
Abstract
Background and Purpose:
Transurethral seminal vesiculoscopy (TSV) provides an efficient approach to diagnose and treat hematospermia, but still needs further improvement in manipulation and corresponding instruments. In this study, we develop an innovative technique with ultrasonic lithotripter (EMS) to treat severe, persistent hematospermia.
Patients and Methods:
Data of patients who underwent TSV with or without ultrasonic lithotripter between May 2012 and December 2015 was reviewed. For the innovative procedure, a 3.3F ultrasonic lithotripter was introduced through the working channel of an 8F seminal vesiculoscope to remove calculi, blood clots, or purulent material, whereas in routine procedure, the holmium laser lithotripsy was performed with lower energy (maximum power 10 W). Complication, hematospermia recurrence, the operative time, and postoperative hospitalization were recorded.
Results:
A total of 30 patients, 16 in Group A (routine TSV) and 14 in Group B (TSV with ultrasonic lithotripter procedure), were involved in this study. The median follow-up time for patients in Group A and B was 28 and 31 months, respectively. The mean operative time in Group A and B was 66 and 50 minutes, respectively (p < 0.05). All the TSV procedures in Group B were successful, except one patient had a two-stage procedure because of right seminal vesicle stones accompanying with pus. One patient in Group A had the discontinuation of the procedure because of accidental bleeding during stone fragmentation. During the follow-up, two patients in Group A had recurrent hematospermia and underwent the second TSV, whereas no recurrence happened in Group B. No epididymitis, retrograde ejaculation, rectal injury, incontinence, bladder neck contracture, or erectile dysfunction happened in both groups.
Conclusion:
TSV with ultrasonic lithotripter enables a more reliable, effective, and convenient procedure to diagnose and treat severe, persistent hematospermia. It controls the recurrent hematospermia with less operative time and complication.
Introduction
H
Ex vivo endoscopy of the SV was first reported by Shimada and Yoshida, whereas the following in vivo operation was finished by Okubo and colleagues. 6,7 Lots of studies have shown that transurethral seminal vesiculoscopy (TSV) is feasible in the diagnosis and treatment of hematospermia 8 –10 ; however, there is still the absence of endoscopic instruments to effectively remove stone fragments, blood clots, and pus residues. In this study, we will present the innovative technique of TSV with ultrasonic lithotripter for diagnosis and treatment of severe, persistent hematospermia and validate the efficacy and safety of the procedure in clinical practice.
Patients and Methods
Patients
Patients with severe, persistent hematospermia undergoing TSV between May 2012 and December 2015 were retrospectively reviewed. The patients who underwent routine TSV were in group A, whereas those who underwent TSV with ultrasonic lithotripter were in group B. The indication of TSV procedure was multiple episodes of hematospermia (occurred more than six times or lasted over 6 months) and meantime, the failure of a 4-week levofloxacin treatment. No patient who has not yet fathered was enrolled. This study was approved by the Ethics Committee of Changhai Hospital and the management algorithm of hematospermia is shown in Figure 1. All the patients were evaluated by routine hematology examination, clinical biochemistry test, urinalysis, and urine/prostatic solution microorganism culture. Imaging examinations were performed to further exclude malignant diseases. Serum prostate-specific antigen was tested if the age of the patient was more than 40 years, because prostate cancer, an important cause of hematospermia, cannot be directly diagnosed by TSV. In addition, the companying symptoms were recorded. For the patient with a positive microorganism culture, the culture-specific antimicrobial therapy was administrated and the negative culture outcome was confirmed before surgery. All the operations were performed by two senior urologic surgeons.

The algorithm of hematospermia approach and management.
Surgical technique
Group A: routine TSV
Under general anesthesia, patients were positioned in the standard lithotomy position. After observing urethra and bladder, an 8F rigid ureteroscope (Storz, German) used as the seminal vesiculoscopy was inserted retrograde, under the guidance of a 0.032-inch Zebra guidewire (Urovision, German), through the utricular orifice at the verumontanum. After entering the lumen, the Zebra guidewire was further introduced through the ejaculatory duct orifice to guide the ureteroscope entering the SV, a multilocular cystic structure containing ivory-colored, jelly-like seminal plasma. If the orifice was masked behind a thin, transparent membrane-like wall, tentative penetration with the soft head of the guidewire was performed to identify the orifice.
