
Abstract
Introduction and Objectives:
Ureteral stent symptoms are experienced by the majority of patients with ureteral stents. No one stent or technology has shown a clear advantage. The Helical™ stent, a spirally cut stent made of proprietary Percuflex™ material, was designed to conform to the shape of the ureter and better accommodate patient movement. We prospectively sought to compare unscheduled visits, analgesic use, and pain scores in patients who received a Percuflex Helical ureteral stent following ureteroscopy compared to a historical control group.
Methods:
Fifteen (n = 15) patients undergoing ureteroscopy for the treatment of kidney stones were consented for study. A Percuflex Helical ureteral stent was inserted after treating the urinary stone. The historical control group consisted of 30 patients, from a previous (ketorolac eluting) ureteral stent study utilizing the same protocol and clinical monitoring forms, who received a regular Percuflex ureteral stent. The control patients were matched by age and sex. The primary study outcome was to compare unscheduled visits. Secondary outcomes included comparison of Visual Pain Analog Scale (VPAS) scores and analgesic use between the two groups.
Results:
There were no differences in the gender, age, BMI, or stone characteristics between groups. Both groups underwent retrograde ureteroscopy using holmium:YAG laser lithotripsy and stone fragmentation. There was a significant reduction in the amount of analgesics required in the Helical stent group (4.4 ± 7.99 mg morphine equivalents) compared to controls (16.75 ± 18.31 mg, p = 0.0035) to achieve similar VPAS scores. There was no difference in unscheduled visits (20%) or VPAS scores (13.84 ± 13.68 helical vs 14.29 ± 11.58 control, p = 0.7910) between groups.
Conclusions:
Patients who received a Percuflex Helical ureteral stent required significantly fewer analgesics than those who received a Percuflex stent and both had equivalent pain scores.
Introduction
U

Percuflex helical ureteral stent.
Methods
This study is a prospective, single-center, single-arm research study comparing patient tolerability of a novel Percuflex Helical ureteral stent to a standard Percuflex ureteral stent design (historical control from a study that occurred between December 2005 and January 2007). The study was approved by the Clinical Research Ethics Board of the University of British Columbia.
Men and women 19 years of age and older undergoing ureteroscopy for stone removal and requiring retrograde placement of a ureteral stent for an anticipated duration between 2 and 21 days were eligible for enrollment. Female patients were required to be sterile, postmenopausal, or willing to use birth control during the course of the study. Patients were excluded from the study if they had any of the following conditions: active urinary tract infection; pregnant or lactating; spinal cord injury; complications during ureteroscopy such as ureteral perforation; significant retained stone burden (with stone fragments >2 mm); history of voiding dysfunction or interstitial cystitis; nonstone related distal ureteral obstruction/stricture; solitary kidney; or chronic use of steroids, prescription anti-inflammatory drugs, nonsteroidal anti-inflammatory drugs (NSAIDS), opioids, or antispasmodic drugs. Anyone thought to require subsequent ancillary ureteroscopy was ineligible as the Helical stent is not designed to be “rewired” during a subsequent procedure, whereby the stent is pulled partially out to the urethra and then a guidewire is reinserted through the lumen of the stent to regain access into the ureter.
Patients were consented before ureteroscopy and answered a Visual Pain Analog Scale (VPAS) evaluation preoperatively immediately before surgery, and on days 1, 2, 7, and 10 poststent insertion. The VPAS questionnaire was utilized from a previous study. 3 To expedite the study, reduce costs, and remove randomization, patients were prospectively recruited and received only the Percuflex Helical ureteral stent. The control group consisted of patients from a previously completed study that utilized the same clinical protocol, clinical research forms, and VPAS scores. 3 The control group from the previous study received the Percuflex ureteral stent to compare to a stent that eluted the drug ketorolac in an attempt to reduce stent symptoms (Lexington™ stent; Boston Scientific Corporation). After this study was completed, control patients (2:1) were matched for age, sex, and ureteroscopic technique (without ureteral access sheath and without baskets) to make the comparisons comparable. Unfortunately, we were unable to access the stone details for the control group and thus we cannot compare stone characteristics. For this study, the mean stone size was 11.5 ± 1.9 mm, and a mean indwelling stent time of 7.3 ± 2.1 days, with 11 out of 15 patients having had a prior history of stone procedure. Patients in both groups had X-rays postoperatively to ensure proper stent position. Patients were given acetaminophen (325 mg) and oxycodone (5 mg) (Percocet) and instructed to take them on a p.r.n. basis postoperatively. Analgesics dosages used by patients were converted to morphine equivalents.
