
Abstract
Introduction:
Patients with ileal conduit urinary diversions are at an increased risk of long-term upper urinary tract (UUT) complications, including anastomotic strictures, infections, and urolithiasis. The reconstructed urinary system poses challenges for endoscopic manipulation. We present and describe our dual-center experience in performing retrograde ureteroscopy to treat or diagnose UUT abnormalities in patients with ileal conduit incontinent diversion.
Patient and Methods:
We performed a retrospective analysis of medical records for all patients with previous urinary diversion who underwent retrograde ureteroscopic procedures via the ileal loop in our institutions over a 9 year period (between June 2007 and August 2016).
Results:
Fifty-four procedures were performed in 36 patients. Mean age was 61 (28–90) years. Average time from diversion to ureteroscopic procedure was 13.0 (0.08–53) years. Stone disease was the most common indication for intervention in 35.2% (19/54) of cases, with a stone-free rate of 78.9% (15/19). Other indications included surveillance of transitional-cell carcinoma in 22.2% (12/54), diagnostic flexible ureteroscopy (fURS) in 20.4% (11/54), stricture management in 11.1% (6/54), removal of encrusted stent/nephrostomy in 7.4% (4/54), urine leak after diversion in 1.9% (1/54), and miscellaneous in 1.9% (1/54). Successful retrograde access was possible in 74% (40/54) of cases. A long and tortuous ileal segment, too difficult to negotiate, was the most common cause of failure to access the UUT. In 13 out of 54 (24.1%) cases, retrograde fURS was combined with simultaneous percutaneous antegrade access. Six patients (11.1%) developed postprocedural pyrexia requiring additional antibiotic therapy, and one (1.9%) patient required embolization of the renal artery for ongoing bleeding. Median length of stay was 1 day (0–55), with 13 (24%) being performed as day-case procedures.
Conclusions:
Retrograde ureteroscopy in patients with ileal conduits can be technically challenging due to distorted anatomy. This procedure can be safely performed in experienced hands with standard endourological equipment. An antegrade approach can be carried out simultaneously, which may be required in a small number of patients.
Introduction
P
In addition, those with a history of urolithiasis have a significantly higher risk of recurrent stones, with an estimated 5 year recurrence rate as high as 63%. 4 Those undergoing cystectomy for bladder cancer are also at an increased risk of developing subsequent recurrences in the UUT, thus necessitating access to the upper tract through the ileal conduit, if recurrent or new malignancy is suspected.
Advances in endoscopic equipment and technique have shifted the surgical treatment of UUT pathology away from the conventional open procedures into the realms of minimal invasive endoscopic surgery. This has resulted in a reduction in the risk of complications, procedural morbidity, and length of hospital stay/recovery. 2 However, despite the reduced morbidity that is associated with endourological techniques, the reconstructed urinary tract poses a variety of challenges that are largely due to the altered nature of the anatomy. Upper tract maneuverability in the conduit is difficult due to its tortuosity, and subsequent cannulation of the ipsilateral ureter may not always be possible. Several authors have described retrograde, antegrade, and combined endoscopic approaches to complications that are associated with a variety of urinary diversions. 5 –15 These reports are often limited by small numbers of patients, with the majority of authors preferring a percutaneous or antegrade ureteroscopic approach. 16 We describe our dual-center experience in performing retrograde ureteroscopy to treat or diagnose UUT abnormalities in patients with ileal conduit diversion.
Patients and Methods
We performed a retrospective analysis of medical records for all patients with previous urinary diversion who underwent retrograde ureteroscopic procedure in our institutions over a 9 year period (from June 2007 to August 2016). All the procedures were performed by experienced endourologists in the two hospitals. Both hospitals are tertiary referral centers for stone disease management and cover the most of Lancashire County in the United Kingdom. The hospital records were reviewed to identify patient demographics, primary diagnosis resulting in urinary diversion surgery, the indication for retrograde ureteroscopy, procedural technical details, rate of successful access to the ureter and kidney, and associated intra- and postoperative complications. Additional information collected included length of stay, cause of failure to access the ureter, and successful treatment of stones.
