Introduction
E
The urinary incontinence rate after robot-assisted radical prostatectomy (RALP) varies significantly among the different series, affecting as many as 34% of patients. 2,3
Recent studies 4,5 showed how continence in men, especially after surgery, is not only related to internal and external sphincteric muscles but also (similarly in women) to the proper anatomical position of the pelvic organs and maintenance of adequate urethral supports. Moreover, several urodynamic investigations have been used to properly assess postprostatectomy incontinence to evaluate the sphincteric apparatus, 6 –9 with retrograde leak point pressure (RLPP) being considered the most relevant and user-friendly parameter to be used. 8,9
To improve urethral support to achieve better urinary continence results after RALP, several surgical techniques have been described, 10 –12 and recently, the intraoperative use of autologous slings during surgery has been reported by several authors 13,14 with encouraging results, although doubts remain on proper sling tensioning and its possibility to restore the sphincteric apparatus after prostatectomy.
In this article, we describe (urodynamically), by means of RLPP evaluation during RALP, the impact of radical prostatectomy on sphincteric capacity and the effects of the use of a 6-branch autologous suburethral sling to support the bladder neck and urethra during RALP and its role in restoration of sphincteric efficacy.
Materials and Methods
RLPP was intraoperatively evaluated by means of retrograde perfusion sphincterometry (RPS) in 77 consecutive patients scheduled to undergo RALP at our institution after Ethics Committee approval and including the urodynamic evaluation in the informed consent of the patient. The study is registered in
All the procedures were performed by the same surgeon (A.C.) with more than 10 years experience in RALP procedures.
Table 1 lists preoperative patients' characteristics, with no patient affected by preoperative urinary incontinence or neurological disorders.
