
Abstract
Purpose:
To evaluate and compare Flexor®Vue™, a semidisposable endoscopic deflection system with disposable ureteral sheath and reusable visualization source, and a nondisposable fiber optic ureteroscope in a standard in vitro setting.
Materials and Methods:
FlexorVue and a reusable fiber optic flexible ureteroscope were each tested in an artificial kidney model. The experimental setup included the visualization of colored pearls and the extraction of calculi with two different extraction devices (NCircle® and NGage®). The procedures were performed by six experienced surgeons. Visualization time, access to calices, successful stone retraction, and time required were recorded. In addition, the surgeons' workload and subjective performance were determined according to the National Aeronautics and Space Administration-task load index (NASA-TLX). We referred to the Likert scale to assess maneuverability, handling, and image quality.
Results:
Nearly all calices (99%) were correctly identified using the reusable scope, indicating full kidney access, whereas 74% of the calices were visualized using FlexorVue, of which 81% were correctly identified. Access to the lower poles of the kidney model was significantly less likely with the disposable device, and time to completion was significantly longer (755 s vs 153 s, p < 0.001). The stone clearance success rate with the disposable device was 23% using the NGage and 13% using the NCircle basket. Overall NASA-TLX scores were significantly higher using FlexorVue. The conventional reusable device also demonstrated superior maneuverability, handling, and image quality.
Conclusions:
FlexorVue offers a semidisposable deflecting endoscopic system allowing basic ureteroscopic and cystoscopic procedures. For its use as an addition or replacement for current reusable scopes, it requires substantial technical improvements.
Introduction
T
For new technical devices to gain acceptance in surgical routine, we need data revealing that their efficacy and image quality are similar to the standard flexible ureteroscopes. However, until now, no clinical or preclinical study has been published evaluating this endoscope. 5 It was this study's aim to evaluate the FlexorVue in a standard experimental setup and compare it to a common nondisposable fiber optic device (BOA vision®; Richard Wolf GmbH, Knittlingen, Germany) using two different extraction devices.
Materials and Methods
Experimental setting
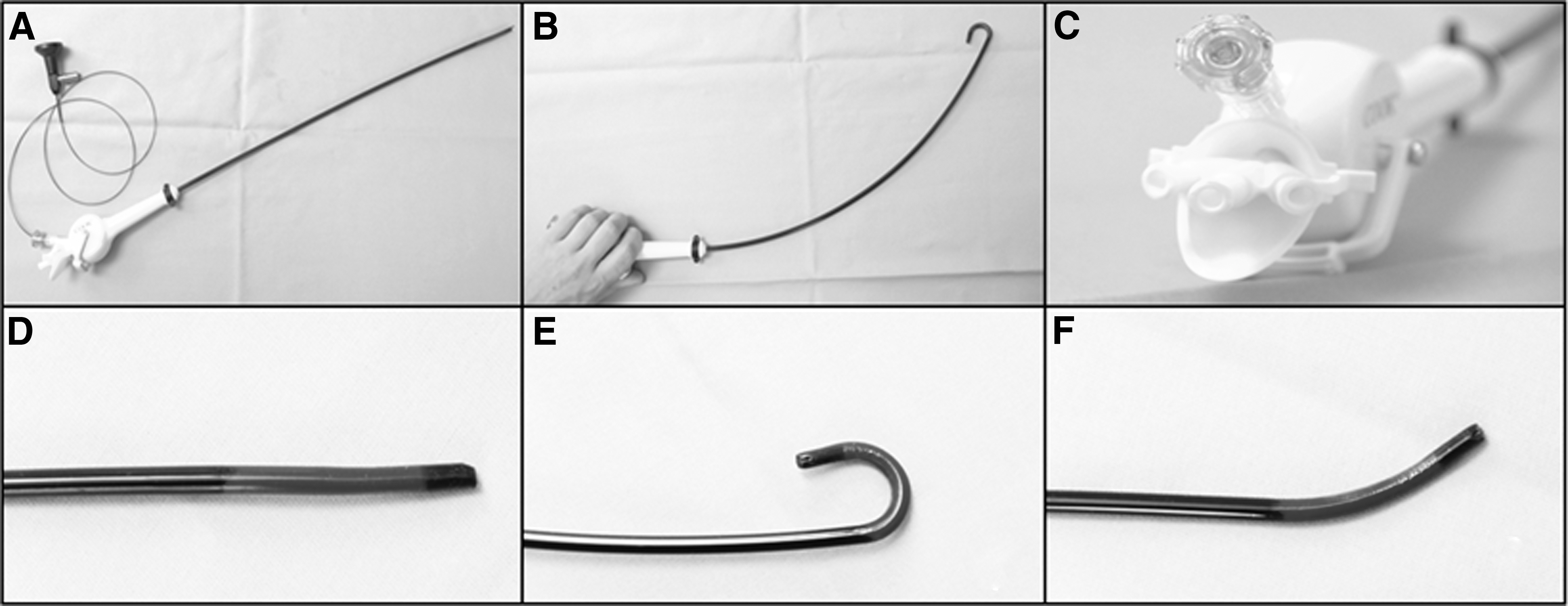
FlexorVue and a conventional fiber optic flexible ureteroscope (BOA vision; Richard Wolf GmbH, Knittlingen, Germany) were each tested in a standardized human kidney model. The devices' technical characteristics are described in Table 1. The experimental setup included two basic tasks: standardized visualization of colored pearls (resembling kidney stones) and secondarily, the extraction of stones (2–3 mm length) with two different stone extractors (NCircle®, NGage®, Cook Medical) as illustrated in Figure 1. The tasks were performed by six surgeons with extensive experience in endourology (two attending, two fellows, and two residents).