The primary objective was to determine if there was a difference in unscheduled patient visits. This included any unplanned visits to the clinic and emergency department or phone calls. Secondary objectives included analgesic use and VPAS scores between the groups.
Results
Fifteen patients were enrolled and consented in the study (Table 1). Thirty patients were matched to gender and age from the control group. There were no differences in age, sex, or BMI between groups. All patients underwent ureteroscopy without ureteral access sheath or use of a basket retrieval device, that is stones were fragmented into pieces and left to spontaneously pass (“dusted”). The holmium:YAG laser was used in all cases. There were no differences in unscheduled visits (20%, p = 1.000) between the two groups (Table 2). There was a significant difference, however, in analgesic use in morphine equivalents between the two groups. The Helical group required significantly less analgesics than the control group (p = 0.0035) to achieve a similar pain score on the VPAS (p = 0.7910) (Figs. 2 and 3). Comparison of the VPAS scores excluded four subjects from the Helical group because of incomplete number of questionnaires filled; however all 15 subjects were included for all the other outcomes. All stents were easily placed and removed in the Helical group. There were no complications in either group (Table 2). No patients required subsequent ureteroscopy following stent removal.
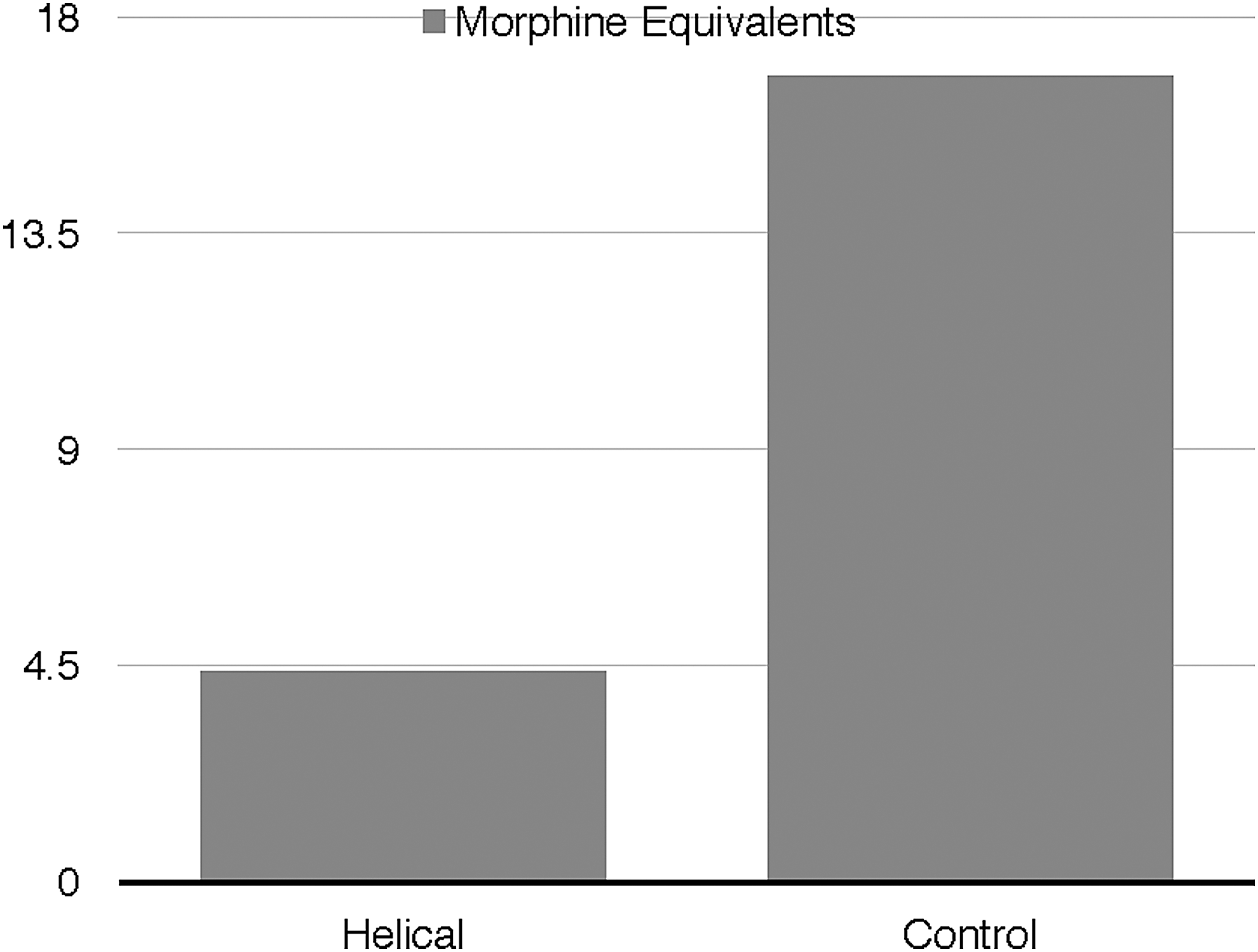
Analgesic use. Helical: 4.4 ± 7.99, Control: 16.75 ± 18.31; p = 0.0035.
