
Abstract
Background:
The standard treatment of T1 renal cell carcinoma (RCC) is (partial) nephrectomy. For patients where surgery is not the treatment of choice, for example in the elderly, in case of severe comorbidity, inoperability, or refusal of surgery, alternative treatment options are available. These treatment options include active surveillance (AS), radiofrequency ablation (RFA), cryoablation (CA), microwave ablation (MWA), or stereotactic body radiotherapy (SBRT). In the present overview, the efficacy, safety, and outcome of these different options are summarized, particularly focusing on recent developments.
Materials and Methods:
Databases of MEDLINE (through PubMed), EMBASE, and the Cochrane Library were systematically searched according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria. The search was performed in December 2016, and included a search period from 2010 to 2016. The terms and synonyms used were renal cell carcinoma, active surveillance, radiofrequency ablation, microwave ablation, cryoablation and stereotactic body radiotherapy.
Results:
The database search identified 2806 records, in total 73 articles were included to assess the rationale and clinical evidence of alternative treatment modalities for small renal masses. The methodological quality of the included articles varied between level 2b and level 4.
Conclusion:
Alternative treatment modalities, such as AS, RFA, CA, MWA, and SBRT, are treatment options especially for those patients who are unfit to undergo an invasive treatment. There are no randomized controlled trials available comparing surgery and less invasive modalities, leading to a low quality on the reported articles. A case-controlled registry might be an alternative to compare outcomes of noninvasive treatment modalities in the future.
Introduction
K
The current standard treatment of T1 tumors is (partial) nephrectomy. 1 Alternative treatments are active surveillance (AS), radiofrequency ablation (RFA), cryoablation (CA), microwave ablation (MWA), and stereotactic body radiation therapy (SBRT) (for inoperable patients). In this systematic review, we will give an overview of the alternative treatment modalities for SRM. The aim is to summarize efficacy, safety, and outcome for each alternative therapeutic method available, focusing on nephron-sparing treatment for T1 RCC.
This review can be considered an update on the review of Cutress and colleagues, 5 without the surgical options. The added value of this review is that the focus is solely on alternative treatment options, including SBRT, the most recent development in the treatment of RCC.
Materials and Methods
The protocol for this systematic review was registered on PROSPERO (CRD42016052946) and can be assessed at
Search strategy
A systematic search was performed in the databases MEDLINE, EMBASE, and the Cochrane Library, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) criteria. 6 The last update was on December 1st, 2016. Details of this search strategy are provided in Table 1.
Comparable search strategies have been conducted for EMBASE and the Cochrane Library.
Study inclusion
Articles reporting on alternative treatment options for RCC (AS, RFA, CA, MWA, SBRT) were eligible for inclusion. Articles were excluded if the title/abstract did not report primary treatment with AS, RFA, MWA, CA, or SBRT in patients with primary RCC/SRM, or if it was not an original article (i.e., review, abstract, commentary, case report, animal studies), or not written in English or Dutch. The resulting titles and abstracts were reviewed by the researchers. The search covered a period from 2010 to December 2016.
Selection of studies and data extraction
After removal of duplicates, all articles were screened on title and abstract. Full-text articles assessed for eligibility were all reviewed by one investigator (F.M.P.) and, to retrieve a second independent review opinion, divided among all researchers. Disagreement among team members was resolved by discussion and consensus. A predefined data-extraction form was used to obtain all relevant information, including a level of evidence according to the Oxford Center for Evidence-based Medicine Levels of Evidence 2009 (
Results
The database search identified 2806 records. After removal of duplicates, 2534 articles were screened on title/abstract. A flowchart of this search is reported in Figure 1. In total 73 articles were included in this review, divided among the different treatment modalities.