Technique
All patients provided a urostomy urine sample for urine culture between 1 and 2 weeks before the procedure. This was collected from the patients' urostomy bag into a sterile pot. Those with a positive urine culture received 1 week of the appropriate oral antibiotic preoperatively. All patients, irrespective of the preoperative urine culture, received intravenous antibiotics at induction of anesthesia (predominantly an aminoglycoside, such as gentamicin, unless otherwise indicated by preprocedural urine culture). Patients did not routinely receive postoperative antibiotics. All procedures were initially commenced in the supine position under a general anesthesia. The patient was subsequently placed in a prone position if a percutaneous approach was required. The ileal conduit (ileal loop) was initially accessed by using a 17F flexible cystoscope to clarify the integrity and anatomy of the conduit up to the uretero-ileal anastomosis (looposcopy). In case of difficulty in maneuvering the ileal loop, a loopogram was performed by injecting contrast through the flexible cystoscope to demonstrate the anatomy of the conduit. Once visualized, the appropriate ureteral orifice was cannulated by using either a 0.035” standard guidewire (Boston Scientific, Natick, MA) or a hydrophilic glidewire (Terumo, Somerset, NJ). A 6F open-ended ureteric catheter was introduced over the guidewire to facilitate a retrograde pyelo-ureterogram contrast study for the demonstration of pelvi-caliceal anatomy.
Access to the ureter and kidney was obtained by introducing a flexible ureteroscope (9.5F, Flex-X2; Karl Storz, Tutlingen, Germany) over the guidewire for subsequent diagnostic or therapeutic pursuits. In cases of a tortuous and difficult-to-maneuver ileal conduit, success manipulation was facilitated by the placement of a 12F multiple-access sheath (Boston Scientific) over a stiff guidewire that had the effect of “straightening” the ileal conduit with advancement of the flexible ureteroscope via the access sheath. Failure was defined as the inability to access the ipsilateral ureter in a retrograde fashion via the ileal loop. In cases of urolithiasis, stones were fragmented via flexible ureteroscopy (fURS) by using holmium YAG (Ho-YAG) laser lithotripsy with a 365 μm fiber, unless percutaneous nephrolithotomy (PCNL) was indicated in patients with a large stone burden. Similarly, stricture incision and ablation of small-volume, nonmuscle invasive UUT transitional-cell carcinoma (TCC) were undertaken by using Ho-YAG laser.
Where percutaneous access for antegrade manipulation was necessary, renal collecting system puncture was obtained by the urologist using fluoroscopic guidance. Tract dilatation was performed to either 26F or 30F by using either a balloon device (30F) or serial metal dilators (26F).
Post-fURS drainage, where deemed necessary, was in the form of either an open-ended ureteral catheter placed in situ overnight or a 6F/8F double-pigtail ureteral stent left in for 2 weeks. In patients who underwent a simultaneous percutaneous procedure, a 10F single-pigtail nephrostomy tube was positioned at the completion of surgery.
Results
In total, 54 retrograde ureteroscopic procedures were attempted in 36 patients over a 9-year period. Patients who underwent bilateral fURS at the same sitting were only counted as having undergone a single procedure. Where the same patient had undergone multiple ureteroscopic procedures during the study period, no more than two of the episodes were included in the analysis.
The mean patient age was 61 (28–90) years. The mean time from diversion to ureteroscopic intervention was 13 (0.8–50) years. The indications for the original diversion surgery were cystectomy for bladder cancer, 52.7% (n = 19); spina bifida, 19.4% (n = 7); neuropathic bladder due to multiple sclerosis, 8.3% (n = 3) and secondary to spinal cord injury, 2.7% (n = 1); interstitial cystitis, 5.5% (n = 2); total pelvic clearance due to locally advanced rectal adenocarcinoma, 2.7% (n = 1); and total pelvic clearance due to locally advanced cervical cancer, 5.5% (n = 2).
