
Abstract
Objective:
The majority of patients undergoing partial nephrectomy (PN) present with a clinical T1a tumor with both kidneys present. Some groups have advocated using off-clamp (Off-C) techniques to eliminate warm ischemia whenever possible, even when elective. We evaluated whether Off-C technique during robotic PN (RPN) provides any functional benefit over main arterial clamping (MAC) in these patients.
Subjects/Patients and Methods:
A total of 351 patients with a R.E.N.A.L. nephrometry score (RNS) <10, T1a tumor, and two kidneys who underwent RPN from five high-volume surgeons between 2008 and 2016 were retrospectively identified from a multi-institutional database. MAC and Off-C patients were 2 to 1 nearest neighbor propensity score matched on tumor size, RNS, % endophytic, tumor location, age, gender, body mass index, comorbidities, baseline estimated glomerular filtration rates (eGFRs), and surgeon performing the RPN. Preoperative, surgical, and postoperative outcomes were compared.
Results:
After propensity score matching, 82 MAC and 41 Off-C RPN patients were compared with no remaining statistically significant differences in baseline demographic or tumor-specific characteristics, including tumor size (p = 0.203) or RNS (p = 0.744). There were no significant differences in complications (p = 0.141), positive surgical margins (p = 0.625), or non-neoplastic parenchymal volume removed (p = 0.138). Off-C RPN had significantly higher estimated blood loss (100 mL vs 50 mL, p < 0.001), but no increased rate of transfusion (p = 0.328). There were no significant differences in rates of acute kidney injury (p = 0.132) nor percentage change in eGFRs (p = 0.763) at discharge. Freedom from progression of chronic kidney disease (CKD) stage was 87.7% for MAC and 91.1% for Off-C at 12 months. The percentage change in eGFRs (p = 0.457) and CKD stage progression (p = 0.866) was not different at last follow-up (median 9.2 months).
Conclusion:
Our data showed that the use of Off-C RPN marginally increased blood loss without providing a renal function benefit. In two-kidney patients presenting with a T1a renal tumor, Off-C RPN may not be necessary.
Introduction
K
Patients and Methods
This study identified 914 patients undergoing Off-C or main arterial clamping (MAC) RPN at five medical institutions for a T1a tumor between January 2008 and June 2016 from a multi-institutional database. All data are stored in Research Electronic Data Capture (REDCap), an IRB-approved online database with both data merged from individual institutional prospective databases before December 2014 and prospective data recorded in the database since that date. All RPNs were performed transperitonealy and the choice of surgical technique was made at the discretion of the surgeon with Off-C utilized at rates of 32% (n = 12), 20% (n = 34), 15% (n = 11), 0% (n = 0), and 0% (n = 0) among the five included surgeons. No cold ischemia was used in this cohort and no patients underwent selective clamping in this cohort. To limit the cohort to tumors that were equally amenable to either an Off-C or MAC approach, several patients were prospectively excluded from the cohort. Patients with a solitary kidney (n = 9), a R.E.N.A.L. nephrometry score (RNS) >9 (n = 96), a mass abutting the main renal artery or vein (n = 78), multiple renal masses resected (n = 20), previous ipsilateral kidney surgery (n = 21), baseline estimated glomerular filtration rates (eGFRs) <30 (n = 10), known metastatic disease (n = 1), a horseshoe kidney (n = 2), tumor thrombus (n = 2), conversion to radical or open PN (n = 3), missing complete follow-up data between 3 and 18 months (n = 302), and/or missing clamp technique data (n = 22) were excluded from the analysis. After exclusion criteria, 57 Off-C and 294 MAC patients were available for analysis.
Baseline demographic, tumor-specific, and intraoperative data included age at surgery, gender, body mass index (BMI), American Society of Anesthesiologists (ASA), hypertension, diabetes, coronary artery disease, chronic kidney disease (CKD), age-adjusted Charlson comorbidity index (CCI), baseline eGFRs, history of abdominal surgery, pole of the tumor, tumor laterality, anterior vs posterior vs lateral tumor location, tumor size, percentage endophytic of the tumor, and RNS, date of surgery, the use of indocyanine green, and renal vein clamping. As has been previously shown, 9 renal function outcomes are influenced by underlying medical comorbidities, and accordingly these were included in propensity score matching.