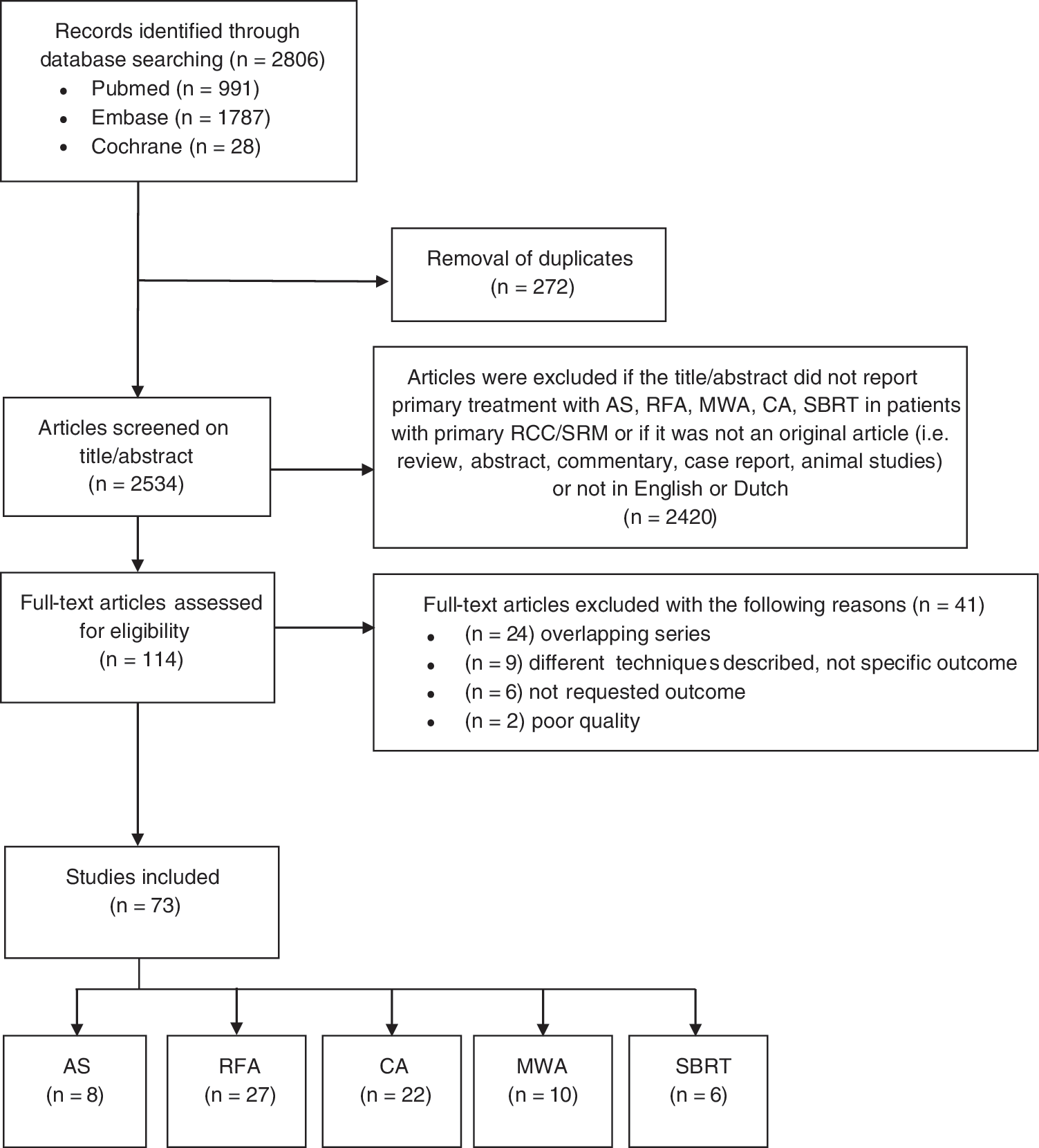
PRISMA flow chart of the systematic review. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Active surveillance
AS involves monitoring tumor size by different imaging techniques over a period of time. In case progression occurs, delayed intervention will be performed. 1 The goal of AS is to prevent unnecessary treatment-related morbidity and monitor the tumor progression in such manner that timely intervention with curative intent is assured.