BMI = body mass index; PSA = prostate-specific antigen; SD = standard deviation.
RPS technique
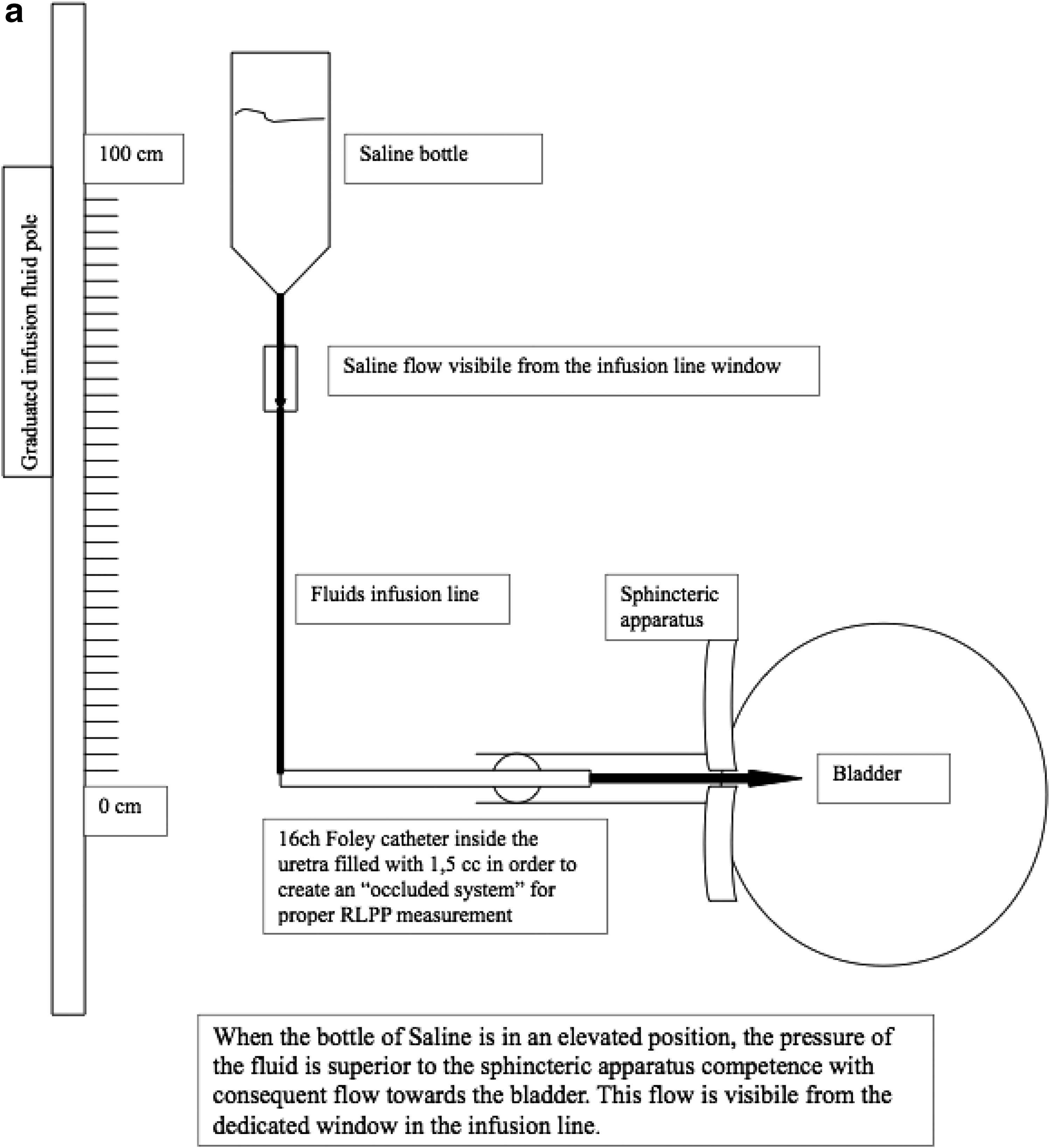
With the patient under general anesthesia, with a nasogastric tube and rectal tube to decompress the bowel properly positioned for the RALP procedure (30° of Trendelenburg), a graduated fluid supporting pole is positioned so that the 0 cm position resulted at the level of patient's pubis (Fig. 1). At the beginning of the surgical procedure, an indwelling 16F Foley catheter is inserted and the bladder fully emptied.

The graduated fluid supporting pole is positioned so that the 0 level corresponds with the pubis, with the patient positioned in 30° of Trendelenburg, ready for surgery.
The deflated Foley catheter is then retracted to mid-urethra/fossa navicularis and inflated with 1.5 mL of saline to prevent fluid extravasation from the external meatus. The catheter is then connected to a 500-mL bottle of saline perfusate and the bottle is progressively lowered (along the fluid supporting pole) from a height of 1 m above the pubis till the fluid stops to flow (Fig. 2). The value, in cmH2O, at which the fluid stops to flow into the bladder, represents the RLPP. Figure 3a and b schematically shows the principles of RLPP evaluation.

The perfusate infusion bag, connected to the Foley catheter positioned at the level of mid-urethra/fossa navicularis, is progressively lowered along the graduated pole till the fluids stop to flow, indicating the degree of retrograde leak point pressure.

6-Branch autologous sling surgical technique
The 6-branch autologous sling technique that we routinely use during RALP has been already extensively described. 15 Briefly, after bilateral vas deferens harvesting at the time of bladder mobilization during RALP, the sling is prepared on the scrub nurse table with six absorbable CT2 needle 0-Vicryl sutures (each measuring 16 cm in length) tied centrally together; the vas deferens is cut into six specimens and transfixed with the suture and collected centrally to create the bulky central part of the sling (Fig. 4).
