
Abstract
Introduction:
Cystinuria is a genetic disorder marked by elevated urinary cystine excretion and recurrent cystine nephrolithiasis. Interestingly, despite seemingly similar contralateral renal anatomy, a subset of cystinuric patients consistently form stones in only one kidney. The aim of this study is to evaluate clinical outcomes in unilateral vs bilateral cystine stone formers.
Patients and Methods:
We performed a retrospective case–control study of cystinuric patients evaluated and treated at the University of California, San Francisco between 1994 and 2015 and categorized patients as either unilateral or bilateral stone formers. Clinical presentation, baseline patient demographics, stone procedures, medical therapy regimens, and long-term renal function were compared between the two groups.
Results:
A total of 42 cystine stone patients (22 female, 20 male) were included in the analysis. The median age at first presentation was 18.5 years and median age at study conclusion was 45.5 years. Two-thirds of patients (n = 28) had a history of bilateral stones, whereas one-third (n = 14) had unilateral stones. Medical therapy regimens were similar between groups. Despite an increased average number of lifetime surgeries (7.5 sessions for bilateral vs 3.7 sessions for unilateral, p < 0.05), there was no significant difference in medians of the most recent glomerular filtration rate when compared with unilateral stone formers (81.5 vs 95 mL/min, respectively; p = 0.28).
Conclusions:
The majority of cystinuric patients within our cohort form stones bilaterally during their lifetime, and require more surgical interventions than unilateral stone formers. Despite this, overall renal function is well preserved in unilateral and bilateral cystinuric stone formers treated with minimally invasive stone extraction procedures.
Introduction
C
Despite the life-long and systemic nature of cystinuria, a subset of cystinuric patients only form stones in one kidney, despite no obvious differences when compared with contralateral renal anatomy. 3 The aim of this study was to determine baseline characteristics and clinical outcomes of unilateral vs bilateral cystine stone formers.
Patients and Methods
We performed a retrospective case–control study of all cystinuric patients evaluated and treated in at a university-based stone clinic (University of California, San Francisco or UCSF) between 1994 and 2015 after obtaining the Institutional Review Board approval (CHR No. 14-4533). Patients with at least two clinical visits and a confirmed history of cystine nephrolithiasis were included in the analysis. For all patients, a diagnosis of cystinuria was confirmed by routine laboratory stone analysis of ex vivo stone specimens obtained after stone passage or stone extraction procedures. Laterality of stone disease was determined by comprehensive review of all imaging studies, radiology reports, operative reports, and clinic notes. Patients were then categorized into two groups: unilateral (history of cystine stone formation in only one kidney) and bilateral (history of cystine stone formation in both kidneys). Baseline characteristics, including demographic data, clinical presentation, lifetime stone procedures, and current cystinuria medication regimens were obtained for each group.
Clinical outcomes were evaluated by comparing need for operative intervention and long-term renal function. Procedures were only included in the analysis if they were performed for stone removal; these included percutaneous nephrolithotomy (PCNL), ureteroscopy (URS), shockwave lithotripsy (SWL), and open stone surgery. Stone-related procedures, such as percutaneous nephrostomy tube placement, ureteral stent insertion, or diagnostic cystoscopy were not included in the analysis. Cystinuria duration was defined as the time from initial diagnosis through January 1, 2017. Follow-up duration was defined as time from first presentation at our institution through January 1, 2017. Long-term renal function was determined by glomerular filtration rate (GFR) obtained at initial presentation compared with GFR obtained at the most recent follow-up. Baseline characteristics and clinical outcomes were evaluated through comparative statistical analyses utilizing Chi-squared test, Fisher's exact test, Student's t-test, and Mann–Whitney U-test using Stata version 14.1 (StataCorp, College Station, TX).