As is shown in Table 2, the level of evidence in all studies is 2b, and the studies are all retrospective or prospective cohort studies. AS is mainly used for SRM, that is, renal masses ≤4 cm. The mean and median tumor diameters in these studies varied between 1.8 and 2.8 cm with a mean tumor growth between 0.11 and 0.7 cm/year. Although the range of tumor growth is not wide, evidence concerning the relationship between tumor size and tumor growth was inconclusive. One study did not report any association between tumor size and growth rate. 4 Three studies reported an association with an increased growth rate for larger tumors. 7 –9 Mason and colleagues reported that larger tumors (≥2.45 cm) grow faster than smaller lesions. 7 However, all studies concluded that a faster growth rate was related to worse outcome, and a higher risk of developing metastatic disease.
Biopsy-proven RCC: percentage of RCC proven of total NP.
CSS = cancer-specific survival; NP = number of patients; NR = not reported; NT = number of tumors.
Based on the growth rate, delayed intervention can be necessary in patients on AS. 8,9 Delayed intervention varied between 5% and 26%. Indeed, fast growth rate was the major indication to start invasive treatment, most often surgery. 4,7,9 –13 Even so, two studies showed delayed intervention with RFA or CA as well. 10,13 The goal of delayed intervention is to assure local control and prevent metastatic disease, which occurred in 0%–3.2% of the AS population. 4,7 –13 Patel and colleagues did not observe any metastatic progression in tumors showing negative or zero tumor growth during follow-up (FU). 8 Moreover, they proposed to intervene if SRMs are >3.5 cm in size or show mean tumor growth of >0.5 cm/year. 8
Interestingly, only a small proportion of patients in FU for AS underwent a biopsy either at the start or during FU. As such, the percentage of biopsy-proven RCC in these studies of the total number of patients varied from 8.5% to 50%. Therefore, the results presented are possibly not an accurate reflection of the actual study population, that is, patients with RCC-proven SRM (Table 2: biopsy-proven RCC). In groups with delayed intervention, more often a biopsy was performed shown to be positive for RCC; patients with benign or unknown pathology were more likely to be scheduled for AS. 10 –12
Several outcome measures have been used in the aforementioned studies. Cancer-specific survival (CSS) varied from 97% to 100% in a median FU period between 25 and 92 months (range 6–208). Nevertheless, in most studies, AS was mainly considered for the elderly, patients with comorbidities preventing an invasive treatment approach, or patients refusing surgery. 4,7 –13
In conclusion, a small proportion of patients will need to undergo delayed intervention during AS. AS is considered a safe treatment option for patients with SRMs. However, as there is no curative treatment for metastatic disease, developing metastatic disease during surveillance remains a rare but nonetheless potential risk.
Radiofrequency ablation
The first study describing the treatment of RCC by RFA was published in 1997 by Zlotta and colleagues. 14 Radiofrequency energy can be used to create heat causing necrosis of tumor cells. The local effects are obtained by implanting single or clustered needles in the tumor tissue through which the radiofrequency energy is applied. Operating temperatures range from 50°C to 100°C. Placement of these needles can be achieved both laparoscopically or through a percutaneous approach. 1 Percutaneous treatment is most frequently used, usually ultrasound (US) or CT guided, under general anesthesia or intravenous (IV) sedation. 15,16
Table 3 summarizes the studies reviewed on RFA. The level of evidence in all studies varied between 2b and 4. The described techniques of RFA were either percutaneous or laparoscopic, both US or CT guided. Most tumors treated by RFA were classified as T1a or T1b tumors. RCC was 100% proven in 13 studies, and in the other 15 studies RCC was partly biopsy-proven benign or suspected for RCC on CT or MRI.
Biopsy-proven RCC: percentage of RCC proven of total NP.
CSS = cancer specific survival; NP = number of patients; NR = not reported; NT = number of tumors; RFS = recurrence free survival.