The type of uretero-ileal anastomosis performed at the time of initial ileal loop urinary diversion was recorded in 35 out of 54 cases. Of the recorded cases, 29 had a Wallace type II, two had undergone a Bricker uretero-ileal reconstruction, and in four a single ureter was anastomosed to the conduit. The Wallace type II anastomosis is more commonly performed in the United Kingdom.
With regards to indications for ureteroscopic intervention, UUT stone disease was the most common in the majority (35%) of cases (Table 1).
fURS = flexible ureteroscopy; TCC = transitional-cell carcinoma; UUT = upper urinary tract.
Retrograde ureteroscopic access to the UUT was possible in 74% (40/54) of cases. Successful retrograde access was defined as satisfactory access to the part of the UUT (ureter or pelvicaliceal system) that was relevant, which required either assessment or treatment. In the remainder (14/54), a long and tortuous ileal segment, which was too difficult to negotiate, was the primary cause for failure to access the ureter. The other causes of failure to access the ureter are listed in Table 2. The techniques used to access the UUT are discussed in detail later in this article. The time interval from the original urinary diversion construction to retrograde fURS did not influence the chance of successful ureteral access. Successful looposcopy was performed in all patients who had had a Bricker anastomosis and in 50% (2/4) of the cases in whom a single ureter was anastomosed to the conduit.
A 12F multiple-access sheath was used in four cases to negotiate the tortuous conduit. The indication for multiple-access sheath usage was left to the discretion of the operating endourologist. In none of these four patients was a simultaneous percutaneous procedure necessary. In five cases, there was satisfactory access to the UUT via looposcopy but these patients also required a PCNL puncture due to their stone burden and in two of these, the tortuous ileal loop made intra-renal maneuverability too difficult to deal with the stones via ureteroscopy.
In 13 out of 54 (24.1%) patients, the retrograde ureteroscopic manipulation was followed by prone percutaneous access to the collecting system. Indications were significant (multiple stones or stones >1 cm in maximum dimension) stone burden (n = 8), antegrade balloon dilatation of a ureteric stricture (n = 1), calcified and knotted stent or nephrostomy (n = 3), and TCC surveillance (n = 1).
The time to find the ureter or total operative time was not recorded uniformly and, thus, not reported in this study. The median length of stay was 1 day (range 0–55 days). Length-of-stay data for 52 patients are included here. Two patients were excluded as one had no length-of-stay data recorded and the other patient had two procedures performed during the admission. Twenty-four percent (n = 13) were performed as day-case procedures, 33.3% (n = 18) had an overnight stay, and 38.8% (n = 21) had multiple-day stays. In the patient with a 55 day length of stay, the discharge was delayed due to inadequate home social circumstances and was not related to the urological intervention.
Seven patients had a postsurgical complication. Six patients had a postoperative systemic inflammatory response syndrome (SIRS) requiring additional intravenous antibiotic therapy without necessitating high dependency/intensive care support, supplementary surgical intervention, or renal drainage. One patient required selective renal arterial embolization due to prolonged bleeding after simultaneous PCNL. Of the six patients who required postoperative antibiotic treatment, only one patient had a positive postoperative urine culture (Escherichia coli), two patients had no postoperative urine culture results available, and three patients had negative cultures. Four out of the six patients with a postoperative SIRS had positive preoperative urine culture, but all had received appropriate oral antibiotics before surgery and intravenous gentamicin on induction of anesthesia. Of the six patients who had SIRS, five patients had some form of drainage, which included three patients having a nephrostomy.
Stone disease
Nineteen patients underwent flexible retrograde ureteroscopy and laser stone fragmentation with or without PCNL. Table 3 shows the stone size, stone position, whether a simultaneous PCNL was required, and method of assessment of stone clearance for each of the procedures.
PCNL = percutaneous nephrolithotomy.
