
Abstract
Objective:
To determine the time to specialist urologic consultation and definitive management after establishing a subspecialist administered acute stone clinic (ASC) for adults with symptomatic upper tract stones in a publically funded universal healthcare system.
Materials and Methods:
We retrospectively reviewed 337 adult referrals for stone management. Three distinct 9-week periods were assessed. Group 1 patients were seen/treated by their individual urologist before inception of a general urology emergency clinic (pre-EC). Group 2 patients were seen in a pooled EC and Group 3 patients were seen in the ASC.
Results:
A total of 337 patients (75, pre-EC; 91, EC; 171, ASC) were reviewed. Mean time to consultation for pre-EC, EC, and ASC cohorts was 29, 7, and 7 days, respectively (p < 0.05), whereas loss to follow-up decreased from 13% to 5% (p < 0.05). On average, the number of patients seen per week increased from 9 to 20. Mean time to stone surgery from date of referral was 75 days pre-EC, 43 days EC, and 25 days ASC (p < 0.05). The percentage of patients undergoing surgery was between 59% and 63% per cohort; however, the number of patients increased from 5 to 11 per week.
Conclusions:
By reorganizing clinical resources, a dedicated ASC was able to increase patient capacity, reduce time to urologist consultation and reduce surgical wait times.
Introduction
A
To improve our acute stone care delivery, we built upon acute care surgery (ACS) models that have gained rapid popularity in the general surgery literature. 7 –9 Canada is an innovator in evaluating ACS models for improving access to care and definitive treatment for presentations ranging from acute appendicitis to bowel obstructions. To date, their remains a paucity of publications examining ACS models in urology. Abstract results from Golda et al. of Toronto, Canada, were presented at the 2017 Annual Canadian Urological Association (CUA) Meeting in which they developed an acute care urologist to triage general ER consultations and to minimize on call urology cases. 10 By reorganizing access to acute care, they advocated for additional operating room (OR) resources to manage more patients in a cost neutral way. 10
With the goals of efficient throughput from primary diagnosis to urologic consultation/surgery and improved follow-up, an acute stone clinic (ASC) was established at our center in 2014. This involved pooling individual urologists' resources, to create a shared infrastructure, including centralized referrals, triaging, and expedited access to surgical management. The anticipated benefits of this system were to reduce wait times for consultation, whereas minimizing protracted courses of renal colic experienced by delayed surgical management and loss to follow-up.
The Division of Urology at the University of Alberta has 16 members delivering adult urologic care. Our center services ∼3 million people living in the northern half of the province of Alberta in Canada. In 2009, urologists on call (irrespective of subspecialty) triaged their own stone consults and scheduled clinics and surgery accordingly. In 2012, this approach was replaced by a general urology emergency clinic (EC) that was developed to facilitate prompt outpatient urologic follow-up for emergency referred consultations. These weekly clinics were not restricted by diagnostic code, and were staffed by the urologists on call. Given that 85% of acute urologic emergency patients were presenting with nephrolithiasis, the need for specialized attention for these patients became evident. Furthermore, with the addition of a new endourology fellowship trained staff, the EC was replaced with an ASC.
The ASC established a defined screening, consultation, and management system. A stone working group of eight urologists with interests in stone disease (three with fellowship training in endourology) maintains the clinic, and screens/triages all acute and elective consultations. Sources for consultation included emergency medicine (EM), primary care physicians (PCPs), nonstone-focused urologists, and other specialties (endocrinology, nephrology, etc.). Pooled clinic and OR time were distributed among the stone working group, with a target of two acute stone-dedicated clinics, as well as two acute stone ORs per week.
To evaluate the ASC effect, a retrospective chart review commenced to compare access to urologic care and subsequent management in the ASC.