Tumor diameter is an important predictor for success in RFA treatment. In the reviewed studies, tumor diameter ranged between 2.1 and 5.1 cm (range 0.5–7.6). Zagoria and colleagues concluded that for RCCs less than 4 cm long-term tumor control can be achieved since no recurrences were reported for lesions <4 cm. 17 Iannuccilli and colleagues reported an increased risk of residual tumor for lesions ≥3.5 cm. 18 In US-guided percutaneous RFA of tumors ≥4 cm, 40% showed incomplete ablation, whereas in CT-guided percutaneous RFA, there was an incomplete ablation of 16.7%. 19 Each centimeter increase in tumor diameters greater than 3.6 cm appeared to be associated with a decreased disease-free survival (DFS) by a factor of 2.19. 17 In accordance with other studies, it was concluded that for RCC >4 cm other treatment options should be considered. 17 Or, as McClure and colleagues stated, smaller lesions may require a single ablation (median size 2.1 cm), but larger lesions (3.6 cm) need more than one ablation. 20
Another independent predictor of successful RFA is the location of the tumor. An exophytic localization is considered beneficial, with a decrease in risk of residual disease. 20 –23 Larger diameter and central localizations were associated with an increased risk of major complications, 16 and a risk of incomplete ablation. 20,24 Therefore, a laparoscopic RFA approach has been proposed as the treatment of preference when the renal tumor is in the proximity of critical structures. 25 Beside tumor location, clear cell subtype and maximum treatment temperature ≤70°C were factors related to an increased risk of residual lesions. 23
Several complications have been reported after RFA treatment. Complication rates varied between 5.1% and 37% in different studies. Most of these complications were minor, that is, Clavien-Dindo grade I–II. Minor complications included perirenal hematoma, 16,18 –21,26 –31 postoperative fever, 19,27,32,33 gross hematuria, 19,26,29,34 asymptomatic pneumothoraxes, 16,17,21,28,34 paresthesias, 16,18,19,21,27,33 thermal injury in skin, psoas muscle, and liver, 16,21,26,33 and arterial hypertension. 16,18 Major complications (Clavien-Dindo grade III–IV) included fistula in the abdominal tract (with or without urinoma and infection), 16,21,25,28 bowel injury (which required diverting ileostoma) or duodenal perforation, 16,26,35 abscess, 16,21,24,29 acute kidney failure and dialysis, 16,20,21,33 urethral stenosis, stricture, obstruction, or urine leak. 16,18,20,21,24,25,27,30,33
A few studies also reported on kidney function pre- and postprocedural. Most find no significant decrease in estimated glomerular filtration rate (eGFR), 19,28,36,37 or an increase in creatinine. 35,38 Three studies reported a better preservation of renal function after a RFA procedure, compared with a partial nephrectomy. 22,29,39 Impaired baseline kidney function tended to deteriorate after RFA. 22
Median FU varied between 15 and 79 months (range 1–131 months); only four studies reported results after a median FU time >60 months. 15,23,37,40 In most studies recurrence was defined as contrast enhancement of >10 HU, 17,25,27 >15 HU, 15,16 >20 HU, 26,41 based on a CT scan, a >15% increase of the signal on MRI, 17,21,21,26 or presence of viable tumor cells. 26 FU was set at 1, 3, 6 months, and biannually thereafter for all studies.