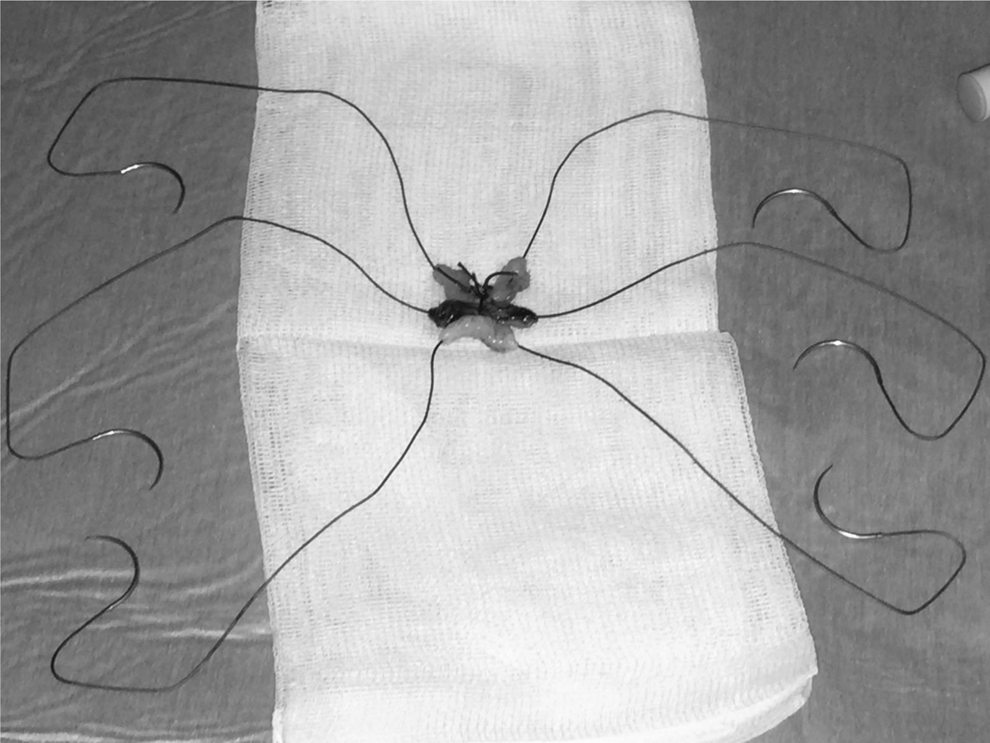
The 6-branch autologous sling.
Before restoration of urinary continuity, the sling is introduced into the surgical field and its extremities are fixed bilaterally to the periosteum of the pubic branches at the medial (just lateral to the symphysis), lateral, and posterior levels; Denonvilliers' fascia is restored in a double layer manner to separate the urethrovesical anastomosis from the sling. Upon completion of urethrovesical anastomosis, the sling is tensioned, tightening together the two medial branches first; after subjective proper tension is achieved, the RLPP is evaluated and the tension adjusted accordingly to achieve an RLPP similar to presurgery values. The two medial branches are then knotted together and subsequently the two lateral ones on each side, as shown in Figure 5.
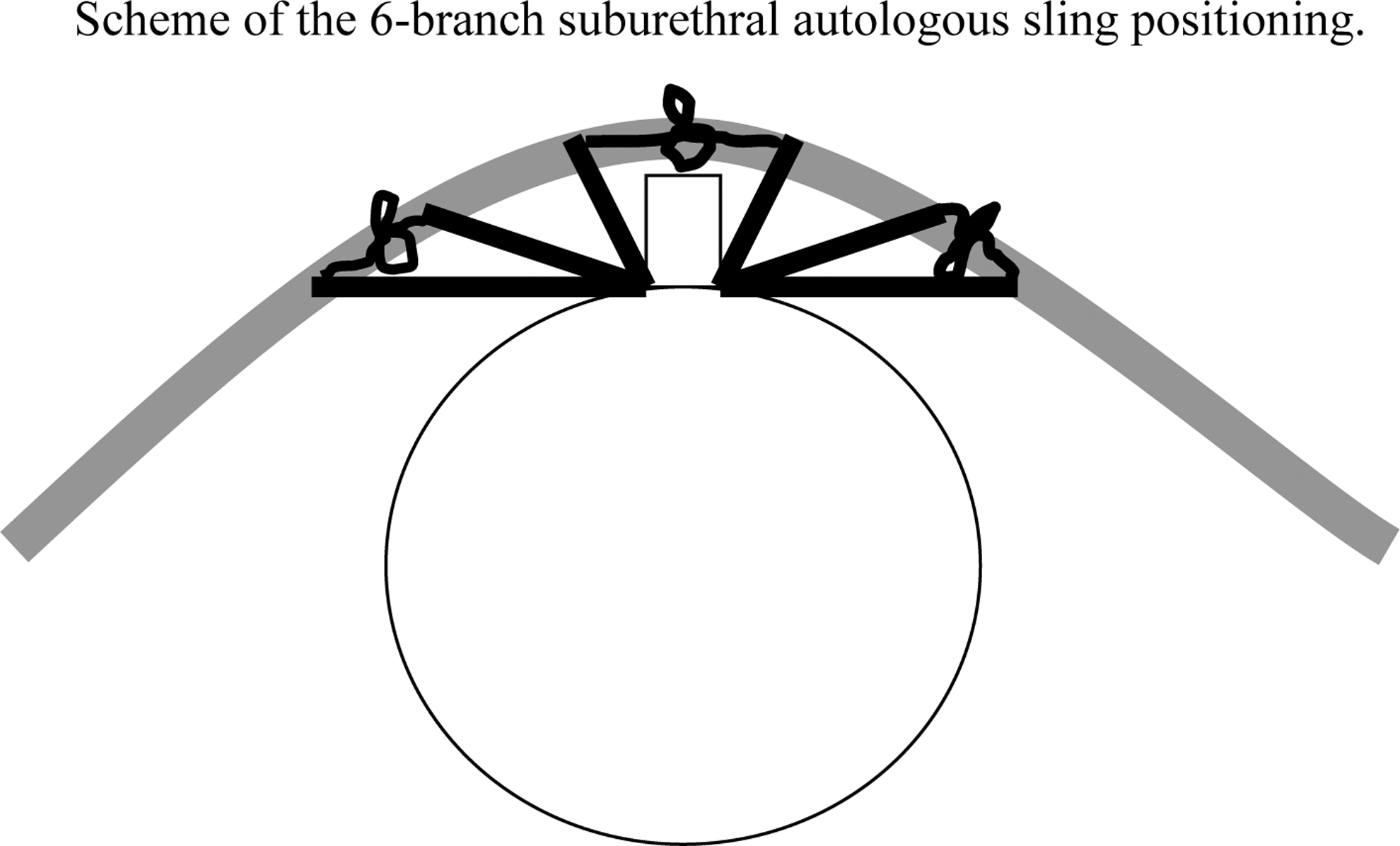
Scheme of the 6-branch suburethral autologous sling positioning.
RLPP was, respectively, evaluated before pneumoperitoneum induction (RLPPb) and after pneumoperitoneum induction (RLPPp). RLPP was then evaluated after urethrovesical anastomosis (RLPPa) and during proper sling tensioning (RLPPs). The aim of sling tensioning was to obtain similar pressures as after pneumoperitoneum induction (RLPPs ≅ RLPPp).
Each measurement was repeated three times at every step and the mean value considered.
Primary endpoints of the study were (1) to demonstrate that pneumoperitoneum does not impair the RLPP evaluation, (2) to evaluate the impact of prostatectomy on sphincteric efficiency, and (3) the possibility to improve RLPP with proper sling tensioning, with the goal to restore sphincteric efficiency similar to the presurgical condition.