Materials and Methods
After receiving institutional review board approval, we retrospectively reviewed the charts of three patient cohorts who were referred for urologic consultation regarding their symptomatic upper urinary tract stones in Edmonton, AB, Canada. Group 1 (pre-emergency clinic [pre-EC]): includes patients who were seen by eight urologists during 9 consecutive weeks (February 2009) before inception of a general urology EC. Group 2 (EC) patients were seen during 9 consecutive weeks starting in February 2012 after creating the EC, and Group 3 (ASC) patients were seen over 9 consecutive weeks after establishing the ASC (February 2015). Of note, we selected eight pre-ASC staff to examine an equivalent number of urologists to the number involved with the ASC, excluding those who were not seeing stone consultations.
As our primary outcome, we assessed the mean time to urologic consultation from the date of initial referral (days). Secondary outcomes were the mean time from initial referral to treatment of the referred acute stone(s) (days), proportion of patients with complete follow-up, and number of patients lost to follow-up.
Continuous variables are expressed as mean and range, whereas proportions were used for categorical variables. GraphPad Prism (v6.0, Inc., La Jolla, CA) was used for our statistical analysis including one-way ANOVA with Tukey's multiple comparisons test set to a significance of 0.05 (95% confidence interval).
Results
Population characteristics
In the 27 total weeks analyzed (9 pre-EC + 9 EC + 9 ASC), 353 adults with acutely symptomatic upper urinary tract stone consultations were reviewed. Of these, 337 patients were included as the denominator in our final analysis. The 16 patients who were excluded did not have an acute stone requiring expedited consultation (n = 6), or did not have reviewable data (n = 10).