Tumor recurrence was usually seen within the first 2 years after treatment. 18,23 Recurrence-free survival (RFS) between 67.6% and 100% was reported at a median FU between 15 and 79 months (range 1–131 months). A higher tumor stage correlated with a decreased RFS and DFS in patients treated with RFA. 15,17 Stage T1a tumor was a positive predictor for overall and CSS. 24 In addition to tumor size, the technical success and RFS are dependent on the experience of the operator, and more experienced physicians can achieve RFS rates up to 100%. 21 In case incomplete ablation or recurrence occurred, patients were considered candidates for a second RFA treatment. 20,24
Median survival and overall survival rates were higher for tumors ≤3 cm than for tumors >3 cm. 16,23 Tumor size diameter over 4 cm was also mentioned as being the only risk factor associated with residual tumor or recurrence of the tumor. 16,19 Indeed, in T1b tumors, a significantly higher risk of residual disease was reported compared with T1a lesions. 15 In Veltri and colleagues T1a is mentioned as a positive predictor for complete ablation. 24 Balageas and colleagues reported a relative risk of recurrence or residual disease for each centimeter increase of 9.35. 16
In conclusion, RFA is considered to be an effective treatment option in small renal tumors <4 cm with a beneficial localization and is mostly used in poor surgical candidates, 17,25,29,31,35,36 although a few studies do report the possibility in healthy patients with T1a tumors. 22,27,37,40 In the last few years, studies with longer FU are presented and, therefore, RFA can also be considered as an alternative treatment for durable local control. 15
Cryoablation
In 1995, Uchida and colleagues were the first to report on percutaneous renal CA. 42 Both laparoscopic cryoablation (LCA) and percutaneous cryoablation (PCA) are used in clinical practice. Patients with a localized SRM (≤4 cm) are selected for treatment by CA based on operator preference, presence of multiple masses, previous renal surgery, and medical comorbidity. 43 –46 PCA is most often used in clinical practice and is preferred in posterior and lateral tumors, with a clear window for probe placement. 47 Aron and colleagues suggested to use the PCA for posterior and posteromedial tumors; for anterior and lateral tumors they prefer LCA, although it is a more invasive approach. 48 LCA is preferred if bowel or solid organs are close to the tumor. 49 The exact mechanism of cryotherapy is not entirely known, but it relies on the assumption that temperatures <−20°C induce cell death. 45,49 A nitrogen-based liquid is guided through the tip of the cryoprobe to create an ice ball extending 1 cm beyond the margins of the tumor. There is a rapid freeze at the tip with working temperatures between −185 and −195°C.
In Table 4 the reviewed studies on CA are summarized. The level of evidence in all studies is 2b. The mean tumor diameter varied between 2.1 and 4.8 cm. Although most tumor sizes were rather small, treatment failure was significantly associated in tumor size >4 cm as was reported by Kim and colleagues. 56 Even so, two studies reported no association between tumor size and complication rate. 50,51 In all studies the majority of tumors within the study group were pathologically proven RCC, varying between 49% and 100%.
Biopsy-proven RCC: percentage of RCC proven of total NP.
The cause of treatment failures mentioned in the different studies were diverse. One technical failure occurred during treatment of a 4.3 cm large centrally situated RCC. 52,53 A broad-based contact with the renal sinus led to a clinical treatment failure in seven out of eight patients. 53 Ice ball formation under 6 mm around the tumor was related to incomplete local control. 45,54 An increased skin-to-tumor distance was also mentioned as a risk factor of treatment failure. 50 Location of the tumor also plays an important role in treatment success, where central location of the tumor was associated with an increased risk in treatment failure. 52 –54
Renal clamping in surgical treatment is necessary, but causes a period of ischemia and, therefore, it influences renal function postoperatively. Ischemia is not used in ablative procedures, which is a potential benefit of ablative therapies. 49,55 Most studies reported on kidney function after treatment. The results were heterogeneous. Most studies showed no difference in serum creatinine levels and eGFR, pre- and postablation, 43,45 –48,51,55 –59 whereas others showed a minimal impact. 44,48,57 It is even stated that CA has superior outcomes compared with surgery with regard to preserving renal function, especially in single kidneys. 45,49 Interestingly, Tanagho and colleagues stated that a smaller tumor size and hilar location contribute to improved renal function outcomes after CA. 44
