
Abstract
Background and Purpose:
Bipolar transurethral resection of bladder tumors (TURBTs) has been claimed to have lesser complications and better specimen quality, but recent studies have contradictory results, and hence, we conducted this study to compare the clinical efficacy and safety of monopolar and bipolar electrosurgical modalities in TURBTs.
Materials and Methods:
A total of 287 patients were enrolled in the study and underwent TURBTs between July 2015 and September 2016. Patients undergoing surgery under general anesthesia and restage procedure were excluded from the study. Patient demographic profile, tumor characteristics, and complications of the procedures such as obturator jerk, bladder perforation, blood loss, need for resurgery, and transurethral resection syndrome were recorded. Tumor specimens were analyzed for stage, grade, deep muscle invasion, and quantity and quality of thermal artifacts.
Results:
A total of 160 patients were block randomized and analyzed with 80 patients in either group. Patient demographics and tumor characteristics were comparable between the groups. Change in hemoglobin levels and incidence of bladder perforation were comparable between the groups. A higher proportion of patients in bipolar group had obturator jerk compared with those in monopolar group, however, it was not statistically significant (24% vs 14%; p = 0.23). A higher proportion of patients in bipolar group did not have thermal artifacts when compared with monopolar group (27.5% vs 5%; p < 0.0001).
Conclusions:
The operative risks of bipolar TURBT such as obturator jerk, bladder perforation, and blood loss are comparable with monopolar resection. However, less thermal artifacts in tissue samples obtained with bipolar resection may be helpful to the pathologist in interpretation of histopathologic findings.
Introduction
Monopolar cautery is commonly used for transurethral resection of bladder tumor (TURBT). During monopolar resection, activated current may cause stimulation of obturator nerve leading to contraction of the adductor muscle and bladder perforation. 1 Moreover, if the irrigation fluid gets absorbed into systemic circulation, increased uptake of the irrigation fluid can lead to overhydration, which may cause transurethral resection (TUR) syndrome. 1 In bipolar energy due to the modified current flow, the use of nonconducting irrigation fluid is not necessary and physiologic saline irrigation reduces the incidence of TUR syndrome. 2 In bipolar resection, the patient does not constitute a direct part of the current circle as the impedance of the patient is higher than that of the irrigation fluid. 3 Problem with older bipolar systems occurred due to smaller and thinner resection loops, which may cause prolongation of operating time. 4 Favorable results of bipolar TURBT include lower risk of TUR syndrome, better hemostasis, and shorter hospital stay. 5 However, recent studies have shown that bipolar TURBT was not superior to monopolar resection with respect to obturator reflex and bladder perforation. 6 –8 Quality of the biopsy specimens depends on multiple factors such as the energy used, location of the tumor, and surgical skill. 6 Bipolar energy has the propensity to cause less thermal damage to tissues during TURBT compared with monopolar energy, but recent studies have shown contradicting results. 1,7 To address these issues, we compared the clinical efficacy and safety of these two electrosurgical modalities in TURBT and the impact on thermal artifacts and damage.
Materials and Methods
Study design and patient selection
Following approval from the institute ethics committee, patients undergoing TUR of bladder tumor between July 2015 and September 2016 at our institute were included in the study. Written informed consent was obtained from all participants.
Inclusion criteria
Patients with bladder tumor undergoing TURBTs under regional anesthesia.
Exclusion criteria
All those patients undergoing restage TURBTs, those requiring general anesthesia, and those who refused to give informed consent were excluded from the study.
Methods
Patients with bladder tumor were randomized into two groups using block randomization method with each block comprising 10. Allocation was concealed in a sealed envelope and implemented by an operating room technician after administration of regional anesthesia. Patients, pathologists, and statisticians were blinded regarding allocation.
All patients underwent surgery under spinal anesthesia, no epidural anesthesia was used. Isobaric bupivacaine, 0.5%, was the anesthetic agent used. Patients were placed in lithotomy position once the anesthetist ensures sensory blockade was effective till the level of umbilicus. Three consultants performed the procedure, of which one had around 20 years experience and the other two had 10 years experience. Others were residents with 2 to 3 years experience. Consultants were present in the OT observing the entire procedure when TURBT was performed.
Bipolar TURBT was performed by using bipolar electrocautery. A 26F resectoscope and angled loop wire were used for bipolar resection. For cutting, power setting was 160 to 200 W and for coagulation 100 to 120 W with automatic adjustment according to tissue thickness. Isotonic saline was used as irrigant during resection. Monopolar TURBT was performed using a standard 26F resectoscope with power setting and energy levels of 70 to 90 W for cutting and 30 to 40 W for coagulation. Glycine was used as irrigant. At the end of the procedures, a 22F three-way Foley catheter was placed and saline irrigation was continued as required. The catheter was removed after the urine was clear for 24 hours.