Of the 337 patients reviewed, the mean age was 50 years old (range: 18–93 years old), and 65% were male, with no significant differences between cohorts. Fifty percent of patients lived in urban areas, with the remaining half living a mean distance of 128 km outside of the city (67% lived ≤100 km, 16% 100–200 km, 8% 201–400, and 9%> 400 km away). Six percent of the patients lived >3 hours away from our tertiary care center. Forty-two percent of our patients were recurrent stone formers (Table 1).
p > 0.05 between all cohorts for all patient characteristics.
ASC = acute stone clinic; EC = emergency clinic; pre-EC = pre-emergency clinic.
Efficiency of patient consultations
The proportion of emergency physician to primary care referrals showed that pre-EC referrals were mostly from PCPs (52%), whereas the majority of EC referrals were from the emergency department (91%), and the ASC fell between the two (71% ER, 25% PCP) (Fig. 1).
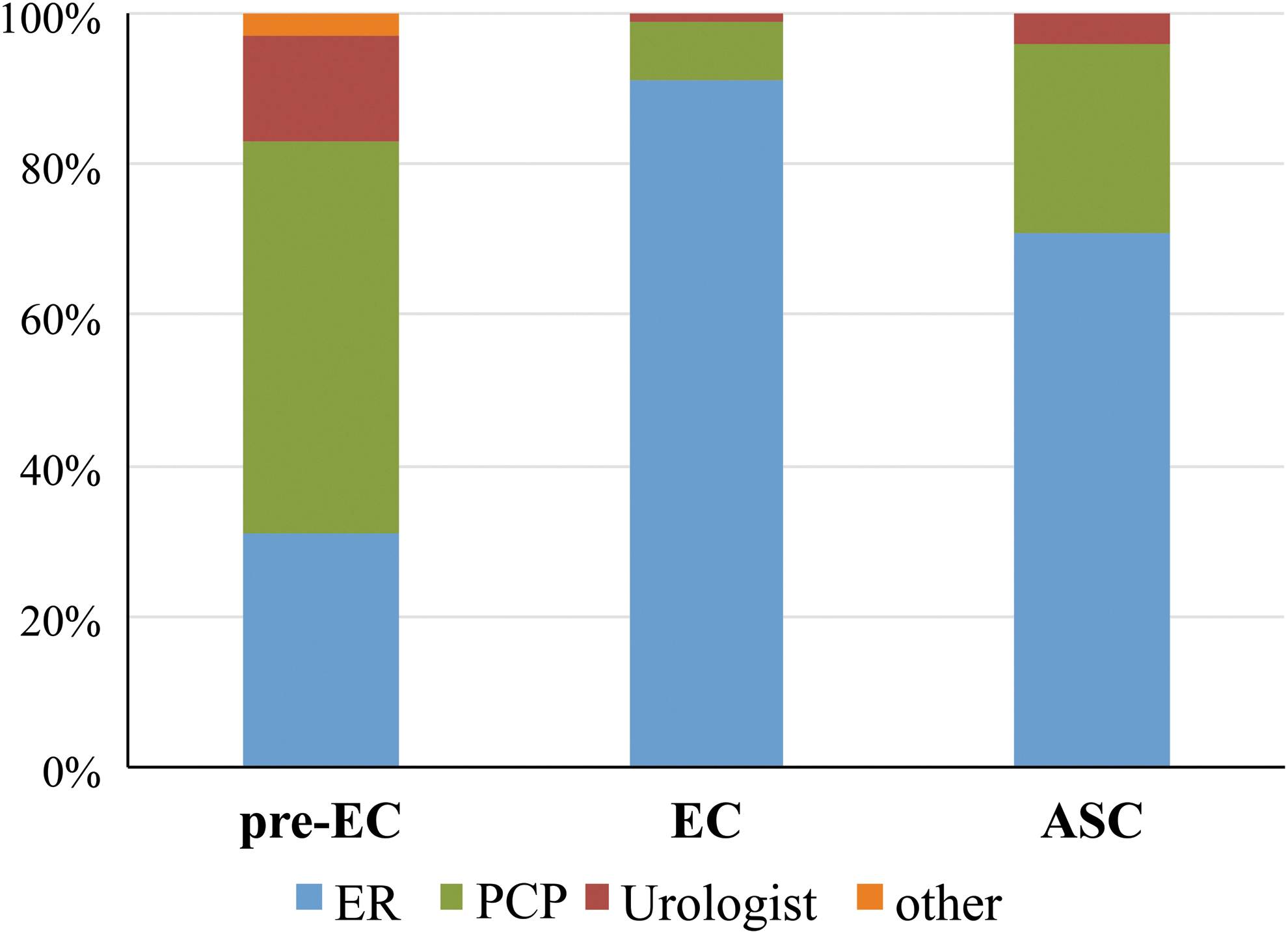
Referral sources for acute stone consultation for pre-EC, EC, and ASC cohorts. p < 0.05 between all cohorts for ER, PCP, and urologist referrals, p < 0.05 between pre-EC and EC or ASC for other referrals. ASC, Acute Stone Clinic; EC, emergency clinic; ER, emergency; PCPs: primary care physicians; pre-EC, pre-emergency clinic.
Of the 337 patients, 75 were seen during the pre-EC period, 91 in the EC, and 171 in the ASC. These three cohorts of patients were each collected for 9 consecutive weeks in February 2009, 2012, and 2015. This resulted in an average of 9, 11, and 20 patients seen per week for the pre-EC, EC, and ASC cohorts. The mean time to urology consultation for pre-EC, EC, and ASC cohorts was 29, 7, and 7 days, respectively (p < 0.05 between pre-EC and EC or ASC).
Time to stone treatment
The mean time to definitive stone management from date of referral for the pre-EC, EC, and ASC cohorts was 75, 43, and 25 days, respectively (p < 0.05 between all cohorts) (Fig. 2). Although the percentage of patients treated surgically remained similar (61% pre-EC vs 59% ASC, p > 0.05), the absolute number of patients doubled (46 vs 101).