Results
A total of 42 cystine stone patients (22 females, 20 males) met criteria and were included in the analysis. The majority of patients were Caucasian and median body mass index (BMI) was 28.6 kg/m2. The median age at the first presentation was 18.5 years [interquartile range (IQR): 13–30 years], the median age at study completion was 45.5 years (IQR: 28–63 years), and the median disease duration since diagnosis was 17.5 years (IQR: 12–31 years). Most (n = 33, 78.6%) cystinurics experienced their first stone event at an age ≤30 years. The most common presenting symptoms were flank pain (62.0%), recent stone passage (24.0%), hematuria (3.5%), urinary tract infection (3.5%), acute renal failure (3.5%), and urinary retention (3.5%). The median follow-up period within our institution was 8.8 years. Family history was available in 40 (95.2%) patients and revealed a positive history of stone disease in first-degree relatives of 42.5% of the patients (Table 1). Detailed family medical history was unknown for two adopted patients and we did not differentiate between cystine and noncystine stones for family history.
Statistically significant difference.
BMI = body mass index; IQR = interquartile range; UTI = urinary tract infection.
Of the 42 patients, 28 patients (66.7%) had bilateral stones, whereas 14 patients (33.3%) developed unilateral stones. Among the unilateral stone formers, nine patients experienced stones solely on the left side, and five patients exclusively experienced stone on the right side. Staghorn stones in at least one kidney were present in 14 patients (33.3%). These included 11 bilateral stone formers and three unilateral stone formers. Bilaterality of stone formation did not significantly correlate to gender (p = 0.38), age of first presentation (p = 0.84), presenting symptoms (p = 0.60), BMI (p = 0.07), presence of Staghorn stone (p = 0.31), or family history of stone disease (p = 0.32). While follow-up duration was comparable between the two groups, median cystinuria follow-up duration was significantly longer in the bilateral stone disease group (20 vs 12 years, p = 0.02) (Table 1).
