
Abstract
Smart Simulator is a new advanced bench training model for achieving proficiency in flexible ureteroscopy (fURS). Its important features are portability and the ability to simulate breathing-induced kidney movements, model pyelocalices similar to those in humans, create a situation closely resembling a fURS field, and create papillae of a size equivalent to that of the access sheath. Smart Simulator thus creates a situation more closely resembling that in a clinical setting than the other bench training models for fURS. Sixteen urologists experienced in fURS assessed the Smart Simulator for face validity and content validity. The model was acceptable in terms of realism, acceptability, and feasibility. Trainees can use it to practice laser manipulation for kidney stone fragmentation and retrieval in accord with breathing-induced movements and various other created fields sometimes confronted during fURS. Training in situations in nearly real fURS surgical fields may improve trainees' technical skills.
Introduction
P
We, therefore, introduce a new advanced bench model for fURS training called the Smart Simulator (Olympus, Tokyo, Japan). This simulator has five important features: portability, ability to create breathing-induced kidney movements, ability to model pyelocalices similar to those in humans, ability to create a situation closely resembling an fURS field, and ability to create a papilla size equivalent to that of the access sheath. Furthermore, we evaluate the face and content validity to assess the utility of the new advanced bench model for fURS training. In addition, we compare the face and content validities of the new advanced bench model with those of a high-fidelity bench model as described earlier: Scope Trainer (Mediskills, Northampton, United Kingdom).
Smart Simulator