The whole SV was first inspected to exclude the malignant lesions. Then, the pus or blood clots were driven away by manual water irrigation or under the assistance of grasping forceps through the working channel of the seminal vesiculoscope. For calculi, the holmium laser lithotripsy was performed with lower energy (0.5–1.0 W, 10–20 Hz; maximum power 10 W). After stone fragmentation, water irrigation or grasping forceps (Storz) was used to remove the stone fragments. Finally, 0.5% Levofloxacin solution was used to wash both SVs under low pressure. After the procedure, a urethral Foley catheter was placed overnight and removed 24 hours later.
Group B: TSV with ultrasonic lithotripter
The anesthesia and position for patients in Group B were similar to those in Group A. A 3.3F ultrasonic lithotripter (EMS Medical, Switzerland) with 40% energy, introduced through the working channel of the seminal vesiculoscope, was used to get rid of the calculi, blood clot, or purulence in the SV (Fig. 2). The continuous suction function of the EMS lithotripter provided a clear surgical field, also keeping the pressure of SV as low as possible. After the procedure, the same antibiotic solution was injected and a urethral Foley catheter was also placed overnight.
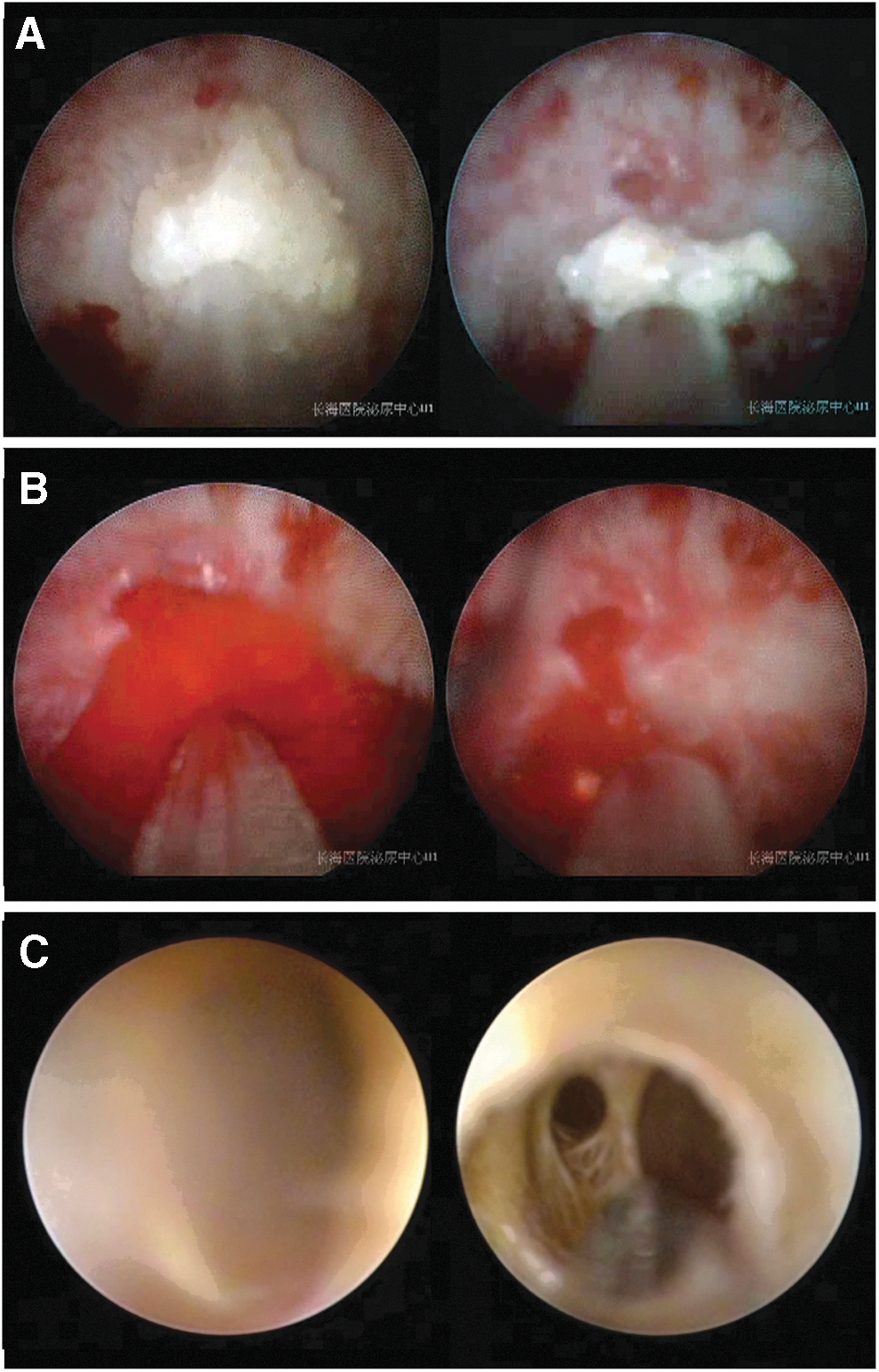
Representative images illustrating the process of disrupting and removing
Postoperative course
Additional oral quinolone antibiotic was given during hospitalization, but sensitive antibiotics were maintained for 1 week if positive culture outcome existed before procedure. All the patients were informed no intercourse for at least 4 weeks. Every patient was followed up by telephone or clinic visits for at most 3 years. Postoperative transrectal ultrasonography was performed at 4 weeks to