Stone burden was difficult to assess accurately due to the finding of multiple renal/ureteral calculi in the majority of these patients. Ureteroscopic stone treatment was performed with Ho-YAG laser fragmentation into <2 mm fragments, which were allowed to pass spontaneously. A simultaneous PCNL was required in nine patients either due to inadequate retrograde access or because of significant stone burden (multiple stone or the presence of stone >1 cm). Treatment success was defined as the absence of stones >2 mm either endoscopically or on postprocedure plain abdominal radiography, noncontrast CT scan, or nephrostogram was 78.9% (15/19). Of these, two cases did not have postoperative imaging as detailed earlier and stone-free status was based on the surgeon's opinion at the conclusion of the procedure.
Ureteral/uretero-ileal stricture disease
Of the six patients with stricture disease, retrograde ureteroscopic access was unsuccessful in one, with the patient requiring antegrade ureteroscopy and balloon dilatation after renal puncture. In three cases, a balloon dilatation (n = 2) or one-step bougie dilatation (Nottingham one-step dilator; Boston Scientific) over a guidewire (n = 1) was performed to adequately dilate the stricture. In the remaining case, no dilatation was required and the ureter was easily negotiated with the flexible ureteroscope, thus excluding any significant stenosis. We defined a stricture as either an excessive narrowing of a segment of the ureter (with/without reflux of contrast) in retrograde contrast studies or evidence of obstruction on radioisotope renography.
Postoperative drainage
Postoperative drainage was dependant on the nature of intervention and the presence/absence of ureteric trauma. In total, 23 U (42.7%) were deemed to not require any renal drainage postprocedure. When required (n = 31), renal drainage was achieved by using a double-pigtail ureteral stent (n = 17) with the lower end resting in the ileal loop, a 6F open-ended ureteric catheter removed on day 1 postoperatively (n = 4), or a 10F self-locking nephrostomy tube in those undergoing a simultaneous PCNL (n = 10). For stone patients and those with a UUT malignancy, the ureteral stents were removed after 2 weeks, but for cases of ureteral stricture disease, stents were left in situ for 4 to 6 weeks.
Failure to gain retrograde access to the ureter
The clinical and outcome data related to patients in whom retrograde ureteroscopic access failed are summarized in the table (Table 4). In some cases, a lengthy and tortuous ileal conduit made retrograde access impossible (Figs. 1 and 2).
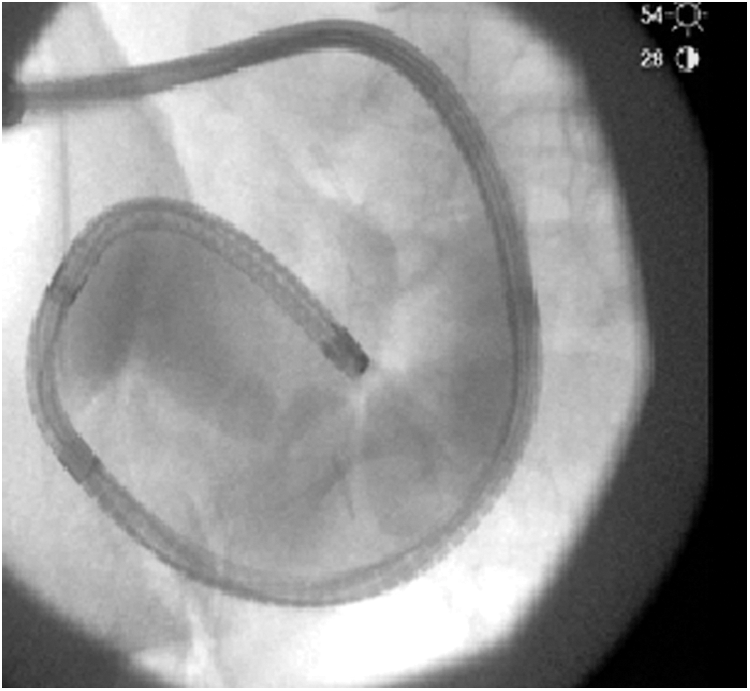
An example of multiple deflections ileal loop.