Intra and postoperative data including WIT, estimated blood loss (EBL), operative time, rates of collecting system entry, non-neoplastic parenchymal volume (NNPV) removed, positive surgical margin (PSM) rates among malignant cases, rates of overall, medical, surgical, and major (Clavien score ≥3) postoperative complications, length of hospital stay ≥3 days were compared between groups. Kidney function outcome at discharge, including the percentage change in eGFRs and acute kidney injury (AKI) in addition to the percentage change in eGFRs and progression to CKD at the most recent follow-up between 3 and 18 months (median 9.2 months) were compared between groups. NNPV was calculated using a previously defined method. 10 The modification of diet in renal disease (MDRD) formula was used to calculate eGFRs. 11 Risk Injury Failure Loss End-Stage Kidney Disease (RIFLE) criterion of a >25% reduction in eGFR was used to define AKI. 12 Progression to CKD was defined as an increase from baseline CKD stage 1 or 2 to ≥3, stage 3 to ≥4, or stage 4 to 5 at a median follow-up of 9.2 months.
Propensity score matching
MAC and Off-C patients were nearest neighbor 2 to 1 propensity score matched on age, gender, BMI, ASA score ≥3, diabetes, hypertension, coronary artery disease, baseline eGFRs (mL/min/1.73/m2), tumor size (cm), RNS, tumor laterality, lateral vs anterior/posterior tumor location, percentage of tumor endophytic, and operating surgeon. A 2 to 1 ratio was chosen to increase the number of patients used for matching, given the large number of available MAC patients. 13 Propensity score matching provided 41 Off-C and 82 MAC patients for analysis. Only patients with complete data on matched parameters were included in the propensity score-matched analysis. Propensity score matching was conducted using the MatchIt package in R (version 3.1.3). 14
Subanalyses
Subanalyses were also done to compare Off-C and MAC patients with simple complexity tumors (i.e., RNS ≤ 6) and also for patients with an eGFR < 90 after 1:1 propensity score matching age, gender, BMI, ASA score ≥ 3, diabetes, hypertension, coronary artery disease, baseline eGFRs, tumor size, RNS, tumor laterality, lateral vs anterior/posterior tumor location, percentage of tumor endophytic, and operating surgeon. There were insufficient patients in the cohort with both small renal masses and MAC WIT >25 minutes to perform an accurate analysis of Off-C vs MAC in this setting.
Predictors of receipt of Off-C
Multivariable logistic regression analysis of predictors of receipt of Off-C as opposed to MAC was conducted to gain insight as to why surgeons opt for Off-C vs MAC among T1a renal masses during RPN.
Statistical analysis
Frequencies and percentages were calculated for categorical variables, medians, and interquartile ranges for continuous variables, and each were calculated/presented based on the number of patients with complete data on that particular variable. Mann–Whitney U tests were used to compare continuous variables, whereas chi-squared or Fisher's exact tests were used to compare categorical variables with significance considered at the p < 0.05 level. A log-rank test was used to compare progression of CKD stage. Statistical analysis was performed using R version 3.1.3 and IBM SPSS version 20.0.
Results
Baseline characteristics
Baseline demographic and tumor-specific characteristics for the pre- and postpropensity score-matched cohorts are presented in Table 1. For the propensity score-matched cohort of 41 Off-C and 82 MAC patients, no differences in tumor size (p = 0.203), RNS (p = 0.744), age (p = 0.908), gender (p = 0.516), BMI (p = 0.344), age-adjusted CCI (p = 0.646), baseline eGFRs (p = 0.994), pole of the tumor (p = 0.256), tumor laterality (p = 0.920), percentage endophytic (p = 0.795), and other demographic or tumor-specific characteristics were identified.
Statistical significance is highlighted by bold values.
Categorical variables presented as frequencies.
Continuous variables presented as medians with interquartile ranges, ranges in parentheses.
ASA = American Society of Anesthesiologists; BMI = body mass index; CCI = Charlson comorbidity index; CKD = chronic kidney disease; ICG = indocyanine green; eGFRs = estimated glomerular filtration rates.