All resected specimens were submitted in formalin to the department of histopathology. Histopathologists evaluated the tissues for tumor stage, grade, muscle invasion, and thermal damage. All pathologic results were reevaluated by one senior uropathologist. Thermal damage was quantified into three grades according to the quantity of thermal artifacts. Grade 1 is defined as thermal artifacts involving less than one-third of the entire specimen. Tissues with one-third to two-thirds thermal artifacts were categorized as grade 2, and tissues with more than two-thirds thermal artifacts were categorized as grade 3. Thermal damage was also qualitatively analyzed according to the following grades. Grade 0 is defined as no thermal damage. Grade 1 included those specimens where cellular structures were identifiable and not impaired. Grade 2 included those with impaired cellular structure and nuclei but readable with difficulty, and grade 3 included those with complete loss of cellular architecture and not readable. The second thermal artifact was defined as the second-most common thermal damage found in tissue.
Study variables
Primary study outcomes assessed were incidence of obturator jerk and bladder perforation. Bladder perforation was defined subjectively by surgeon when perivesical fat was seen during TURBT. Change in hemoglobin and sodium levels, clot retention, need for blood transfusion, TUR syndrome, and resection time were also compared. Bladder tumors located in lateral wall were considered for calculating incidence of obturator jerk. The secondary endpoints were quantity and quality of cautery artifacts in the tissue specimens in both groups.
Statistical analysis
A minimum sample size of 50 in each group was computed using a power of 80%, with a confidence level of 95%. 7 When the sample size reached 80 in each group, power of the study increased to 95%. Sample size was calculated using obturator jerk incidence rate, which was around 25% in monopolar TURBT (MTURBT) and 5% in bipolar TURBT (BTURBT) in standard literature review. 7 We have not calculated the effect size, which could be a limitation. All data were statistically analyzed by using the statistical software SPSS version 22 (SPSS, Inc., Chicago, IL). Unpaired Student's t-test was used to compare mean values of continuous variables, whereas the chi-square test and Fischer's exact test were used to compare categorical variables. Mann–Whitney U test was used for skewed data. p-Value less than 0.05 was considered statistically significant.
Results
Two hundred eighty-seven patients underwent TURBTs during the study period. After exclusion, 160 patients were included in the study. Statistical analysis was done for a total of 80 patients in the bipolar group and for 80 patients in monopolar group. Patient screening, allocation, and analysis are summarized in the CONSORT diagram (Supplementary Fig. S1; Supplementary Data are available online at
Both groups were comparable for their demographic and baseline variables (Table 1). Tumor characteristics between the groups were also comparable (Table 2). Urothelial carcinoma was the most common histologic bladder tumor subtype in both groups. Distribution of various histologic types of bladder tumor was not statistically significant (p = 0.43). The proportion of patients with different tumor grades was comparable between the two groups (p = 0.734). In BTURBT group, mean change in hemoglobin was 0.27 ± 0.309 g/dL, while it was 0.26 ± 0.329 g/dL in MTURBT group (p = 0.961). Mean change in serum sodium was 0.478 ± 2.16 meq/dL in BTURBT group, while it was 0.375 ± 2.67 meq/dL in MTURBT group (p = 0.967). None of the patients had TUR syndrome and there was no need for blood transfusion in both groups.
Comparison of Demographic and Baseline Data Between the Groups
Independent samples t-test.
Chi-square test.
Comparison of Tumor Characteristics Between the Groups
Chi-square test.
Mann–Whitney U test.
Complications and hospital stay between the two groups were compared (Table 3). Although more number of obturator jerks occurred in BTURBT group, the difference was not statistically significant (p = 0.242). When only tumors located in the lateral wall were used as a denominator for analysis of obturator jerk, 13/54 (24%) patients in bipolar and 8/57 (14%) in monopolar group had obturator jerk. This difference was not statistically significant (p = 0.227). Only one patient from monopolar group had grade 3 Clavien–Dindo complication requiring clot evacuation under spinal anesthesia. Apart from this, none of the patients in either group required blood transfusion or immediate intervention (grade 1 Clavien–Dindo complication). Quantity and quality of thermal artifacts were compared between the two groups in TURBT chips and deep muscle biopsy (Tables 4 and 5). A higher proportion of patients' tumor specimen in bipolar group did not have thermal artifacts compared with monopolar group (27.5% vs 5%; p < 0.0001).