The portable Smart Simulator (length 30 cm, width 56 cm, height 31.5 cm; weight 9 kg) has two components: a simulated breathing-induced kidney movement system and an irrigation system (Fig. 1A, B). The breathing-induced movement of the kidney is simulated by a rolling electric motor built into a box. This system can be set to simulate the chosen motion speeds—respiratory frequencies of 10–25 times/minute—with the motion width of the kidney of 0- to 55-mm amplitude according to the surgeon's skill (Fig. 1C, D). This system can also be changed according to the slope of the kidney based on the surgeon's expertise (Fig. 1E, F). The pyelocalices model used in this simulator was made using a three-dimensional (3D) printer based on 3D computed tomography images from many patients. The type A1 model (from among types A1, A2, B1, and B2 pyelocalices models), as reported by Sampaio and Mandarim-Lacerda, was used in this study (Fig. 2). 4 This kidney model is constructed from high-tensile elastomeric silicone.

Smart Simulator and its components:
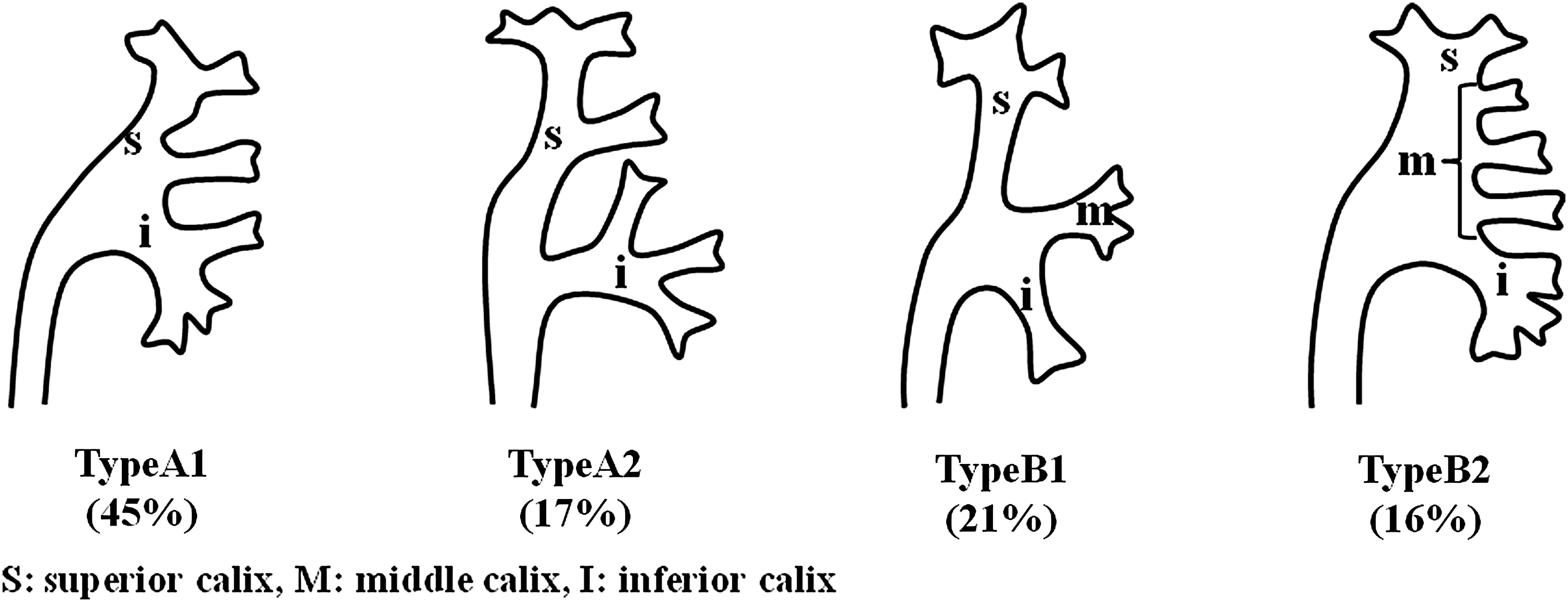
Morphological classification of the kidney's collecting system. Types A1 and A2 anatomy, with superior and inferior calices. In type A2, the kidney midzone is drained by crossing calices. Types B1 and B2 anatomy, with superior, middle, and inferior calices. In type B2, the kidney midzone is drained by one to four minor calices that enter the renal pelvis directly.
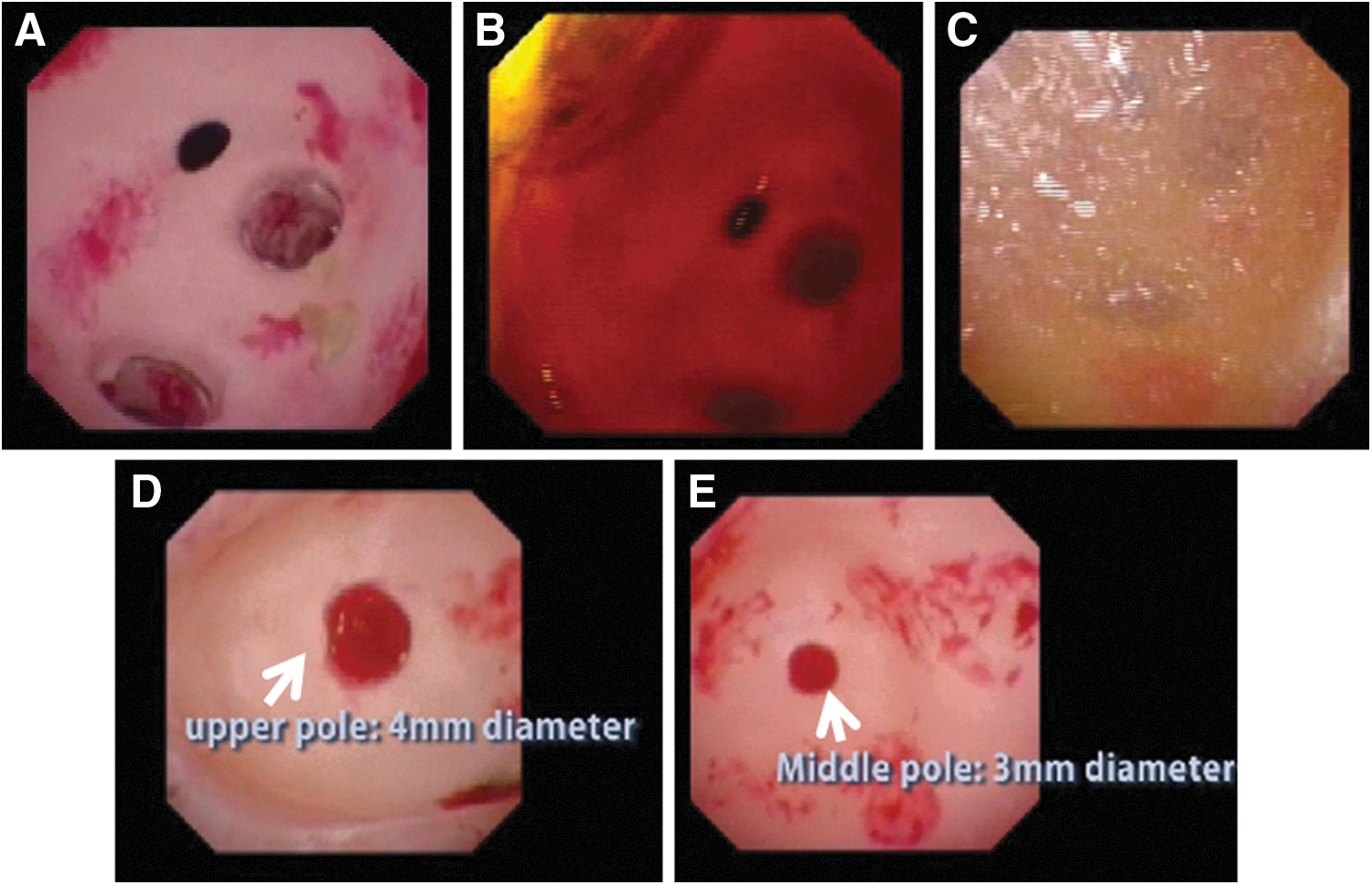
The irrigation system built into this simulator creates a situation similar to that of the actual fURS surgical field. This system consists of a tube that conducts continuous saline irrigation from a saline tank and a ureteral drainage tube through which the saline exits. Thus, trainees can not only perform fURS in the presence of clear saline irrigation of the pyelocalices but also in a surgical field in which hematuria and stone dust can be created (Fig. 3A–C). Consequently, trainees can practice laser manipulation for stone fragmentation and retrieval from a kidney with ongoing simulated breathing-induced movement and variously created fields.