Secondary endpoints included time to perform the intraoperative urodynamic evaluation, eventual difficulties, and/or complications related to the clinical procedure.
Moreover, early urinary continence (EUC) recovery, defined as the use of no pad, was also evaluated 10, 30, and 180 days after catheter removal and stratified by classes of age (<60 years, 60–70 years, and >70 years).
Statistical methods
Continuous variables are expressed as means ± standard deviations and categorical data as frequencies and proportions. An analysis of variance model for repeated measures was fitted, including unstructured covariance to take into account the correlation among measurements on the same subjects, to estimate the RLPP mean for each phase and their 95% confidence interval (CI). Pairwise comparisons among phase means were conducted by means of Tukey's 16 method to take into account the type I error (alpha). All analyses were performed using SAS, version 9.4, software (SAS Institute, Cary, NC). Statistical significance was set at the 0.05 level. All p-values were two-sided.
Results
RPS and proper sling positioning and tensioning were feasible in all patients without any perioperative complications; the mean surgical time was 218 ± 39.78 minutes and the time required to perform urodynamic evaluations and sling positioning was similar in all patients, resulting in <15 minutes for all cases, with negligible impact on overall surgical time during RALP.
Table 2 lists in detail the results of RLPP measured at various steps of the procedure, as previously described. In detail, RLPP increased similarly in all patients by ∼8 cmH2O (95% CI: 6.81–9.31) after pneumoperitoneum induction and consequently allowed for proper evaluation of its modification during RALP.
RALP = robot-assisted laparoscopic prostatectomy; RLPP = retrograde leak point pressure.