Comparison of Complications and Hospital Stay
Chi-square test.
Fischer's exact t-test.
Independent Student's t–test.
Mann–Whitney U test.
Thermal Artifacts in Transurethral Resection of Bladder Tumor Chips
Chi-square test.
TA = thermal artifacts.
Thermal Artifacts in Deep Muscle Biopsy
Chi-square test.
Discussion
Bipolar energy has recently upsurged as a modality of choice for TURBT. The main advantages of bipolar electrocautery are the ability to cut clean, reduced tissue charring, and clear vision due to use of physiologic saline. Studies had shown that bipolar TURBT is almost devoid of TUR syndrome. 9 –11 In our study also, TUR syndrome was not encountered in any of the patients. Another potential benefit of bipolar resection is decreased blood loss because of better hemostasis. 12 –15 Similar to other studies, 7,8,12 in our study also, none of the patients required blood transfusion in either of the groups.
A major concern during bladder tumor resection is obturator jerk, which may cause perforation of the bladder. The incidence of obturator jerk during monopolar TURBTs ranges from 1.7% to 11%, 15 –17 but seems to be underreported in the literature if not accompanied by a serious complication. In the RCT by Venkatramani and colleagues, 7 when only lateral tumor was taken as denominator, incidence of obturator jerk was 49% in monopolar group and 60% in bipolar group. Similarly in our study, the incidence of obturator jerk was 24% and 14% in bipolar and monopolar groups, respectively. However, the difference was not statistically significant. Although previous studies 4,12 have claimed bipolar resection reduces obturator jerk (<5%), this was not observed in our study because there was automatic energy setting variation according to the tissue character during bipolar resection. Maybe bipolar resection at lower energy setting can overcome this drawback as shown by Gupta and colleagues, 12 but according to our experience this may not be feasible as settings need to be adjusted according to the individual patient, and satisfactory resection may be difficult at a lower setting.
In a study done by Ozer and colleagues, 8 bladder perforation was more in bipolar group (23%) than in monopolar group (8%), but in the study done by Venkatramani et al., 7 the incidence of bladder perforation was 16% in both monopolar and bipolar groups. The resection loop during bipolar activation gets warmer than during monopolar before initiating resection, and hence, more chances of eliciting obturator jerk and perforation during BTURBT. 8 However, in our study, patients in BTURBT group (1.2%) had lower incidence of bladder perforation when compared with MTURBT group (5%). Although the incidence of bladder perforation was lower in our study, the difference was not statistically significant.
Cautery artifact has been reported to be more with monopolar resection. 18 –21 However, recent studies have not shown any significant difference in the occurrence of cautery artifacts in monopolar resection when compared with bipolar resection. 6,22 It is the usual experience to have clean cutting with bipolar energy, clear vision due to resection in physiologic saline, and plasma vaporization of tissues during bipolar resection (Fig. 1). Del Rosso et al. 9 stated that they experienced clean cutting and reduced charring of tissue during bipolar TURBT, which resulted in a significantly lower incidence of thermal artifacts in bipolar resection. There are only few randomized studies comparing cautery artifacts in the specimens obtained by bipolar and monopolar resection. 7,16 In our study, 22 (27.5%) patients in BTURBT group did not have any degree of thermal artifacts compared with 4 (5%) patients in MTURBT group. The proportion of patients having quantitative thermal artifacts was significantly more in MTURBT group (p < 0.0001). There are only few studies 1,6,22 in the literature comparing quality of thermal artifacts between monopolar and bipolar resection. In these studies, there was no significant difference with respect to quality of thermal artifacts. Because the qualitative grading of thermal artifacts is not standardized in the literature, there is a need for developing consensus regarding the classification of thermal artifacts. In our study, we also compared the quality of thermal artifacts. Proportions of patients having qualitative thermal artifacts were also significantly more in MTURBT group (p < 0.0001).