evaluate the residual blood clot or calculi and recovery of SV volume. For residual blood clots or stone fragments beyond 4 weeks, additional examinations of transrectal ultrasound (TRUS) or CT scan were scheduled every 3 months. In our study, the success of the procedure was defined as the entrance of bilateral SVs through the natural ejaculatory orifice. The recurrence of hematospermia was defined as, at least 1-year follow-up, the occurrence of hematospermia after disappearance. A second TSV with ultrasonic lithotripter was suggested for recurrent hematospermia after failed conservative therapy.
Main outcome measures
Primary outcomes included complication, hematospermia recurrence, and accompanying symptoms alleviation. The operative time and postoperative hospitalization were recorded as secondary outcomes.
Results
A total of 30 patients, 16 in Group A (routine TSV procedure) and 14 in Group B (TSV with ultrasonic lithotripter procedure) were involved in this study. Baseline characteristics of the patients and preoperative imaging findings are summarized in Table 1. There was no significant difference between two groups in any baseline characteristics. As described in Table 1, we could detect SV hemorrhage, SV/ejaculatory duct calculi, SV enlargement, and seminal vesiculitis using TRUS, CT, or MRI (Fig. 3). The median follow-up time for patients in Group A and Group B was 28 (range: 17–36) months and 31 (range: 19–36) months, respectively.
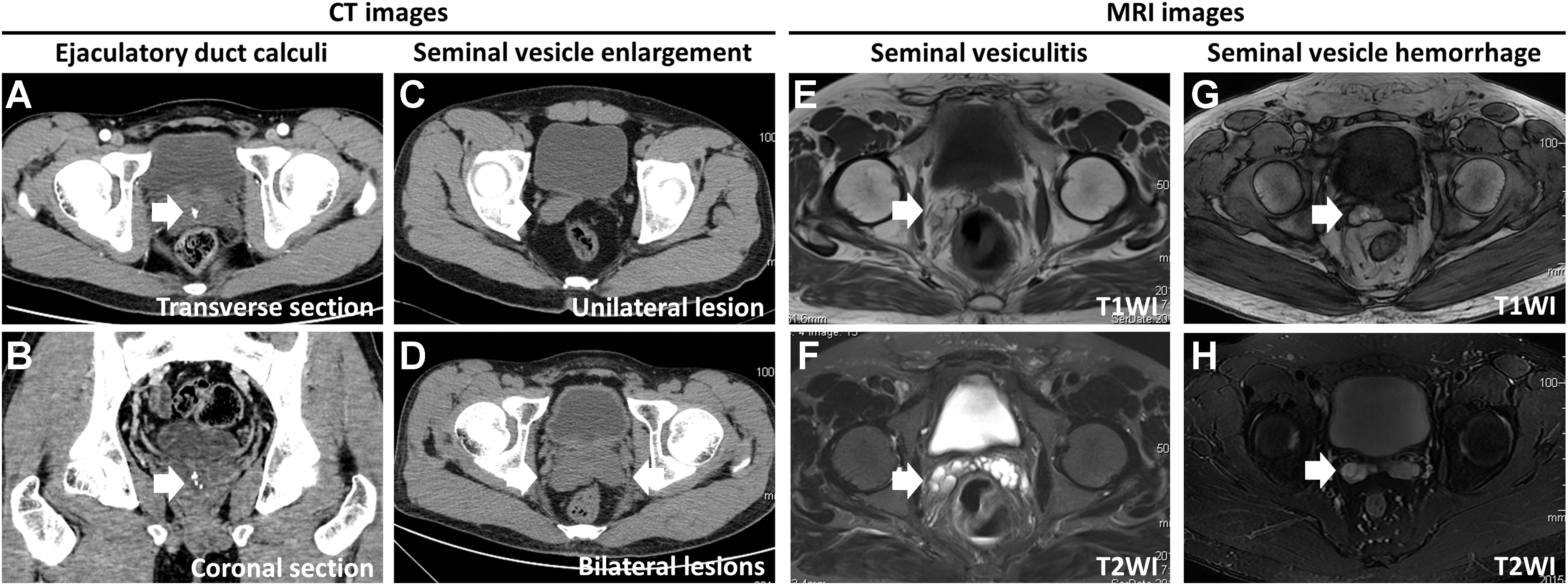
The CT or MRI images illustrating the lesions of ejaculatory duct calculi, SV enlargement, seminal vesiculitis, and SV hemorrhage. The CT images show that multiple calculi are inside the ejaculatory duct in both transverse section
SV = seminal vesicle; TSV = transurethral seminal vesiculoscopy.