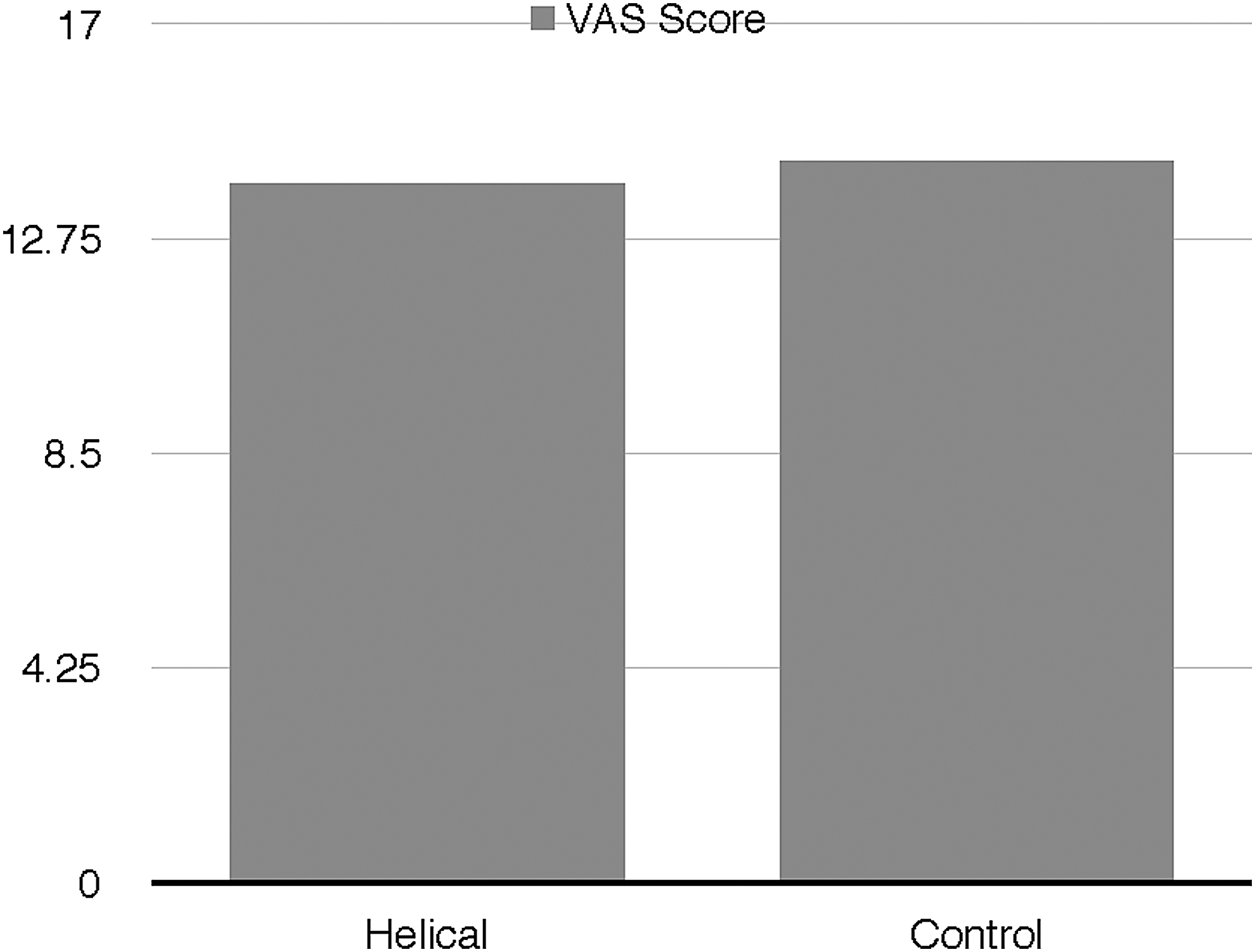
VPAS score (AUC). Helical (n = 11): 13.84 ± 13.68, Control: 14.29 ± 11.58; p = 0.7910. VPAS is calculated from the average of all scores from the day of stenting to the day of stent removal. AUC = area under the curve; VPAS = Visual Pain Analog Scale.