Perioperative outcomes
Perioperative outcome for the pre- and postpropensity score-matched cohorts is presented in Table 2. In the propensity score-matched cohort, WIT (0 minutes vs 11.0 minutes, p < 0.001) was higher in the MAC group, whereas EBL (100.0 mL vs 50.0 mL, p < 0.001) was higher in the Off-C than in MAC patients. No differences in any other perioperative outcomes were identified, including postoperative complications (p = 0.141), perioperative blood transfusion (p = 0.328), NNPV removed (p = 0.138), and PSMs (p = 0.625).
Statistical significance is highlighted by bold values.
Categorical variables presented as frequencies.
Continuous variables presented as medians with interquartile ranges, ranges in parentheses.
AKI = acute kidney injury; NNPV = non-neoplastic parenchymal volume.
Kidney function outcomes
Kidney function outcomes for the pre- and postpropensity score-matched cohorts is presented in Table 2. In the propensity score-matched cohort, the percentage change in eGFRs (p = 0.763) and AKI (p = 0.132) at discharge was not different. Freedom from progression of CKD stage was 87.7% for MAC and 91.1% for Off-C at 12 months. The percentage change in eGFRs (p = 0.457) and progression to CKD (p = 0.866) (Fig. 1.) at median 9 months were each not statistically significantly different.
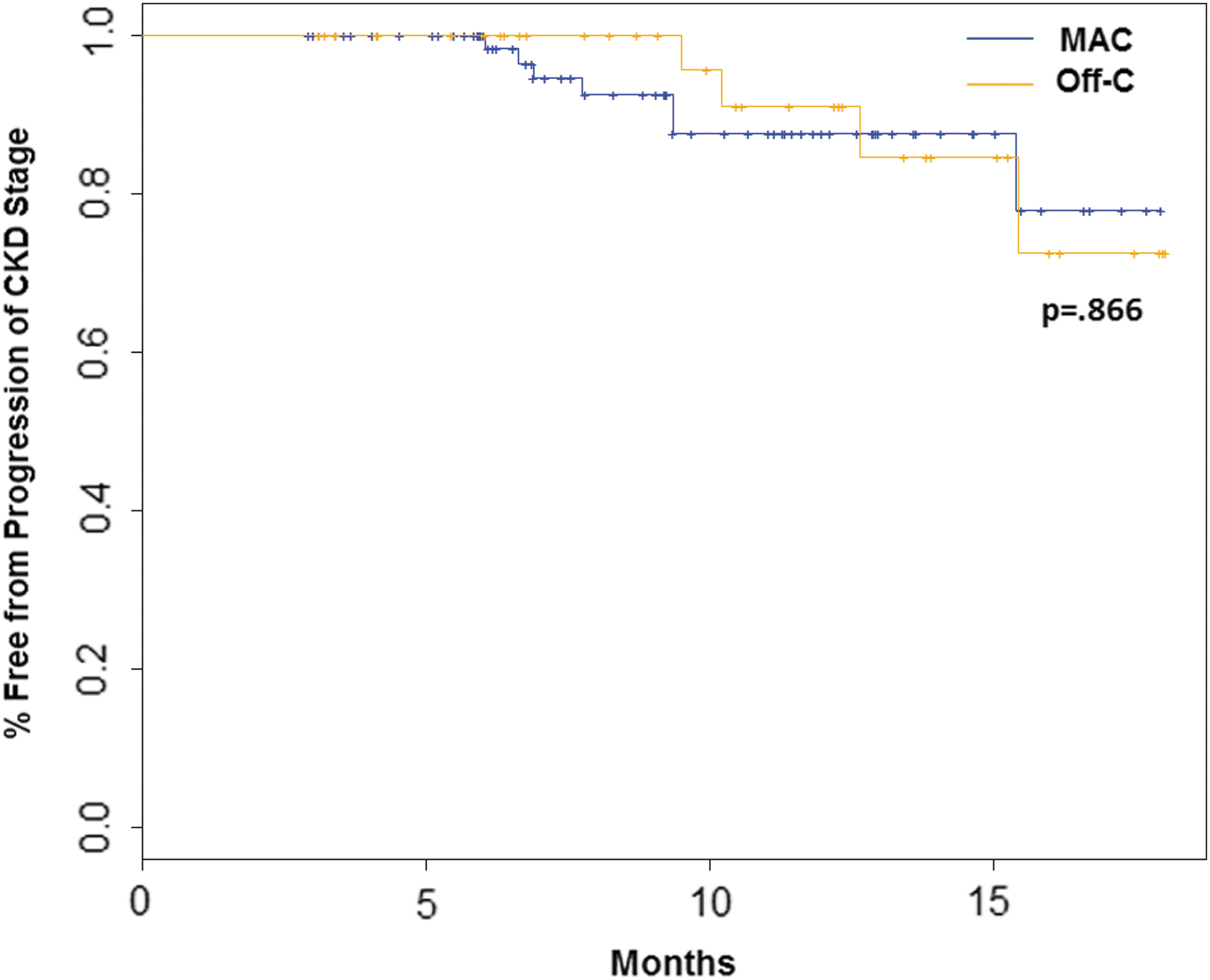
Kaplan–Meier curves of freedom from progression of CKD stage at median 9 months between patients undergoing MAC or Off-C RPN. CKD = chronic kidney disease; MAC = main arterial clamping; Off-C = off-clamp; RPN = robotic partial nephrectomy.