Perioperative outcomes of patients and postoperative imaging findings are summarized in Table 2. The mean operative time in Group A and Group B was 66 (range: 35–110) min and 50 (range: 20–93) min, respectively (p < 0.05). The mean postoperative hospitalization was 2 days in both groups (p = 0.883). In almost all the cases, blood clots were observed being accompanied by mucosal edema, congestion, and bleeding. Particulate calculi were also detected in the verumontanum lumen or SVs in eight patients (50.0%) in Group A and nine patients (64.3%) in Group B (p = 0.431). Moreover, the yellow-brown calculi in the ejaculatory duct were found in four patients (25.0%) in Group A and three patients (21.4%) in Group B (p = 1.000).
Accompanying symptoms such as discomfort or pain in perineal region, frequent micturition, and ejaculatory pain/discomfort were, respectively, alleviated in 3/5, 4/4, and 1/1 patients in Group A and 3/4, 2/3, and 3/3 patients in Group B (all p = 1.000). TRUS or CT scan confirmed resolution of SV blood clot, absence of SV calculi, reduction of SV volume, and disappearance of seminal vesiculitis, respectively, in 4/4, 2/3, 5/6, and 5/7 patients in Group A and 5/5, 4/5, 8/10, and 6/7 patients in Group B (all p = 1.000).
In Group B, all the TSV procedures were successful, except one patient had a two-stage procedure because of right SV stones accompanying with pus. In the first procedure of TSV, right ejaculate orifice obstruction was relieved to drain the pus. Then, the lithotripsy was finished in the second procedure for the sake of safety. In Group A, one patient had the discontinuation of the procedure because of accidental bleeding during stone fragmentation. During the follow-up, two patients in Group A had recurrent hematospermia and underwent the second TSV, whereas no recurrence happened in Group B. Of the recurrent cases, one patient had residual stone fragments, whereas the other had hemorrhage in the left SV. In both the groups, no epididymitis, retrograde ejaculation, rectal injury, incontinence, bladder neck contracture, or erectile dysfunction happened during the maximum of 3-year follow-up.
Discussion
Inflammation, infection, malignancy, vascular anomalies, or other genitourinary lesions are the pathological factors of hematospermia. 11 Of all the identified causes, infection is the most common one. As the hematospermia symptoms in most patients are self-limiting or will disappear after antibiotic treatment, conservative therapy is the usual course of action. 3 This is also the reason why in our study, only patients with severe and persistent hematospermia even after long-term antibiotic treatment are indicated for TSV procedures. Furthermore, TSV has been considered a safe procedure since the first report by Yang and colleagues. 3 However, acute epididymitis after surgery has been reported in several studies. 4,12,13 Although the epididymitis is rare and convalescent without sequela, this complication is still the consideration for men who have never fathered. Thus, the negative microorganism culture outcome before surgery was mandatory in our study.