The complication rates in the different studies varied from 0% to 23%. The occurrence of major complications appeared to be associated with tumor size. 50,52,60 Atwell and colleagues reported a significant higher complication rate in higher T-stages, in which they advise that CA for >T1b is technically feasible, although complications are more frequent. 60 Bleeding was also significantly increased in T1b tumors. 59 Breen and colleagues reported that upper pole location was a predictive factor for complications. 52
Most reported minor complications (Clavien grade I–II) were perirenal hematoma, 44,45,50,52,57,59,61 pneumothorax, 48,50,52,55,62 pneumonia, 48,55,62 hematuria, 54,59 and persistent flank pain. 45,52,60,62
Most reported major complications (Clavien grade III–IV) were cardiopulmonary decompensation and myocardial infarct, 44,47,48,60,62 ureteropelvic junction obstruction/injury, 47,52,55,60,63 postprocedural bleeding, 47,48,52,57,60,64 and blood transfusion. 52,59,62,63 One of the causes of bleeding during CA treatment was ice ball fracture, especially in treatment with a larger tumor diameter. 52
The RFS varied between 81% and 99%, with a median FU period between 12.7 and 97.9 months. RFS was defined as no evidence of radiographic recurrence or increasing tumor size >6 months after the procedure, 43,50 although the definition of recurrence in the reviewed studies is not always clear. Four studies reported a FU of 10 years, 48,57,63,64 in which Johnson and colleagues described an average time to recurrence of 39.9 months, Larcher and colleagues reported a median time to recurrence of 18 months, and Caputo and colleagues reported a time to recurrence of 27.6 months, with the latest recurrence after 53.3 months. The CSS varied between 92% and 100%, although it was not reported in nine studies. Even so, several short FU studies show adequate oncological control and limited morbidity indicating that the use of CA in renal tumors is acceptable. However, more recent results on ablative treatment of T1 lesions in long-term studies suggested that CA is possibly associated with poorer outcomes, such as reduced overall, cancer-specific and DFS. 48,60,62 However, CA may be safely used in patient groups not suitable for surgical treatment. 45,46,57
In conclusion, CA is considered a safe and effective treatment for patients with SRM who are poor surgical candidates due to significant comorbidities. 51,52,60,65 The RFS and CSS are favorable on the short term. Whether results in the long term are acceptable is up for debate, since several studies suggest a poorer outcome, 48,60,62 whereas other studies do show a beneficial outcome in a longer FU period. 48,57,63,64
Microwave ablation
MWA is a thermal ablation technique, which uses electromagnetic microwaves through one or multiple antennas placed in the tumor. Tumor cells are damaged by the mechanism of creating a thermal field by rotation of dipole water molecules, producing heat and causing tissue necrosis in solid tumors. 66 The electrodes function as an antenna to concentrate the energy and are placed by a percutaneous 67 –74 laparoscopic 67,75,76 or open approach 76 under general anesthesia. The number of antennas used depends on size and location of the tumor. The penetration depth of the energy can be adjusted by the frequency of the energy source. The different energies used vary between 1 and 100 W, with a frequency of 915 or 2450 MHz, depending on the system used.
Table 5 shows the reviewed studies on MWA. The level of evidence varied between 2b and 4. A few studies mention a potential benefit over RFA. A potential benefit can be that MWA is less effected by the heat sink effect, as a result of less dependence on the electrical conductivity of tissue, and higher thermal efficiency, thereby reaching higher intratumoral temperatures and thereby less ablation time. 69,70,72,73,76 As such, possibly larger tumors can be ablated. 69,70,76
Biopsy-proven RCC: percentage of RCC proven of total NP.
The mean diameter varied between 2.4 and 3.7 cm (range 0.6–8.4 cm). The size of the tumor is important. Gao and colleagues reported a significantly better ablation success in tumors <4 cm (100% success), compared with >4 cm (75% success). 72 Guan and colleagues stated that only exophytic low-grade tumors with a diameter <4 cm should be considered for treatment with MWA. 76 A maximum diameter of 4 cm was recommended in most studies. 68 –70 However, several authors suggested that MWA can also be performed in tumors near the renal sinus, 72 or in the collecting system 67 ; a clear benefit over other ablative techniques.