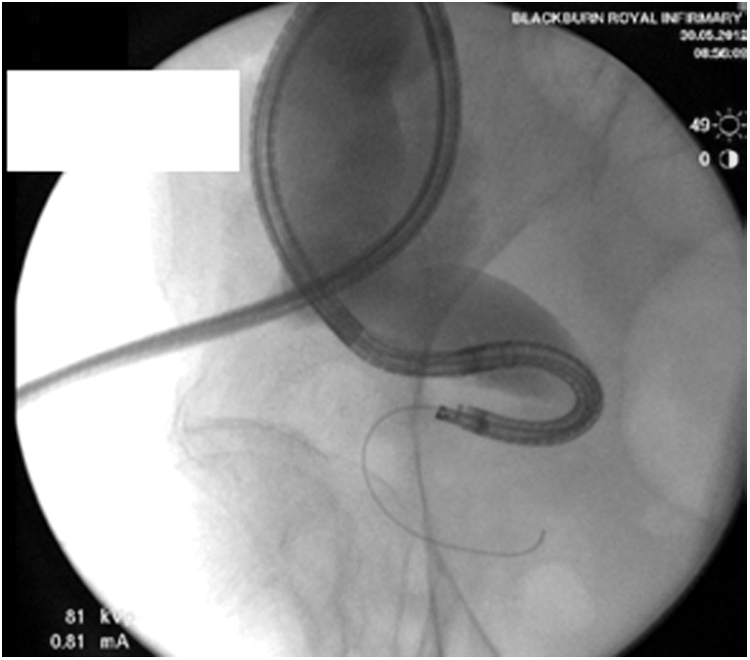
An example of long and tortuous ileal loop.
Discussion
Irrespective of the type of urinary diversion, such patients are at a higher risk of upper tract complications, including nephrolithiasis and anastomotic strictures of between 1.7% and 29%. 16 Factors promoting stone formation include bacterial colonization, urinary stasis, reflux of mucus into the upper tract, and diversion-associated urinary metabolic abnormalities such as acidosis, hypercalciuria, hyperoxaluria, and hypocitraturia. 2,17 Though most patients ultimately remain asymptomatic, the reported incidence of stone disease in patients with an ileal conduit ranges from 9% to 11%, whereas this rises to between 11% and 27% for other types of continent diversions (e.g., Kock and Indiana pouch diversion), with an overall recurrence rate of between 33% and 63% within 3 to 5 years after the initial intervention. 1,8,18
It is likely, therefore, that patients with ileal conduit diversions will require manipulation of the UUT, which poses a challenge due to anatomic distortion. Some endourologists prefer to adopt an antegrade or combined antegrade-retrograde approach but this exposes patients to risks that are associated with percutaneous renal puncture, including bleeding, sepsis, and pleural and adjacent organ injury. 19
Several authors have described their experience with an antegrade approach to accessing the upper tracts in urinary diversions. 14,20,21 In 2014, Zhong et al. performed percutaneous antegrade access in 20 patients with urolithiasis. 20 All patients had an attempt at retrograde ureteroscopic access initially; however, they all failed due to difficulty in accessing the ureteric orifice or traversing the ureteroenteric anastomosis. Eighteen patients were rendered stone free with a clearance of 90%, and 15% of patients had complications using the antegrade technique. In 2013, Stuurman et al. described their experience of using a ureteral access sheath in an antegrade approach. 14 Overall, 21 antegrade flexible ureteroscopies were performed on 17 patients. In 66.6% of patients, a nephrostomy was already in situ before the operation. Successful puncture was performed in all other patients, with four procedures encountering complications. Overall, 82.3% of patients were rendered stone free after the first antegrade procedure and all strictures were successfully managed with balloon dilatation. The stone-free rate in our study was 79% by using a retrograde technique that was associated with fewer serious complications.