Internal anatomy.
The other novel characteristics of the Smart Simulator is that the papilla size in each minor calices is equivalent to the access sheath size, allowing the trainee to become accustomed to judge whether a fragment can pass through the access sheath before confronting the problem in clinical practice (Fig. 3D, E). Papilla sizes in upper pole and central region are 4 and 3 mm, respectively, which are equivalent to fragment sizes accepted by 12–14F and 10–12F access sheaths, respectively (see Supplementary Video 1; Supplementary Data are available online at
Face and Content Validity
We measured face and content validities to assess the model's utility for fURS training. Sixteen urologists experienced in fURS (>50 fURS procedures) were invited to complete some structured questionnaires and assess the realism, acceptability, and feasibility of the model. The five questions assessing face validity included questions about anatomical resemblance, ureteral observation, pyelocaliceal observation, instrument handling, and breathing-induced kidney movement; four questions assessing content validity included availability for training, interest for bench simulator, improvement of fURS technique, and availability of kidney movement for training. First of all, they performed the hands-on experience using URF P6 (Olympus Corporation, Japan) for 3 minutes on both Smart Simulator and Scope Trainer. Thereafter, they gave a quick answer to each question. The measurement used a Likert scale (1 = poor, 7 = excellent; >4 = acceptable threshold). The new advanced bench model was acceptable in all questions of face validity and content validity. In particular, the breathing-induced kidney movement was strongly agreed to be acceptable (6.31 ± 0.79). Furthermore, the availability of kidney movement for training was also most useful (6.75 ± 0.44) (Fig. 4A, B).