Subanalyses
Among 29 Off-C and 29 MAC propensity score-matched patients with a simple complexity tumor (RNS ≤6), no difference was identified in the percentage change in eGFRs (p = 0.919) or rate of AKI (p = 0.249) at discharge, nor in the percentage change in eGFRs (p = 0.484) or progression of CKD stage (p = 0.999) at 8.3 months. Among 24 Off-C and 24 MAC propensity score-matched patients with a baseline eGFR between 30 and 90, no difference was identified in the percentage change in eGFRs (p = 0.851) or AKI (p = 0.999) at discharge, nor in the percentage change in eGFRs (p = 0.877) or progression to CKD (p = 0.999) at 9.7 months.
Predictors of receipt of Off-C RPN
Patients with larger tumors (OR = 0.25, 95% CI = 0.14, 0.46; p < 0.001) and right kidney tumors (OR = 0.31, 95% CI = 0.13, 0.72; p = 0.006) were less likely to undergo Off-C, whereas males were more likely to undergo Off-C (OR = 2.51, 95% CI = 1.03, 6.11; p = 0.042) than females. Baseline eGFRs (p = 0.143), history of abdominal surgery (p = 0.921), anterior/posterior tumor location (p = 0.271), percentage endophytic (p = 0.235), and date of surgery (p = 0.184) were not associated with receipt of Off-C RPN.
Discussion
As PN has become the preferred treatment of small renal masses, 15 a growing chorus of literature has advocated the virtues of the Off-C technique to eliminate ischemia and maximally preserve renal function. Patients with a solitary kidney with compromised renal function or complex tumors where ischemia is likely to be longest are most likely to benefit from an Off-C RPN; but, in both this data set and in the literature, 16 Off-C is actually more often selected for use in smaller and anatomically simpler tumors. Our results suggest that for these cases Off-C may not be necessary, as Off-C RPN showed no advantage over MAC RPN in two-kidney patients with T1a tumors.
This cohort was created to serve as an accurate comparison of the two surgical techniques' ability to treat a solitary T1a renal mass. First, by using propensity score matching, we minimized the selection bias of using Off-C RPN on smaller, more exophytic tumors. Second, even before propensity score matching, our patients' baseline characteristics were comparable, including the age, gender, prevalence of CKD, diabetes, overall ASA score, and age-adjusted CCI. In addition, variables that portend a more complicated surgery, such as BMI or a history of abdominal surgery, were also comparable. It is notable that our MAC patients had low WITs (median 13 minutes IQR: 9.9–17.3), likely because our analysis was limited to simpler, smaller tumors. Our findings are, therefore, generalizable to patients with low–intermediate cT1a tumors with short ischemia time. Although the benefits of Off-C may be more likely to be realized in cases wherein longer WIT would be expected (i.e., in a larger, more complex tumor), our findings are not generalizable to this cohort, though these cases would also likely be cases that would be difficult to perform without MAC. The results from this study correlate with similar data reported by our group, showing no advantage to selective arterial clamping under low WIT. 17
Our results differ from several prior studies in this field. In both the open and laparoscopic setting, Off-C has been suggested to be superior to MAC in terms of postoperative renal function, although not all studies found an advantage. 4 –8,18 –24 Two meta-analyses comparing the techniques found a benefit to the Off-C approach, although the included studies contained a mix of open, laparoscopic, and robotic techniques, and many show a trend toward Off-C surgeries being performed on smaller tumors. 22,25 Laparoscopic and open Off-C may be considered separately, as with the exception of intracorporeal ice slush, 26 laparoscopic and robotic techniques rely on WIT. A notable laparoscopic study by Porpiglia et al. that used renal scintigraphy for evaluation of renal function found that Off-C PN did not offer any functional advantage over MAC in a cohort with low WIT, 7 consistent with our findings in this study. Among other robotic cohorts, Kaczmarek et al. 8 and Tanagho et al. 18 and Mouracade et al. 19 found small improvements in percentage of eGFRs preserved, whereas Spencer Krane and colleagues. 21 and Komninos and colleagues 20 did not find any significant difference.