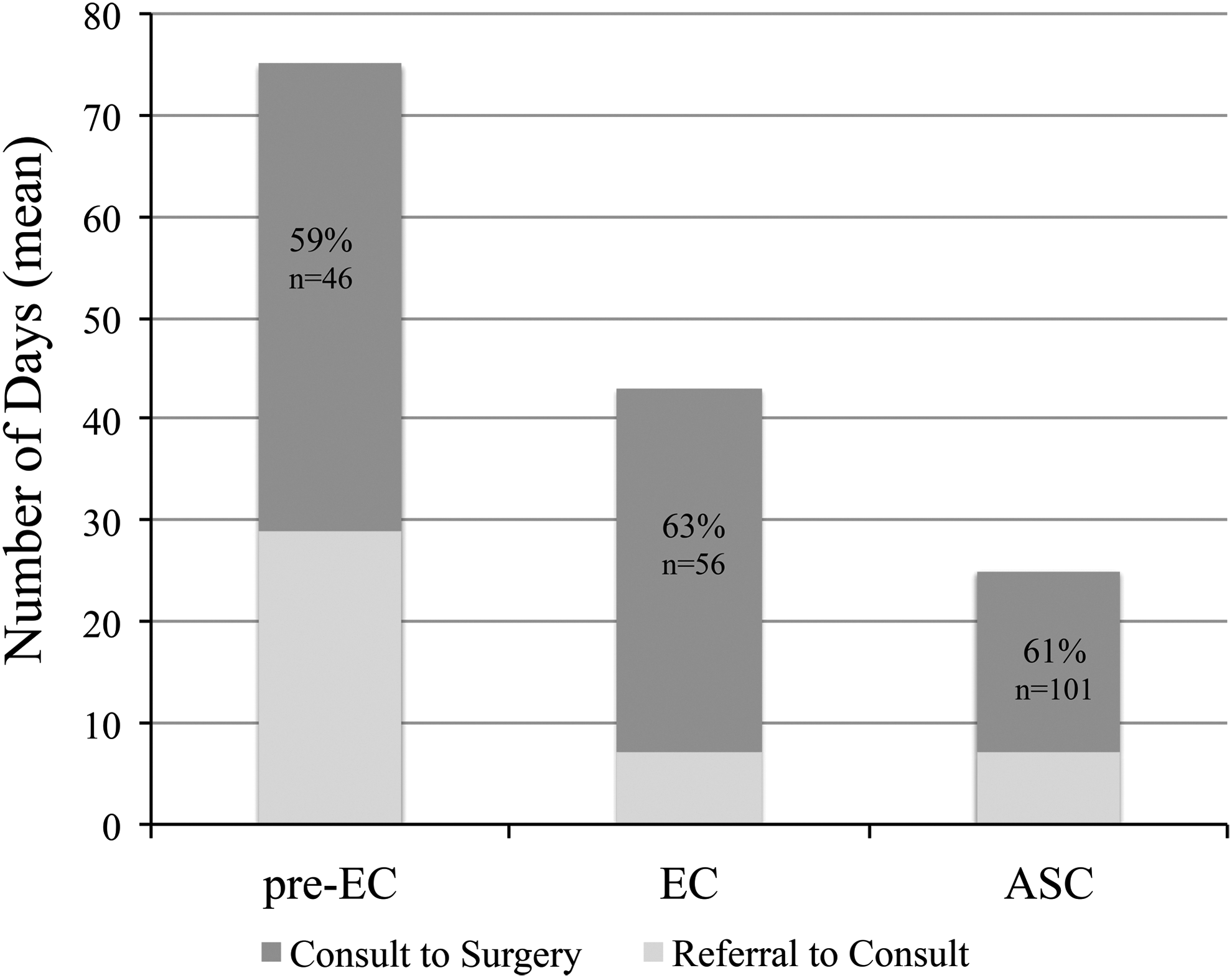
Mean time from referral to consultation to surgery (days) for each of the three cohorts: pre-EC, EC, and ASC. Percentage of patients undergoing surgery stated on each summed bar. Referral to consult: p < 0.05 between pre-EC and EC or ASC, consult to surgery: p < 0.05 between all cohorts.