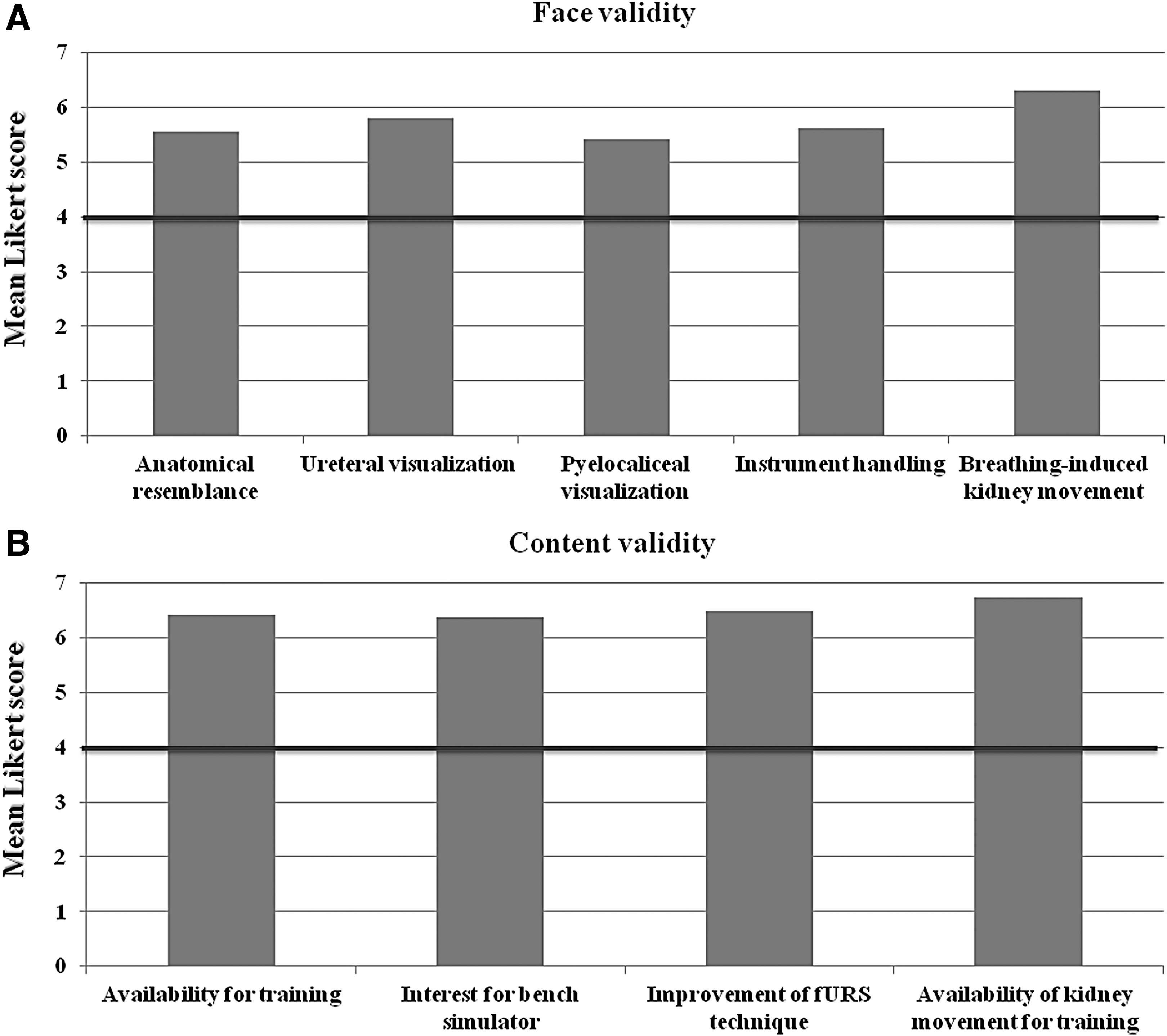
Face and content validity for new advanced bench model; Smart Simulator. Mean Likert scale evaluated by 16 urologists with experienced hands of fURS is demonstrated by each item (1 = poor, 7 = excellent; >4 = acceptable threshold).
We compared the face and content validities of the new advanced bench model with those of an earlier Scope Trainer. The new advanced bench model was superior to the Scope Trainer in all questionnaires (p < 0.0001) (Table 1; Appendix).
N = 16 urologists with experienced hands of fURS.
Data are presented mean ± standard deviation.
Mann–Whitney U test.
fURS = flexible ureteroscopy.
Discussion
The Smart Simulator was the model that best simulated fURS procedures and was found to be the most acceptable for fURS training in our validation study. This simulator creates situations that closely resemble those of actual fURS surgical fields, which could result in trainees achieving greater technical skill before attempting the procedure in the clinical setting. Such trainees can practice laser manipulation for stone fragmentation and retrieval from the kidney with simulated breathing-induced movements of kidney and in variously created fields.
“See one, do one, teach one”—this age-old saying has been handed down during surgical training for many generations. 5 Medical education, however, is undergoing a paradigm shift, from the traditional experience-based model to a program that requires documentation of proficiency. Therefore, it is no longer acceptable for trainees in any surgical area to practice basic technical skills on patients. 1 A training model can thus facilitate the acquisition of skills deemed essential for the procedure. Matsumoto et al. reported that the performance of a ureteroscopic bench model group was significantly better than the didactic group. 6 Liang and colleagues found that a virtual reality simulator training program helped trainees rapidly improve their retrograde skill in URS. 7 Hands-on training using bench models and virtual reality simulators can effectively teach novices basic endourologic skills.