BMI = body mass index.
Categorical variables were tested using Chi-Square analysis and continuous variables were tested using a Kruskal–Wallis test using p < 0.05 for statistical significance.
Discussion
Despite their extensive use in urology, ureteral stents may cause several complications that negatively affect patients' daily functioning and quality of life. Stent-related discomfort is one of the most common effects of ureteral stenting experienced by patients. Greater than 80% of patients with ureteral stents have voiding symptoms such as frequency, urgency, hematuria, and dysuria, in addition to bladder, groin, genital, and flank pain. 7
The exact mechanisms of patient symptoms are not fully understood, but pain and discomfort are potentially caused by ureteral stent irritation of the urothelial lining 3,4 and are typically managed with oral pain medications such as analgesics and alpha blockers. 4 In an attempt to alleviate pain associated with this local irritation, Krambeck and colleagues investigated the effects of the nonsteroidal pain medication ketorolac that is delivered locally through a drug-eluting stent. 3 Despite observing a trend toward a potential benefit with the ketorolac-eluting stent over the regular Percuflex stent in a subset of patients (male and <45 years old), no overall significant advantage was found in the management of patient discomfort when it came to differences in analgesic use or VPAS assessment. 3
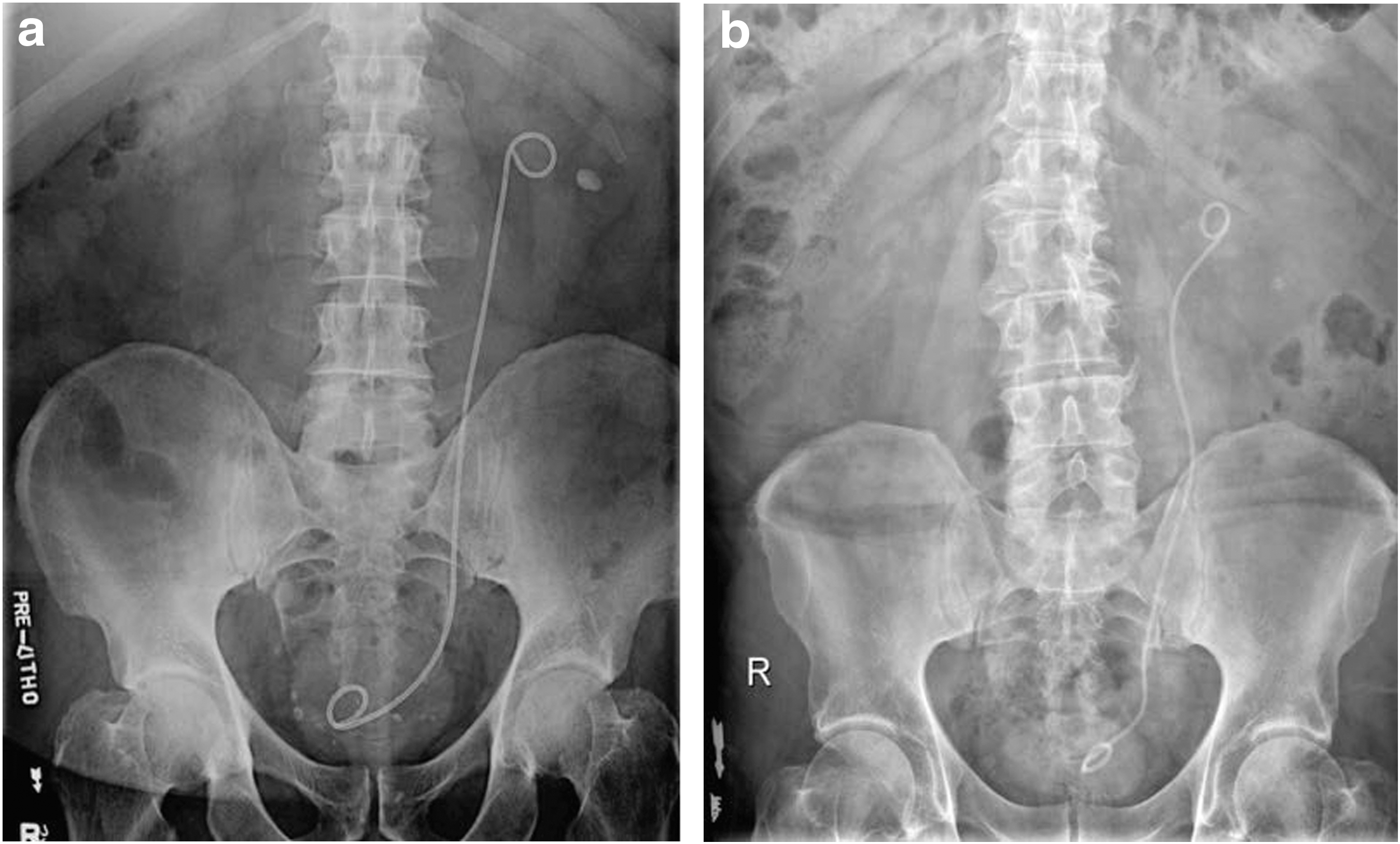
Movement of the stent within the ureter to as much as 2 cm during patient movement may also aggravate local tissue irritation and stent-related complications. 5 The Helical stent's ability to adjust to the shape of the ureter (Fig. 4) may be attributed to its increased flexibility because of its configuration, and possibly result in a decreased need for analgesics owing to the reduction in levels of pain and discomfort. In contrast, a stiffer, less flexible stent may restrict ureteral movement because of its inability to conform to the ureter as the patient moves in different positions—potentially resulting in further irritation and pain. In a porcine study, the Percuflex Helical stent seemed to conform to the shape of the ureter better than the standard Percuflex Plus stent, as seen on X-ray images. 