RLPPa was significantly reduced compared with RLPPp, showing a significant reduction in sphincteric efficacy after prostatectomy (RLPPp vs RLPPa: −11.00 cmH20—95% CI: −12.52, −9.48 cmH20), while proper sling tensioning allowed for a significant improvement of RLPP values compared with postanastomosis completion evaluation (RLPPs vs RLPPa: +11.46 cmH2O—95% CI: 10.13, 12.78 cmH20) with consequent improvement of sphincteric efficacy with the possibility to restore it to preoperative values.
Compared with subjective sling tensioning, in 3 patients (4%), it was necessary to reduce the tension of the sling, and in 23 patients (30%), it was necessary to increase the tension, while in 51 cases (66%), subjective tensioning was adequate to restore RLPP values similar to the preoperative condition.
EUC recovery is reported in detail in Tables 3 and 4.
Chi-square test.
Fisher test.
(A) Subgroups of patients where subjective tensioning was adequate to restore proper RLPP and (B) where tensioning had to be modified according to RPS results to restore RLPP.
Chi-square test.
Fisher test.
One patient experienced acute urinary retention after catheter removal and was treated uneventfully with catheterization for an additional 7 days, without consequences and with a pad-free condition after removal of the catheter.
Continence 30 days postcatheter removal was achieved in 57 (74%) patients and improved over time with 90% (26 patients) 0-pad status in the 29 patients who reached 6-month follow-up continence evaluation.
Interestingly, there were no differences in continence recovery among patients stratified for different age classes, although in elderly patients (>70 years), there was a tendency toward worse EUC recovery compared with younger patients. Moreover, proper sling tensioning under RPS guidance allowed for similar urinary continence recovery in the subgroups of patients where sling tensioning did not require or required modifications over the subjective evaluation, as shown in Table 4.
Discussion
Intraoperative RPS revealed to be a reliable instrument to assess sphincteric efficiency and its modification during RALP as well as to evaluate the role of the autologous suburethral sling in restoring effectiveness of the sphincteric apparatus to preoperative values and offer the basis for EUC recovery after prostate surgery.
The role of proper urodynamic evaluation of postprostatectomy urinary incontinence has been underlined by several authors, particularly in defining the degree of postsurgical intrinsic sphincteric deficiency. 6 –9 Bamshad and colleagues 8 demonstrated a significantly lower retrograde urethral perfusion pressure in patients with postprostatectomy urinary incontinence compared with continent patients, while Comiter and colleagues documented how RLPP correlates with all the urodynamic parameters routinely used to assess sphincteric competence, such as maximal urethral closure pressure and abdominal leak point pressure, 6 and how RLPP correlates with sphincteric deficiency after radical prostatectomy, with significant difference between incontinent and continent patients. 9
Compared with more complex urodynamic tests, RLPP evaluation appears to be an easy-to-perform urodynamic diagnostic tool, not requiring sophisticated instruments, adequate for evaluation of the sphincteric apparatus before and after prostate surgery. 8,9
The RSP technique we described, derived from the technique routinely used for proper intraoperative evaluation during AMS 800 artificial urinary sphincter implants, 17 confirmed to be a reliable instrument in proper RLPP and sphincteric apparatus competence evaluation. It appeared to be a user-friendly system, easy to use and cost-effective, not requiring particular instrumentation, and requiring negligible amount of time to properly assess sphincteric capacity during the various phases of surgery.
We documented how pneumoperitoneum per se does not impair proper evaluation of the sphincteric apparatus of patients since RLPP increased by a similar value in all patients, with the variation observed characterized by low variability as indicated by the CI, thus allowing for proper further evaluation of sphincteric apparatus during the following steps of surgery.