Collectively, the entire cystinuric cohort underwent 261 lifetime stone removal procedures (median 5 surgeries per patient, IQR: 2–9 per patient). Procedures included 112 (42.9%) PCNLs, 90 (34.5%) URSs with laser lithotripsy and/or basket extraction, 44 (16.9%) SWLs, and 15 (5.7%) open stone surgeries. Figure 1 illustrates the mean number of each procedure type for patients with either unilateral or bilateral cystine stone disease. All open nephrolithotomy and SWL procedures were performed outside of our tertiary care center. Three patients in the bilateral stone group required nephrectomy due to stone-related complications and all of them had at some point formed stones in the contralateral kidney. Two cystine stone patients (4.8%) had reported no stone-related surgery in their lifetimes. One of them experienced bilateral small ureteral stones, which routinely passed spontaneously. The other developed bilateral nephrocalcinosis with frequent passage of small stone fragments. Both patients have been treated conservatively with aggressive hydration and urinary alkalization. Bilateral cystine stone formation was associated with a higher median number of lifetime stone surgeries (6.5 vs 2 sessions, p < 0.05). Bilaterality also correlated with median number of lifetime URS sessions compared with unilateral stone formers (2 vs 1 sessions, respectively; p < 0.05), but there was no significant difference in lifetime need for PCNL (p = 0.55) or SWL (p = 0.35) (Fig. 1).
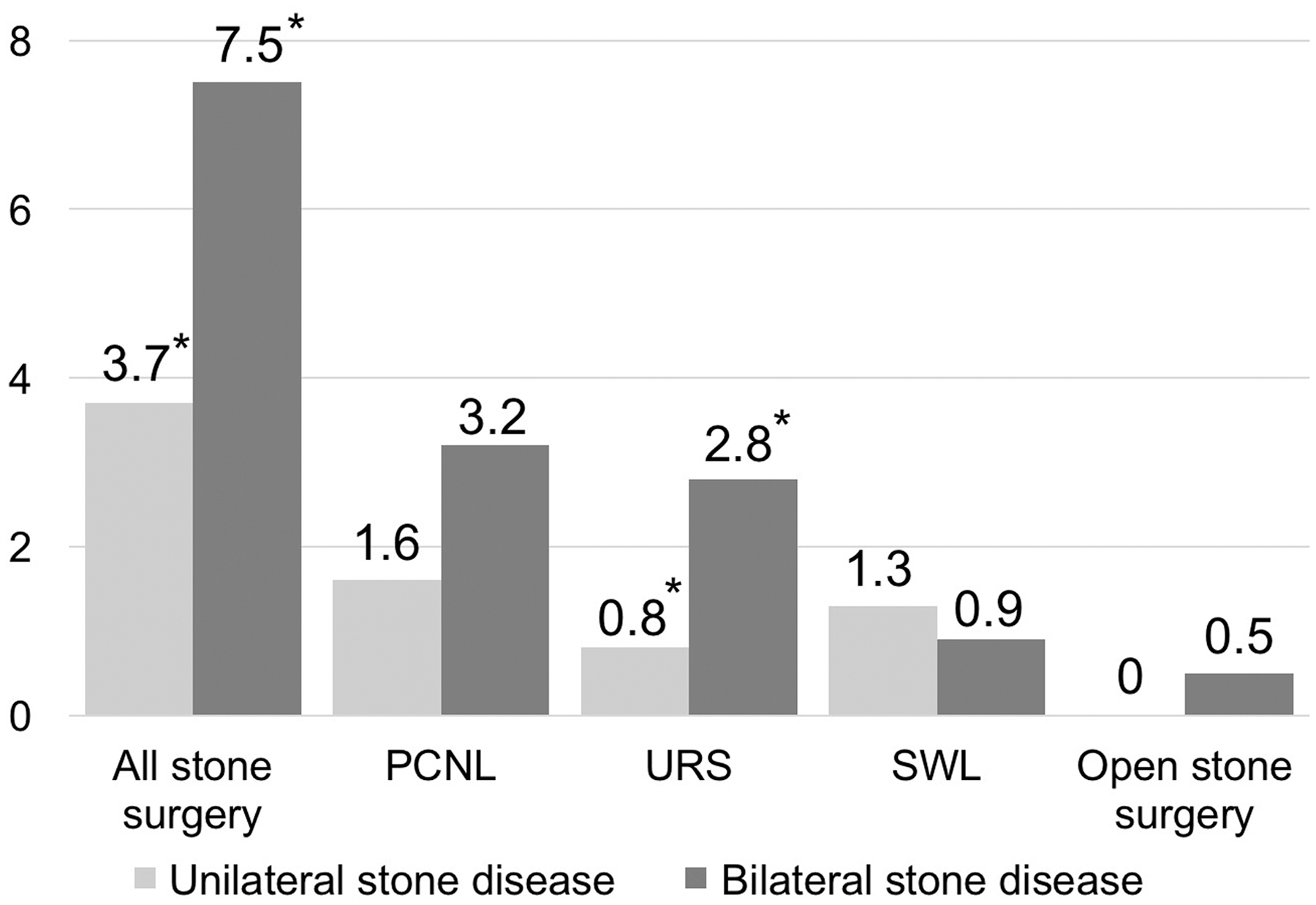
The mean number of surgical interventions for unilateral and bilateral stone disease. The mean number of lifetime stone surgeries was significantly higher in the bilateral stone formers (7.5 vs 3.7 sessions, p < 0.05). PCNL was the most common procedure performed for stone removal, following URS. The mean number of ureteroscopic procedures was also significantly higher in the bilateral stone group (2.8 vs 0.8 sessions, p < 0.05). *Statistically significant difference. PCNL = percutaneous nephrolithotomy; SWL = shockwave lithotripsy; URS = ureteroscopy.
For the entire cohort of cystinuria patients, median GFR at most recent follow-up was 85 mL/min. Median change in GFR from the initial presentation was −2 mL/min. Despite the increased number of lifetime surgeries in patients with bilateral stone formation, there was no significant difference in the median of the most recent GFR when compared with unilateral stone formers (81.5 vs 95 mL/min, respectively; p = 0.28). Furthermore, there was no significant difference in the median change in GFR between groups over the follow-up period (−1 unilateral vs −3 mL/min bilateral, p = 0.64).
Most cystinurics reported taking medical therapy at most recent follow-up; 36 (85.7%) were taking potassium citrate, 11 (26.2%) were on thiol therapy, and 2 (4.8%) patients were receiving
GFR = glomerular filtration rate.