The combined antegrade/retrograde approach has been described to good effect. In 2000, Delvecchio et al. described a technique where percutaneous access was established and then under fluoroscopic guidance, a guidewire was manipulated through the percutaneous needle and down through the ureteric orifice to the pouch. 21 Then, a ureteroscopy was performed in a retrograde fashion over the guidewire or through an access sheath. In their study, five patients (mean follow-up of 12 months) were treated, allowing successful access to the pathological areas in all patients with no reported peri-operative complications. The authors argue that this method allows better delineation of the anatomy, facilitating more efficient fragmentation of calculi. It allows better irrigation, enabling enhanced visibility of stenotic segments that may be hidden by mucosal folds.
In 2014, Rivera and Krambeck reported their experience with retrograde ureteroscopy with continent urinary diversions (12 patients on 17 renal units). They stated that the afferent limb of the neobladder was challenging due to angulation, tortuosity, and extreme length. The authors' success rate was 59%; they state that this is lower than previously published reports but could be related to the length of time between neobladder formation and attempted ureteroscopy. 15 We did not find that the length of time between the initial surgery and ureteroscopy had any impact on our results but we can draw comparisons with these results due to similar anatomical distortions. In 2009, Hyams et al. reported their experience with retrograde ureteral access and/or renal access in patients with urinary diversion (15 patients on 21 renal units). 7 Their success rate was quoted as 75%, which was broken down into 90% in orthotopic neobladders, 73% in ileal conduits, and 33% for Indiana Pouches. The main reason for failed retrograde ureteroscopies was in patients with anastomotic strictures, and they all went on to have successful antegrade access. They quote a 50% success rate in patients with anastomotic strictures; however, in our study, the success rate in these patients was 80% (4/5). For the management of renal tract stones, they quoted a stone-free rate of 60%. The main reasons for difficulty in gaining access were a long tortuous ileal conduit or anastomotic strictures.
The preference in our institutions is to initially attempt retrograde ureteroscopy to gain access in the upper tracts due to the lower morbidity associated with this procedure. We acknowledge the limitations in our article. The retrospective nature of the study over a relatively longer period potentially introduces bias, but in our opinion, simply reflects the infrequent nature of this specific procedure. In addition, though the patient numbers may be small, to the best of our knowledge, this reflects the largest series of patients undergoing retrograde flexible ureteroscopic manipulation via an ileal conduit urinary diversion. In addition, our two-center data represent the overwhelming majority of all such cases in Lancashire County, England. Our stone-free rate, using the retrograde approach of 79%, is similar to other comparable reports (e.g., Hyams—75%). 7 Unfortunately, operative room time was not consistently recorded in all patients and, thus, has not been reported. In our series, the retrograde approach was associated with a shorter hospital stay with a median length of stay of only 1 day and a relatively low rate (2%) of Clavien-Dindo Grade ≥3 complications necessitating surgical, endoscopic, or radiological intervention in the postoperative period.
In our experience, we found the following techniques to improve our chances of successful retrograde ureteroscopy via the ileal loop: Initial inspection of the ileal loop by using a 17F flexible cystoscope followed by a contrast loopogram helps delineate the anatomy; gentle occlusion of the stomal orifice with a finger allows for distention of the conduit, enabling improved endoscopic visualization; the use of a 12F multiple-access sheath over a 0.035” standard guidewire will help negotiate the tortuous conduit and “straighten” the ureter; and advancement of the flexible ureteroscope is often easier over a stiffer guidewire (0.035” Amplatz Super Stiff guidewire; Boston Scientific) rather than a standard guidewire when excessive tortuosity is encountered.
Conclusions
Retrograde ureteroscopy in patients with ileal conduits can be technically challenging due to distorted anatomy and potential ureteral/uretero-ileal anastomotic strictures. Our data reflect “real-life” practice and demonstrate that this procedure can be safely performed in experienced hands with standard endourological equipment and is associated with a satisfactory success rate with low morbidity. An antegrade approach can be carried out simultaneously, which may be required in a small number of patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.