Some basic training models on which to practice technical skill needed for URS—for example, the low-fidelity bench model (K-box; Proges-Coloplast, Rosny-sous-Bois), high-fidelity bench model (Scope Trainer; Mediskills), and virtual reality simulator (URO Mentor; Simbionix, Lod, Israel)—are currently available and useful for trainees before entering clinical practice. 1 The advantage of these training models has already been proven. Although trainees can quickly master fURS using these basic training models, they are still not prepared for maneuvering in the real fURS surgical field. In clinical practice, breathing-induced movement of the kidney, a poor view of the surgical field caused by hematuria or stone dust, or the varying anatomy of the kidney may confuse the novice. The Smart Simulator, as a novel advanced bench training model, can create these situations in which to practice before attempting the procedure in the clinical setting.
Advanced models for ureteroscopic training currently available are animal models and human cadavers, which have many advantages, including their high fidelity and being a true anatomic simulator. 3 Reports of using these animal and human tissues, however, are scarce. In addition, ethical considerations, legal issues, animal licenses, and the difficulty of repeating such training remain. Using the Smart Simulator not only addresses these issues, it allows repeat fURS training.
Sampaio and Mandarim-Lacerda divided the pyelocalices into four types based on the superior, middle, and inferior great calices according to drainage of the polar region from 140 polyester casts of human renal cavities. 4 Types A1 and A2 (62% of the specimens) have the features of two great (superior and inferior) calices. In type A1 (45%), the kidney midzone is drained by minor calices that are dependent on both superior and inferior caliceal groups. In type A2 (17%), the kidney midzone is drained by crossing calices. Types B1 and B2 (38%) have the features of three great calices (superior, middle, and inferior calices), In type B1 (21%), the kidney midzone is drained by a major caliceal group independent of the superior and inferior groups. In type B2 (16%), the kidney midzone is drained by one to four minor calices entering the renal pelvis directly. 8 The reason for selecting type A1 in this study was that it is the most popular, standard type. Furthermore, broader pyelocalices are easy to manipulate and difficult to injure during fURS compared with the other models. The next pyelocaliceal models are currently in preparation.
This kidney model including the ureter and calices is constructed from high-tensile elastomeric silicone. Therefore, the surfaces of its ureter and kidney are often sticky. Immersing the lumen in saline decreases the stickiness and resistance during fURS training. However, surface membrane structures of the ureter and kidney often peel off during fURS handling in saline environments. Conversely, we rarely experience resistance to handling of fURS in human tissue. This difference between the silicone bench model and human tissue is a significant issue. Therefore, the ureteral access sheath is best placed so that it decreases the resistance for fURS training in this bench model.
Cost is always a concern when establishing/maintaining a technical skills laboratory. In the only comparison study available, the cost of building a low-fidelity model was $20 (Canadian) and that for a high-fidelity model was $3700 (Canadian). 6 Although the virtual reality simulator improves clinical skills, its use is limited by the high cost. The development costs for the present new advanced bench model were about $10,000 (United States). This cost was higher than the other bench models. Cost effectiveness analysis plays an important role in selecting a model for establishing a technical skills training program. The cost of the Smart Simulator must also be considered in this regard.
There are some limitations of this study. First is the advantage of fURS training using the Smart Simulator was not clarified. Further research on the construct validity of this simulator for training is required in the future. Second is that it is unclear how the simulator should be incorporated into training. Therefore, a comparison between the basic model and the advanced model for fURS training should be undertaken to decide the role of each model for fURS training.
Conclusion
The Smart Simulator can create situations that closely resemble those confronted in clinical practice. Using a portable simulator that offers breathing-induced movement of the kidney, a pyelocalices model that projects anatomy similar to that in humans, situations closely resembling the actual fURS surgical field, and a papilla size equivalent to that of the access sheath size facilitates the acquisition of skills required for fURS. Training with this simulator for novice trainees before attempting it in the clinical setting may improve the technical skills of trainees more rapidly and in more detail than other simulators.
Footnotes
Acknowledgment
The development of the new advanced simulator was supported by a grant from Olympus Corporation.
Author Disclosure Statement
This study was funded by Olympus Corporation.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.