Given the difference in median cystinuria follow-up duration between the two groups, a matched pair subgroup analysis was performed to examine whether duration of disease impacted results. From the original cohort of 42 patients, 14 bilateral stone formers matched to the unilateral stone-forming group for age, gender, and cystinuria disease duration were selected and compared. In this subgroup of patients, median lifetime stone surgery was still significantly higher in bilateral stone formers compared with unilateral stone formers (7.5 vs 2 sessions, p < 0.05), although comparable medication usage and median current GFR were observed (Supplementary Table S1; Supplementary Data are available online at
Discussion
Cystinuria is an autosomal recessive metabolic disorder, with known disruption of dibasic amino acid transporters in both kidneys. Encoding for the defective SLC3A1 (classic cystinuria or type I) or SLC7A9 (nontype I cystinuria) genes is ubiquitously conserved among cystinuric patients. 4 The resulting excessive renal excretion of cystine leads to lifetime recurrent stone events for most patients. 5 However, it remains a curiosity that approximately one-third of cystinuric stone formers only form stones in one kidney. Our cohort (n = 42) demonstrated bilateral stone disease in 66.7% of cystinurics. Similarly, in previous work, we reported a series of cystinurics (n = 34) with a bilateral stone formation rate of 70.6%, 3 and a smaller study (n = 22) of cystinurics from Iran identified bilateral disease in 59% of patients. 6 By comparison, in a generalized sample of calcium-based stone formers, bilateral stone formation is estimated at ∼25% in contemporary series. 7 Certainly, higher rates of bilateral stone disease are expected in cystinurics given the near-constant presence of elevated urinary cystine. Yet, the question remains: why do some patients only form stones in one kidney?
Genotypes, transport gene defects, hydration status, and urine pH should theoretically be similar in each kidney. While it is assumed that the phenotypic distribution of defective transporters is equal in each kidney, this has not been definitively proven. Are some other lithogenic factors present that may influence stone predominance in one particular kidney? One attractive hypothesis is a potential discrepancy of renal blood flow in each kidney, which may result in differences in glomerular filtration, fluid concentrations, cystine supersaturation, and subsequent risk of stone formation. Some have suggested that sleep patterns may be linked to stone laterality in other forms of nephrolithiasis. We have shown that the side of stone was identical to the dependent sleep side in 76% of 110 consecutive patients with unilateral calcium-based stones (p < 0.05). It has been postulated that routinely sleeping on one side may cause subtle alterations to renal hemodynamics or urinary stasis that promote stone formation. 8,9
In reviewing imaging studies from unilateral stone formers, there was no clear evidence that urinary stasis as caused by anatomic or functional abnormalities such as infundibular stenosis, ureteropelvic junction obstruction, impaired ureteral peristalsis, or neuropathic bladder was present as risk factors for stone formation. It is important to point out that most—but not all—patients with cystinuria form stones. Because cystinurics are often diagnosed after symptomatic stone episodes, it remains unclear how many nonstone-forming cystinurics there are in the general population. 5 It remains possible that the actual prevalence of cystinuria is underreported. Perhaps those who form stones carry additional unknown environmental, genetic, or metabolic risk factors.
In the current analysis, cystinurics developed their first stone episode at a young age, with a median age of onset at 18.5 years and 75% of patients experiencing stones by the age of 30 years. These results parallel previous longitudinal studies of cystinuric patients that have demonstrated a strong predisposition to develop symptomatic stone disease during the first three decades of life. 2,3,10
The median age of disease onset and presenting symptoms was not significantly different between unilateral and bilateral stone formers. Our analyses demonstrated that, overall, cystinurics underwent an average of 6.2 procedures from the time of diagnosis through the follow-up period. Similarly, Varda and colleagues reported a pediatric cystinuria series of 23 patients with long-term follow-up indicating a median surgery number of 6 with a median number of 1.0 surgery per year. 10 Smaller series from Korea and Japan, however, have demonstrated a much lower average surgical burden; 2.7 surgeries per lifetime during a mean follow-up period of 5 years in 14 patients, 11 and <0.2 stone events yearly from a study in 31 patients with a mean follow-up period of 7.5 years. 12 The relatively lower surgery or stone event number from these Asian studies may be explained by differences in disease severity, urologic practice patterns, and definitions of stone-related surgery. 12 Certainly, the differences in daily cystine excretion among various races may contribute to variable results in differing racial cohorts. 13 While Caucasians are more likely than other races to be diagnosed with cystinuria, the overall effect of geographic location and race on cystinuria remain poorly elucidated.