Management and follow-up
Sixty-one percent of patients proceeded to a surgical intervention (ureteroscopy, shockwave lithotripsy, and PCNL) with the majority undergoing ureteroscopy. Table 2 highlights the initial management plan for the entire patient cohort as well as separate cohorts. Other initial management included cystoscopy with retrograde pyelograms to confirm intraluminal calcifications in cases with atypical imaging or radioisotope renography before intervention planning. For patients undergoing observation with follow-up, repeat KUB (if calculus initially observed) and ultrasound or CT with serum creatinine was undertaken 1 to 3 weeks after initial consultation on a case-by-case basis. Medical expulsive therapy with tamsulosin 0.4 mg per os (PO) daily was maintained along with adequate PO fluid intake and as needed PO analgesics, stool softeners, and antiemetics. All of these patients received a follow-up appointment 1 to 4 weeks after their initial consultation.
p < 0.05 between pre-EC and ASC for PCNL, p > 0.05 between all cohorts for all remaining management plans.
F/U = follow-up; PCNL = percutaneous nephrolithotomy, PRN = pro re nata (as needed); SWL = shockwave lithotripsy.
A total of 31 patients were lost to follow-up or the referred stone was not resolved at last contact (10 pre-EC, 12 EC, and 9 ASC). The characteristics of the patients lost to follow-up in each of the three cohorts are outlined in Table 3. A smaller proportion of patients were lost to follow-up after establishing the ASC vs the pre-EC and EC cohorts (5% ASC vs 13% pre-EC and 13% EC, p < 0.05 between ASC vs pre-EC/EC). In addition, the mean stone size of patients lost to follow-up after establishing ASC decreased to 5 mm from 11 to 12 mm previously.
p < 0.05 between ASC and pre-EC or EC for number of patients, pre-EC and EC or ASC for mean time to consultation.
ER = emergency; PCP = primary care physician.
Discussion
In this retrospective cohort analysis of 337 consults to urology for urgent management of symptomatic nephrolithiasis, we found that by reorganizing existing resources to create an organized ASC, we improved access to subspecialist care, while expediting delivery of clinical and surgical care.
At our center, inpatient/ER ASC consultation at the academic hospitals would first be triaged by around the clock urology resident coverage. At community hospitals or PCP clinics, referring physicians directly consult the adult urologists on call. Once the urology team receives the case details and accepts the ASC referral, the referring physician faxes a standardized referral to a central ASC number. All faxed consults are reviewed by one of the triaging ASC staff covering stone intake that day. This ASC urologist distributes patients into upcoming ASC appointments based on urgency of anticipated treatment. Preliminary management plans are documented on the ASC patient electronic record to maximize the efficiency of the ASC clinics. Patients receive prompt notification of an appointment with their assigned stone working group urologist.
Transitioning to the ASC, an observed change in the sources of referrals was noted. In addition, the efficiency of patient consultations improved, allowing more patients to be seen by a urologist with an interest in urinary tract calculi on a weekly basis. The ASC also enabled significant improvements in both time to consultation and time to definitive stone management. In establishing a dedicated clinic with centralized intake and triaging, we reduced the number of patients lost to follow-up.
The makeup of physicians referring stone patients shifted between cohorts, as PCPs were the predominant referral source in the pre-EC period (52%). The proportion of referrals from PCPs decreased to 8% in the EC and increased to a quarter of the ASC consults. This is likely explained by the EC being primarily populated with consults from EM physicians contacting urologists directly on call, with a possibly biased perception of acuity for most EM referrals leading to prompt consultation vs PCP referrals. When faxes and letters from PCPs were received during this period, those patients were seen in each urologist's elective clinics, usually resulting in longer wait times than if a patient presented symptomatically to the ER. Another contributing factor may be that with streamlined triaging, PCPs no longer send their patients to the ER in an attempt to expedite work-up and access to urologists when symptomatic stones are diagnosed. Furthermore, with reliable and rapid access to stone specialists, ER physicians are less likely to send patients home without follow-up, or back to PCPs who would be responsible for follow-up referral. Taken together, we feel the current ASC allows appropriate and level triaging based on objective need for urgent consultation and management, irrespective of the referral source.