Moreover, we demonstrated a significant reduction in sphincteric apparatus efficiency following prostate ablation compared with preoperative status even if, for technical reasons (to protect the fresh anastomosis from potential damages and erosions related to the sling under tension), the RLPPa evaluation was performed after reconstruction of the posterior musculofascial planes (Rocco's stitches). These findings may partially explain the conflicting results reported in literature regarding the efficacy of Rocco's stitches for EUC recovery. 10
To our knowledge, we were the first to report with the use of intraoperatively urodynamic evaluation, the degree of negative impact of prostate extirpation on the sphincteric apparatus, evaluating RLPP differences during the procedure, thus confirming the importance of the anatomical supporting system in determining continence in men, as shown in radiological postoperative studies between continent and incontinent men after radical prostate surgery. 4,5
General anesthesia did not have a negative influence on RLPP evaluation in our series. This finding had been already confirmed in both experimental 18 and clinical settings, 19 where urodynamic evaluations under general anesthesia confirmed for proper evaluation of sphincteric apparatus while eventually blocking bladder overactivity. 19 Those findings further confirm the efficacy and reliability of RLPP evaluation during surgery, not eventually affected by detrusor overactivity, for proper assessment of sphincteric efficiency.
Suburethral autologous sling positioning during RALP has been recently proposed to better support the sphincteric apparatus, thus offering increased EUC recovery rates compared with nonsling groups. 13,14 Moreover, we demonstrated in a prospective randomized manner how the 6-branch sling was superior to a simple sling in achieving EUC recovery after RALP. 15 Nevertheless, one of the main criticisms regarding autologous sling positioning is related to subjective tensioning of the sling by the surgeon, 14 –20 with the risk of obstruction and urinary retention in cases of excessive tensioning or reduced efficacy in cases of inadequate tensioning. Insufficient tensioning of the sling may partially justify the failure in obtaining significant advantages in EUC recovery in the sling group as reported by Bahler and colleagues 21 and Nguyen and colleagues. 22 The intraoperative use of RPS resulted as being fundamental for proper sling tensioning, allowing for proper restoration of the sphincteric apparatus efficiency, with the possibility to adjust the tensioning of the sling, following proper intraoperative urodynamic evaluations. Compared with the subjective tensioning evaluation, as previously used, based on surgeon's experience, in 30% of patients, we had to increase the tension, while in 4% of patients, we had to reduce the tension on the sling, demonstrating how simple subjective evaluation may be inadequate for proper autologous sling tensioning. Moreover, the possibility to adjust sling tensioning, allowed for similar results in terms of EUC in the two subgroups of patients where, respectively, subjective tensioning was adequate to restore RLPP or where the tension of the sling required modifications.
With the aid of RPS to properly assess autologous suburethral sling tensioning, 77% and 74% of the patients experienced recovery of urinary continence within, respectively, 10 and 30 days after catheter removal, which progressively improved to 90% within 6 months after surgery, without differences in various classes of age, supporting the role of suburethral slings in restoring the sphincteric effectiveness after RALP procedures.
Nevertheless, this study has several limitations, such as the absence of a control group (evaluating the association of EUC recovery and RLPP in the absence of autologous suburethral sling). Since we extensively proved the efficacy in our experience of the use of autologous suburethral slings during RALP to improve EUC in similar cohorts of patients, 14,15 we decided not to include a control group for the main purposes of the study that were the evaluation of the impact of prostatectomy on sphincteric efficiency and the possibility to improve RLPP with proper sling tensioning, with the goal to restore sphincteric efficiency similar to the presurgical condition.
We used the 0-pad status to report urinary continence recovery in this study, although in cases of comparative or multicenter studies, more sophisticated instruments to properly assess EUC recovery such as pad count/weight and questionnaires would be better advocated. However, the present findings are preliminary and limited because of single surgeon experience. It is critical to see if the results are applicable to surgeons in general through a multisurgeon and multicenter randomized trial.
Nevertheless, based on our findings, RPS—for proper 6-branch autologous sling tensioning—becomes a standard step during RALP procedures performed at our institution.
Conclusions
RPS, intraoperatively performed during RALP, allows for precise evaluation of the impact of the surgical procedure on sphincteric apparatus competence. Moreover, the use of the 6-branch suburethral sling, in association with perfusion sphincterometry, allows for restoration of the proper supporting system to the urethral sphincter, similar to the preoperative condition, offering the basis for EUC recovery after radical prostate surgery.
This urodynamic evaluation revealed to be safe, feasible, easy to perform, and reproducible, with negligible impact on overall surgical time during RALP.
Further studies, preferably in a multi-institutional setting, are desirable to assess the role of RPS in autologous sling tensioning during RALP procedures to properly restore the sphincteric apparatus and achieve EUC recovery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.