In the current study, bilateral stone formers required significantly more sessions of lifetime surgery than unilateral stone formers. Although median duration of cystinuria was higher in the bilateral stone group, this finding still held true with subgroup analysis matched for duration of disease. Bilateral stone formers were also more likely to have Staghorn stones. Yet, overall renal function was well preserved over the course of treatment in all patients, with a median GFR of 85 mL/min at the conclusion of this study. Median change in GFR from the initial presentation was almost nonperceivable at an absolute value of 2 mL/min. Renal function was well preserved in both bilateral and unilateral stone formers (Table 2). No patients in our study progressed to end-stage renal disease (ESRD) or required renal replacement therapy. The long-term renal preservation seen in this contemporary series of cystinurics is encouraging, but should be interpreted with caution. Previous work has warned that adults with cystinuria are at heightened risk for the development of reduced GFR and the development of chronic kidney disease (CKD). In fact, large population-based studies have indicated that all stone formers, not just cystinurics, are at a heightened risk of CKD. 14 Given the refractory nature of cystinuria marked by frequent bouts of intermittent renal obstruction and repetitive need for procedures, it stands to reason that cystinurics are at risk for renal functional decline over time. Worcester et al. previously reported that 52 adult cystinuric patients had significantly reduced creatinine clearance (63.2 mL/min) compared with 3215 noncystinuric patients (111.1 mL/min). 15 A larger analysis of a French cystinuric cohort (n = 442) demonstrated that 26.8% of patients had impaired renal function as indicated by a GFR <60 mL/min per 1.73 m2 and 1.1% had progressed to ESRD. 16 Another contemporary study by Assimos et al. 17 reported a mean serum creatinine level of 1.13 mg/dL in 85 cystinuric patients. Not surprisingly, they found that a history of open surgical stone removal procedures and/or nephrectomy was correlated with significant decline in renal function. In their cohort, cystinurics were significantly more likely (14.1%) to undergo nephrectomy compared with calcium oxalate stone formers (2.9%). 17 Of note, in our study, although cystine stones are considered resistant to SWL, this modality appeared to be utilized as a primary treatment outside of UCSF, in line with previous published findings. 18 Judicious use of invasive surgery and more widespread adoption of minimally invasive stone extraction techniques may be helping to preserve long-term renal function in cystinuric patients. Furthermore, optimizing hydration habits, medication regimens, and medication compliance can help to decrease the frequency of surgical interventions. Poorly compliant cystinuric patients have been found to require a fourfold average increase in surgical interventions compared with medically compliant cystinuric stone formers. 19
Cystine is poorly soluble at physiological urine pH values <7.0, with stone formation occurring especially when cystine excretion exceeds 250 mg/L.
5
As a result, medical prophylaxis with hydration and urine alkalinization are usually offered as a first-line therapy unless contraindicated.
3
If these interventions fail to prevent cystine stone recurrence, the next step in the treatment algorithm is the addition of a chelating agent, such as thiol compound (tiopronin) or
Some limitations should be recognized in this analysis. The retrospective nature of the data acquisition was susceptible to incomplete and inaccurate retrieval of some data points (such as presenting symptoms and details of all procedures performed before referral to our institution) and hence the results presented must be interpreted cautiously. While a diagnosis of cystinuria was confirmed by stone analysis for all patients at our institution, history of nephrolithiasis in other family members was collected from chart review of patient-reported information, thus lacking confirmation that family members with a history of stone disease were cystinurics. Laterality of stone disease, which was the primary determinant in this study, was concluded from the review of imaging studies, radiology reports, and clinic notes. Additionally, only one-third of patients in our cohort were receiving thiol therapy or
Conclusions
Approximately two-third of cystine stone patients within our cohort form stone bilaterally during their lifetimes and require a significantly greater number of surgical stone interventions compared with unilateral stone formers. The etiology of unilateral vs bilateral stone formation in cystinuric patients remains unclear, but may relate to intrinsic renal and environmental factors.
Despite the need for significantly more lifetime surgical procedures, bilateral cystinurics were found to have median GFRs comparable to unilateral stone formers, indicating excellent intermediate-term renal preservation in both groups.
Footnotes
Acknowledgments
Funding support was provided by the NIH NIDDK K12-DK-07-006: Multidisciplinary K12 Urologic Research Career Development Program (T.C.) and NIH P20-DK100863 (T.C.).
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.