Between 2009 and 2015, we increased throughput of acute stone patients at our center by 228%. This was accomplished by replacing the traditional model of individual urologists booking their consults with a subspecialty stone clinic, all without changing the number of weekly clinics. Although limited, prior publications have examined efforts to optimize management pathways, highlighting that unifying scheduling and referral processes for outpatient follow-up is crucial. 11 The Committee on Quality of Health Care in America identifies five major barriers to specialty surgery follow-up, one of which is standardization of scheduling processes. 11,12 In comparing the findings from 2015 (reported in this study) to our present ASC throughput in 2016 (at time of publication), we have seen a continued increase to a mean of 115 patient consultations per month (28 per week), equivalent to a 145% increase for one and a half years or +322% since 2009.
With the initiation of the standardized ASC, a 75% improvement in time from referral to consultation (29 vs 7 days) has been achieved. After establishing the ASC, a 60% reduction in patients lost to follow-up after consultation (from 13% to 5%) was noted, with a trend toward smaller “safer” stones (5 mm ASC vs 11 to 12 mm EC). In addition, after initiating the ASC, we received anecdotal positive feedback from ER physicians that we hope to objectively examine in a follow-up study. We will examine our ER physicians' awareness of the ASC and satisfaction with referring acute symptomatic upper tract urinary calculi to urology before and after establishing the ASC. In addition, we look to improve the number of patients lost to follow-up after ER presentation as well as the number re-presenting to the ER while awaiting outpatient consultation.
The ASC has dramatically improved the time to definitive stone management at our center. Regionally, wait times of <2 weeks were deemed “best practice” for patients with symptomatic/obstructing ureteral stones. Despite our significant improvements in time to consultation and definitive treatment, our current mean time to surgical intervention (25 days) remains 78% more than our 14-day goal. Similarly, 18% of patients undergoing definitive surgical intervention are receiving it beyond the 14-day recommended time frame. This emphasizes that in order for our care pathway to be effective, the improvements we have made in consultation capacity must be matched by access to surgical resources.
This study highlights the impact of reorganizing and optimizing the utilization of existing resources. We have quantified important milestones, which help guide expectations of all parties involved with these patients. Given that 20% of ER visits for flank pain are because of renal colic, 1 and 11% of these patients return to the ER within 30 days, 13 our aim is to optimize our involvement to decrease the burden on primary and acute care resources.
Limitations of this study include variable data records and nonstandardized evaluations because of its retrospective design for three cohorts (2009, 2012, and 2015). In addition, we did not have access to all outcome data (i.e., stone-free rates). Also, the generalizability of our results may be limited given Canada's single payer public system, and our center's unique position of being the only urology practice for an extremely large geographic area (Edmonton catchment area primarily one province and one territory, 1.17 × 106 km2).
Recently we initiated a prospective stone registry to follow our ASC patients, furthering our understanding of administrative and clinical outcomes. Through this, we hope to continue evolving our ASC. As a surgical specialty in a resource-strained healthcare system, our goal is to enhance the efficiency of resource allocation, while maximizing patient volume and reducing wait times to acceptable levels.
This study shows that with reorganization of an institution's resources, an ASC can provide vast improvements in accessibility, with shorter times to consultation and treatment. Further analysis is required to understand the associated clinical outcomes experienced with these administrative changes.
Conclusions
By reorganizing clinical resources, a dedicated ASC was able to increase patient capacity, reduce time to urologist consultation and reduce surgical wait times.
Footnotes
Acknowledgments
We would like to acknowledge and thank all members of the ASC working group: Dr. T. Wollin, Dr. T. Schuler, Dr. S. De, Dr. D. Bochinski, Dr. H. Evans, Dr. K. Rourke, Dr. N. Jacobsen, and Dr. M. Hobart.
Author Disclosure Statement
No competing financial interests exist for M.A.A., S.D., T.D.S., and T.A.W. Dr. Bochinski reports nonfinancial support from Sanofi, nonfinancial support from Boston Scientific, nonfinancial support from Eli Lilly, and nonfinancial support from Mylan, outside the submitted work.