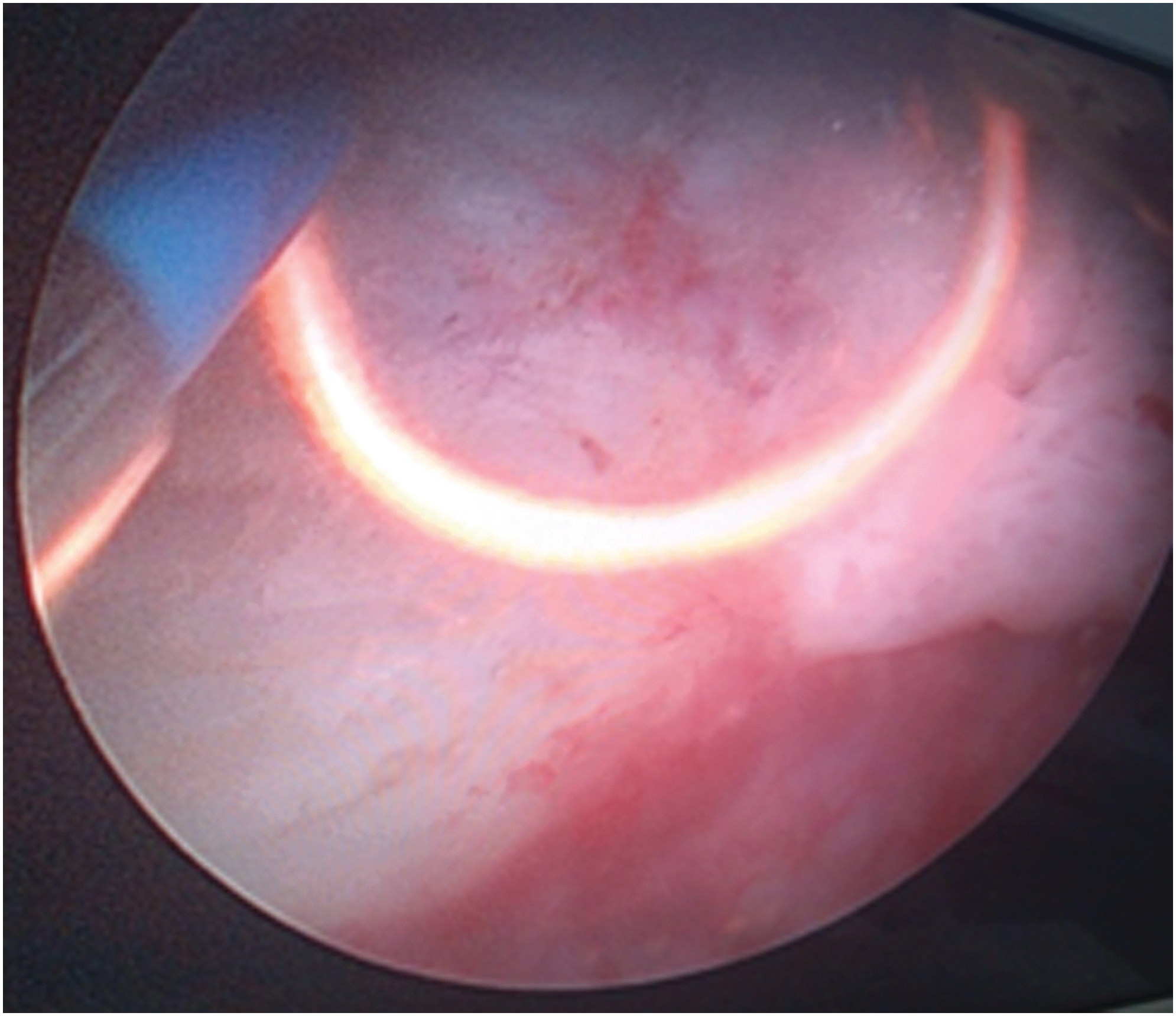
Bipolar resection producing plasma vapor during cutting.
We also compared the degree of thermal artifacts in deep muscle biopsy and found that both quantity and quality of thermal artifacts were significantly more in monopolar group (p = 0.0028). Other studies have shown variable results regarding the presence of thermal artifacts in deep muscle biopsy. 6,7 Yang and colleagues 6 did not have significant statistical difference in the grades of thermal damage in deep muscle biopsy when compared between the monopolar and bipolar groups, but Venkatramani and coworkers 7 showed significantly lower grades of thermal artifacts in deep muscle biopsy in bipolar group compared with monopolar group.
To our knowledge, this is the first study to compare the presence of second thermal artifact in bladder tissue specimen. Thirty-five (43.8%) patients in BTURBT group had the presence of second thermal artifact in their total specimen compared with 50 (62.5%) in MBURBT group. Although the presence of a second thermal artifact was higher in MTURBT group, the difference was not statistically significant. Grade 3 thermal artifacts if present in smaller resection volume can pose diagnostic difficulty when compared with grade 1 and 2 artifacts (Fig. 2A–C). However, unless pathologic grading of thermal artifacts is standardized, the relevance of reporting them is of doubtful clinical significance.

Conclusions
The operative risks of bipolar TURBT such as obturator jerk, bladder perforation, and blood loss are comparable with monopolar TURBT. However, less thermal artifacts in tissue samples obtained with bipolar resection may be helpful to the pathologist in interpretation of histopathologic findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.