As opposed to surgical techniques, renal clamping is not necessary in MWA procedures. 75 A few studies in MWA reported on postprocedural renal functions. In some studies, the eGFR and postprocedural creatinine levels 70 –72,74 did not significantly decrease. 69 In other studies a small decline in kidney function had been seen. 73,76 In patients with pre-existent chronic kidney disease, function remained stable. 72,76
The complication rate varied between 0% and 60%. Most complications were low-grade complications (Clavien grade I–II): hematuria, 67,72,73,76 numbness, 67,76 flank pain, 67,76 thermal injury, 67,73 urine fistula, 70 –72 and subcapsular renal hemorrhage. 69,74
High-grade complications (Clavien grade III–IV) were also reported: urinoma, 67 retrained foreign body, 67 urine leakage and abscess formation requiring drainage, 72,76 hydrothorax in two patients, 73 pleural effusion, 74 and bowel injury. 73 Two studies did not mention any complications. 68,75
The RFS varied between 62% and 100% in a median FU between 8 and 32 months (range 1–93.2 months). Castle and colleagues reported the highest recurrence (38%, median FU of 18 months). 67 Wells and colleagues reported a RFS of 100%, but recurrence to metastatic disease in one patient. 71 Gao and colleagues reported a median time to recurrence of 34.1 months. 72 In a few studies a second ablation session was necessary, due to residual tumor. 68,70,71,74,76 The RFS ratios were reflected in favorable CSS ratios (92%–100%).
In all studies, RCC was biopsy proven in the largest part of the cohort. In Dong and colleagues, a part of the study group was not pathologically proven due to the inability to take biopsies due to comorbidities. 73 In Guan and colleagues, 14 out of 38 treated tumors were benign. 76 This raises the question whether not all SRMs should be biopsied in advance of ablative treatment, as was the case in most other studies. 68 –72,74,75
In conclusion, MWA appears to be a safe and effective treatment option especially for tumors ≤4 cm, in elderly with associated comorbid diseases, and in poor surgical candidates. 70,71 It is also a suitable treatment option in tumors near the renal sinus or in the collecting system 67,72 ; a clear benefit over other ablative modalities. Although these results are promising, the groups were relatively small and only short-time FU is available. MWA has a few theoretical advantages over other ablative techniques, but oncological control has to be proven during the long-term FU. More and larger studies are required to more safely implement this technique.
Stereotactic body radiation therapy
The use of external beam radiotherapy (EBRT) has been limited before the last decade due to assumed radioresistance of RCC dating back to the time that conventional (too) low-dose fractionated radiotherapy for RCC was the standard of care. Developments in SBRT within the last decade have allowed for precise delivery of high-dose hypofractionated radiotherapy. Recent studies have shown that RCC is actually radiosensitive. 77
Stereotactic body radiation therapy is a high precision radiation technique that enables delivery of a high radiation dose in one or a few fractions, making use of online image guidance. An additional advantage relative to conventional EBRT is a steep dose fall off from the planned target volume to surrounding tissues and a high biological dose can be delivered with small margins surrounding the tumor volume and, therefore, low associated toxicity rates. During the last few years, there has been an improvement in imaging and, therefore, the margins are smaller and the dosage can be delivered even more precisely. 78 Another advantage is that this treatment is either noninvasive (without fiducial markers), 77,79 or minimally invasive (when fiducial markers are placed in the tumor or in the near parenchymal tissue). 78,80 –82
An overview of the current literature about SBRT for inoperable RCC is described in Table 6. The level of evidence in these studies is 2b. SBRT treatment for RCC is currently used in inoperable patients. All of the described studies used a high-dose per fraction external radiation, gross tumor volume outline for treatment planning on CT scan, and the use of CT for position verification. In some studies, the position verification before each treatment fraction was improved by the use of fiducial markers in the tumor/surrounding kidney tissue, 78,80 –82 or the patient is fixed in a body frame with vacuum stabilization. 77,79 When using fiducial markers and, therefore, more precise targeting of radiotherapy, in one study a significant lower ratio of renal atrophy was reported. 80 Although the radiotherapy techniques used in the different studies are comparable, the prescribed doses and fractionation schemes used were heterogeneous, sometimes even within studies as the fractionation scheme may be adapted to tumor size, 77,79 or due to dose escalation. 78,82
Biopsy-proven RCC: percentage of RCC proven of total NP.