6 The Helical stent was also shown to exhibit similar performance in terms of drainage and did not induce more histopathological changes to the ureteral epithelium. 6
Percuflex™ Plus Stent*
Our study elaborates on the results of the porcine study and gives further insights on how these Helical stent properties can translate to an improved level of patient comfort. Interestingly, increasing the flexibility of ureteral stents to allow them to conform to the shape of the ureter with patient movement has also been an area of focus for designing metal stents. 4 For example, Passage™ (Prosurg) is a metal stent with spiral winding configurations that increase its flexibility and maintain radial compression strength—features that might potentially alleviate patient discomfort. 8
In addition to local tissue irritation, another factor that has been theorized to cause morbidity is vesicoureteral reflux (VUR) during micturition, causing an increase in renal pelvic pressure. 9,10 A recent study in a swine model evaluated an antireflux stent whose “tipless” distal end is designed to prevent it from interfering with and crossing the ureterovesical junction, and thus prevents VUR and bladder irritation. 10 Results show that animals with the antireflux stent did not have VUR; there was significantly less histopathological damage at the UVJ level in the antireflux stent group, 10 suggesting that patient tolerance may be improved with the antireflux stent compared to standard Double-J stents. However, more research is necessary to fully elucidate the effects of an antireflux stent on patients' stent-related symptoms, as this study was performed using an animal model and symptoms cannot be extrapolated. Currently there is no evidence to support that a helically cut stent reduces VUR, and this was not assessed in this study.