In the largest published robotic study, Kaczmarek et al. found a small renal function benefit while propensity score matching, but several differences between our studies are notable. First, their study included tumors with a RNS of up to 12. Our study focused on smaller and lower complexity tumors to create conditions wherein Off-C and MAC are equally likely to be used. Furthermore, although the study also controlled for RNS, it did not explicitly control for tumor size, which in our cohort is the predominant determinant of postoperative renal function, potentially introducing a meaningful difference in our cohorts. In addition, we examined and controlled for medical comorbidities, including hypertension and diabetes, which are known risk factors for CKD that can independently negatively affect renal function. 27 The confluence of these factors may explain why our data differ from the literature.
Across clinical postoperative variables, we failed to find an advantage of the Off-C technique. After propensity score matching, we found an advantage neither in the amount of NNPV removed nor in short- or long-term renal function outcomes (p > 0.05). Although Off-C surgeries are bloodier, making them both visually and technically more difficult, we did not find any increase in PSM, postoperative complications, or length of stay. Despite the increased blood loss (100 mL vs 50 mL, p = 0.007), we saw no difference in requirements for transfusion, and Off-C RPN may remain a viable surgical option for amenable tumors in the hands of experienced robotic surgeons.
Our study has several limitations through which it should be understood. First, selection bias plays a prominent role in retrospective studies. In this retrospective study, the specific reasons for which Off-C vs on-clamp technique was used during a case are unknown; however, the size of the tumor, a tumor in the right kidney, and male gender were identified as the predictors of selection for Off-C RPN. Accordingly, we attempted to minimize this selection bias through propensity score matching, after which our cohorts had comparable baseline characteristics, including tumor size (p = 0.707), RNS (p = 0.943), gender (p = 0.516), and tumor laterality (p = 0.578). Although a surgeon may be more likely to select more exophytic and smaller tumors for Off-C RPN, this bias was effectively removed from our propensity-matched cohort as well (p = 0.489). Second, the overall low WIT of our MAC cohort prevented us from also commenting on the role of Off-C RPN in patients with long WIT. Third, our study uses eGFRs and the MDRD technique for calculating renal function, which is not always accurate for determining long-term renal function. MAG3 renal scans are more accurate, but unfortunately were not available for the vast majority of our patients. Another limitation of this analysis is that failure to observe a difference in renal function outcome may be because of low statistical power driven by the relatively low number of patients analyzed in the propensity score-matched cohort (n = 82 MAC, n = 41 Off-C). Future studies with more patients are needed to validate these results. In addition, this study focused on the most common patient, with relatively healthy renal function and two kidneys, which is also the patient least likely to show a difference in clamp technique outcome. Although our cohort did not have sufficient solitary kidney patients nor patients with CKD or extended WIT to also accurately assess the effects of Off-C in these situations, the results from this study are highly generalizable because the majority of patients undergoing PN have two healthy kidneys and noncomplex tumors.
Conclusions
Off-C RPN appears to be an equivalent, but not superior, technique to MAC RPN in terms of renal function, cancer control, and complication rates in low complexity tumors. In healthy patients with smaller, less complex tumors with expected short WIT, the usage of Off-C RPN does not appear to offer any long-term clinical outcome benefit and may not be necessary.
Footnotes
Author Disclosure Statement
Dr. Eun reports receiving personal fees from Intuitive Surgical, personal fees from Medtronic, and personal fees from Conmed, outside the submitted work. Dr. Abaza reports receiving grants from Intuitive Surgical and grants from ConMed (Surgiquest), outside the submitted work. All other authors have nothing to disclose.