In this study, we found less operative time in Group B compared with Group A because of using ultrasonic lithotripter. To our knowledge, this is the first report of TSV combined with ultrasonic lithotripter to treat hematospermia. The ultrasonic lithotripter makes TSV a time-saving procedure just as described below. First, the ultrasonic lithotripter can suction stone fragments during the lithotripsy. Second, compared to intermittent, hand-controlled irrigation with 0.9% normal saline, it is efficient to suction clot, pus, and the other debris, thus providing improved visibility and more precise intervention. The last, but not least, the new technique reduces or eliminates the repeated intraoperative exchanges of endoscopic instruments, which can be technically challenging and time-consuming. However, we also found the mean operative time in both groups was longer than 30 minutes, the average operative time reported in literatures. 13 –16 This may be ascribed to the higher proportion of patients with calculi in our study, and lithotripsy is a more time-consuming procedure than simple seminal vesiculoscopy. Although the longer operative time was required in this study, no epididymitis or the other infection-related complications happened. It further suggests that the “sterile status” before surgery is helpful to control the infection after surgery.
Calculi was the most frequent diagnosis (47.4%) in patients with persistent hematospermia, and the first case of endoscopic laser lithotripsy of SV calculi was reported in 2005. 17,18 Since then, laser lithotripsy has been widely used for SV calculi treatment. However, in our study, a patient had to discontinue the procedure because of heavy bleeding during laser lithotripsy, which might be caused by accidental laser damage to the SV mucosa. However, ultrasound lithotripsy almost does no harm to the mucosa. In addition, laser lithotripsy is more suitable for small calculi in SV. 19 Large calculi can be fragmented into pieces by laser lithotripsy, but the fragments are difficult to be expelled by hand-control water irrigation, whereas grasping forceps or stone baskets are more invasive. However, ultrasonic lithotripsy can easily remove stone fragments even for large calculi. At the same time, the strong suction function of the ultrasonic lithotripsy can keep the SV pressure as low as possible, instead of fluctuating pressure with hand-control water irrigation. Actually, excessive intraoperative pressure might cause destruction of the epithelium and damage the internal structure of the SV. 14 In our study, a patient with calculi accompanied by pus in SV was treated by a two-stage ultrasonic lithotripsy, and he had no infection complications and no calculi recurrence during the follow-up. The ultrasonic lithotripsy reduces the risk of infection and makes TSV a much safer procedure.
There were two patients (6.7%) in our study having recurrent hematospermia, similar to the recurrence rate of 0.9% to 10% reported by the other literatures. 4,8,16 The repeated ejaculate orifice obstruction is considered to be the main cause for recurrent hematospermia; however, the residual stone fragment is also an unignorable pathological factor. In our study, one of the two patients suffered with recurrent hematospermia just because of the residual stone fragments. The vicious cycle of calculi, obstruction, inflammation, and stricture may eventually lead to recurrent and refractory hematospermia. 4 Interestingly, no patient in Group B had recurrent hematospermia caused by residual stone fragments during long-time follow-up. This may benefit from the efficient elimination of stone fragments by ultrasonic lithotripsy.
Nowadays several studies have reported the improvement of ejaculation or semen parameters after TSV procedures. 20 –22 However, even so, in this study, no patient who has not yet fathered was enrolled to avoid accidental damage of seminal vesiculoscopy on potential fertility; correspondingly, we have no further preprocedure and postprocedure analysis for differential outcome of the semen parameter. However, we acknowledge that the impact of seminal vesiculoscopy on semen is an important issue and worth further study to investigate the fluctuation of the parameters of ejaculation and semen after the surgical intervention, especially for infertile patients with ejaculatory tract obstruction.
Otherwise, ultrasonic lithotripsy seems to add the cost of seminal vesiculoscopy; however, it spares holmium lithotripsy, resulting in the balance of the final expense. The other limitations include small number of patients in the study, a retrospective analysis, potential treatment choice bias, and subjective assessment of erectile dysfunction and retrograde ejaculation; however, fortunately there is no significant difference on the baseline characteristics of patients and preoperative imaging findings between the two groups. Even so, future high-quality, large-scale multicenter trials are still necessary.
Conclusion
Our initial experience demonstrates that TSV with ultrasonic lithotripter enables a more reliable, effective, and convenient procedure to diagnose and treat severe, persistent hematospermia compared to the traditional technique. The innovative technique greatly controls the recurrent hematospermia with less operative time and complication.
Footnotes
Acknowledgment
We thank Dr. Tom F. Lue from Department of Urology, University of California, San Francisco, for his valuable proposals to our article.
Author Disclosure Statement
No competing financial interests exist.