Research has focused on the development of ureteral stent material that can address complications associated with indwelling ureteral stents. Novel materials, such as biodegradable stents and drug-eluting stents have been investigated for their effects on decreasing bacterial infection and adhesion, and on overall patient comfort. 4 The spirally cut Percuflex Helical stent used in this study is made from the same proprietary material as the Percuflex Plus stent used in the control group. With a change in configuration, the Percuflex Helical stent group achieved a statistically significantly lower analgesic requirement, although without any change in the VPAS score. Continuous progress and advances are ongoing in modifying stent material, and this study shows that even small changes in ureteral design can greatly affect patient symptoms.
In another study, two proprietary materials, Percuflex (Boston Scientific Corporation) and Polaris™ (Boston Scientific Corporation), were compared with respect to stent symptoms, utilizing the Ureteral Stent Symptom Questionnaire (USSQ). 11 Patients with the soft-tailed Polaris stent had fewer symptoms than patients with the regular Percuflex ureteral stent. Although no significant differences were found in terms of VPAS scores, analysis of the USSQ scores showed that the Polaris test group had better outcomes for “presence of pain” and “frequency of pain killer use,” among others. 11 This is comparable to our results where the Helical stent group required significantly less analgesics than the control group, despite scoring similarly on the VPAS. Furthermore, similarly, the Polaris group scored better with respect to the parameters of fatigue, stent-related impact on work, and difficulties with respect to hard physical activity. Intuitively, pain levels and thus pain scores should be lower after receiving pain medication, and conversely, higher scores may pose a need for additional pain medication.
In a study analyzing the clinical significance of VPAS in postoperative patients, a higher proportion of patients requesting an increase in their analgesic dose corresponded to a higher prior VPAS score, 12 suggesting that increased analgesic use can potentially lower a patient's score on the VPAS. Similarly, decreasing VPAS scores were observed after analgesic administration in cancer patients with either chronic pain or postoperative pain. 13 Requiring significantly less analgesics to achieve a similar VPAS score in the Helical stent group may be indicative of improvement in patient comfort with the Helical stent compared to the regular one. Despite the significance of the decreased analgesic use in the more flexible Helical stent, however, we can only postulate that more flexible ureteral stents improve patient comfort, as bigger clinical trials are required to answer this question. However, it should be noted that the Helical stent is not currently commercially available, and the authors are unaware of any future plans to make the stent available again.
Limitations
Limitations of this study include the small sample size, nonrandomized approach, historical control group from a previous study, and a potential source of bias from the absence of blinding of the authors to the use of the helical stent. Also, we did not evaluate the use of over-the-counter pain medications in either study. Patients were not given any specific instruction regarding other medications except to keep track of how many prescribed analgesics they have taken. Anesthesia records for intraoperative use of narcotics and NSAIDs were also not reviewed for this study. However, this study followed the exact protocol and clinical research data collection forms of the previous study, so that the control group could be adequately compared.
Because the stent is not designed to be rewired, the stent is not recommended for prestenting individuals for dilation. However, should a patient require ureteroscopy even with a Helical stent in place, the stent could simply be removed and a guidewire placed into the ureter as if beginning a de novo ureteroscopy. That is to say, stenting with a Helical stent does not preclude subsequent ancillary ureteroscopy. Ureteral dilation using this stent appears to be similar to that found with normal, polymeric solid stents.
Insertion and removal of the Helical ureteral stents were successful in 100% of cases studied. All stents were inserted over a 0.038″ polytetrafluoroethylene (PTFE)-coated nitinol core Sensor Wire (Boston Scientific Corporation). Removal with either string tethers or cystoscopy was uneventful. No stone fragments were noted within the coils of the stent upon removal or impinged stent removal.
Conclusions
Although no significant differences were observed in the primary outcome (unscheduled visits) and in one of the secondary outcomes (VPAS score), this study demonstrates that patients with the Percuflex Helical stent required significantly less pain medications than those with the standard Percuflex Plus stent. Further investigations through larger clinical trials are necessary to confirm the benefits of a highly flexible ureteral stent with a helical configuration.
Footnotes
Acknowledgments
The authors thank Ms. Wen Ding and Mr. John Evans for their statistical analytic work, without whom this project would not have been possible, and Tim Harrah and Boston Scientific Corporation for providing the Percuflex Helical Stents and for sharing the data for the control group from the previous Lexington Stent study. The stents used in this study were given in kind. No other funding support was received from Boston Scientific Corporation.
Author Disclosure Statement
No competing financial interests exist.