The tumors treated in the different studies vary in diameter (mean 3–4 cm; range 1.0–14.6); two studies did not report a diameter of the treated tumors, although one stated that lesions had to be less than 4 cm due to technical limitations of the cyberknife. 81 Successful treatment seems to be related to tumor size. Pham and colleagues use the size of the tumor to determine the dosage given to the tumor, 42 Gy in three fractions in tumors ≥5 cm, and 26 Gy in one fraction in tumors <5 cm. 77 The more recent studies have shown the possibility to treat larger lesions. They stated that in SBRT treatment there are no limitations considering tumor size and location of the tumor. 78,79
The fractionation schemes in literature varied between 25 and 48 Gy, in 1 to 5 fractions. The RFS with these dosages was reported between 63% and 98%. The largest study so far, including 40 patients with 45 tumors, 98% RFS was achieved after a mean FU of 28.1 months. This study did not include metastatic RCC. 81 Overall, the FU was relatively short, with a median FU varying between 6 and 31.2 months. The CSS is not reported in any of the studies.
The reported grade 1–2 toxicities varied between 30% and 60%, but were relatively mild. Most reported toxicities were nausea, 77,79,81 fatigue, 77,81,82 dermatitis, 77,81 and local pain. 77 In one patient, a duodenal ulcer (grade 4 toxicity) occurred. 82 Ponsky and colleagues also reported renal toxicity in 2 out of 19 patients with pre-existing renal dysfunction, 82 Chang and colleagues reported on grade 4 renal toxicities in 2 out of 16 patients, 79 while two other studies described a stable kidney function pre- and posttreatment. 80,81
In conclusion, radiotherapy is considered to be a safe and effective treatment. Indications for the use of SBRT are patients not suitable for surgery due to comorbidity, so there is a need for noninvasive treatment alternatives. 78,80,81 Although early results seem promising, most studies have used a small number of primary RCC, partially not pathologically proven and with a relatively short FU.
Conclusion
There are several alternative treatment options for patients with RCC other than (partial) nephrectomy, especially for those patients who are unfit to undergo an invasive treatment. Most of these treatment modalities are minimally invasive (CA, RFA, MWA, and SBRT with fiducial markers); radiotherapy can be completely noninvasive, when a technique without fiducial markers is used.
AS is by definition noninvasive during the “surveillance” period. However, this modality also implies “active” treatment in case of disease progression, with a limited risk of metastatic disease. It should be noted that in described series only a small fraction of patients underwent a biopsy. So whether these series indeed reflect studies concerning patients with RCC is debatable.
All alternative treatment modalities have been described as being safe and effective, based on phase I and II studies. Phase II studies with mean FU time longer than 5 years have been published for AS, RFA, CA, MWA, and SBRT, although the number of patients treated in MWA and SBRT studies were small. For RFA, CA, and MWA, limitations in the size (and sometimes location) of the tumor exist, as larger sizes or more central locations may interfere with local control rates and treatment-related morbidity. Despite the theoretical advantages of MWA on RFA and CA, more and larger studies are required to more safely execute this treatment. For SBRT there are, in general, no limitations to tumor size and location, and the expected toxicity of SBRT is mostly related to the proximity of the surrounding healthy organs.
Radiotherapy treatment has improved dramatically throughout the last decade, moving from low radiation doses with large treatment fields, to more precise CT-guided radiotherapy, allowing for a higher biological effective dose, a smaller number of treatment fractions at stereotactic accuracy (therefore limiting the volume of healthy tissue treated and minimizing toxicity). Improvements are expected within the next years, when noninvasive (without fiducial markers) MRI-guided radiotherapy will become available, allowing for even more accurate radiation and dose escalation.
Randomized controlled trials (RCTs) comparing (partial) nephrectomy to less-invasive treatment modalities have not been performed to date. However, an RCT comparing surgery and less invasive modalities may not be feasible any more due to patient preferences leading to inability to randomize patients into treatment arms. Nevertheless, case-controlled registries may be alternatives to compare outcomes of minimal to noninvasive treatment modalities to surgery in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.