One working channel is required for optical fiber.
Shaft includes access sheath.
The kidney models were fixed by a Lone Star® Retractor System 3304G ring to the bottom of a 33 × 68 × 11 cm plastic basin. An opening was created in the basin wall toward the surgeon and coated with a sealing ring. For tasks involving the BOA vision ureteroscope, a 14F/16F 35 cm Flexor urethral access sheath (UAS) was inserted above the basin's opening and inserted in the kidney model's pelvis. Since the FlexorVue has an access sheath, no additional UAS was used for trials involving this device. The technical characteristics of these ureteroscopes are listed in Table 1. All tasks were performed with each ureteroscope once for every kidney model. A new FlexorVue device was used for each task. The surgeons had 15 minutes to complete each task. To avoid a training effect and any influence on the surgeons' perceptions, and to rule out their ability to compare the first instrument or the image seen, the order in which each surgeon was given an ureteroscope was randomly assigned.
Technique
The trial consisted of two basic tasks: visualization and extraction. Once the instruments had been randomly assigned, each surgeon was given time to become familiar with the devices until considered fit for the trial. For the first task, surgeons were asked to navigate through the kidney model and identify the calices by number. A picture of the kidney model with the numbered calices was provided to the surgeon throughout the task. To facilitate correct internal verification, each calix was marked with a different-colored pearl. The color–number association was known only to the trial investigator. To guarantee statistical comparability and standardization, the number of all pearls per kidney was identical. The number of colored pearls in each calix of the four kidneys did not differ. To keep the surgeons from remembering the color patterns, the visualization tasks were carried out at minimum 48-hour intervals. In addition, the surgeons were given no performance feedback during the experiments. Our study parameters were the number of correctly identified calices and the time required. After the surgeon finished the trial task with an instrument, the workload was assessed by the National Aeronautics and Space Administration-task load index (NASA-TLX) scale and a questionnaire on image quality and navigation properties was completed.
For the extraction task, artificial calculi had to be extracted from the kidney models with each instrument using two separate baskets (NCircle and NGage®) in independent trial runs. Single 2–3 mm fragments were placed in each calix. Primary endpoints were the number of stone-free calices achieved and the time required. After completing the trial task with an instrument, the surgeons filled out the NASA-TLX questionnaire and answered questions about image quality and navigation properties.
Statistical analysis
Comparison of all nonparametric endpoints was performed using Mann–Whitney U test and Fishers' exact test for categorical data. All statistical computations were performed using IBM SPSS Statistics (IBM SPSS Statistics for Windows, Version 23.0; IBM Corp., Armonk, NY). A p-value ≤0.05 was considered statistically significant.
Results
Visualization
All calices were accessed within 153 seconds with the standard reusable fURS. Nearly all (99%) were correctly identified, indicating excellent orientation within the kidney model. Seventy-four percent of the calices were accessed with the disposable device; 81% were correctly identified and accessed. Access to the lower poles of the kidney model was significantly less than access to the upper and middle poles (calices 1–6, right model, and calices 1–7, left model). Time to completion was significantly longer (755 seconds vs 153 seconds, p < 0.001). Visualization of the kidney model could not be completed within the allotted 15 minutes in 50% of cases. The devices' handling and maneuverability within the model also revealed significant differences: although participants rated the reusable device's handling as “very good” (mean 1.33) and maneuverability within the kidney model as “good” (mean 1.58) on the Likert scale (1–5), both those factors were rated as “poor” (mean 4.0 and 4.08) in conjunction with the disposable device. Overall, we found that the participants had a significantly higher workload when using the disposable ureteroscope than did those in the reusable group (3.95 vs 18.8; p = 0.01) (Table 2).
NASA-TLX = National Aeronautics and Space Administration-task load index.
Stone extraction
Combining the BoaVision and NGage retrieval basket enabled complete stone clearance in 97% of calices. Using the NCircle basket with the reusable device BoaVision, 96% of stones could be cleared. The success rate with the disposable device was 23% using the NGage and 13% using the NCircle basket. In fact, only 2 out of 72 stones (2.7%) located in the lower poles were retrieved using the FlexorVue. Mean time required per stone retrieval was 73 seconds with the BoaVision and 331 seconds with the FlexorVue using the NGage basket. Time required for stone retrieval with the NCircle was slightly higher in the BoaVision tests (82 seconds), but nearly doubled when using the FlexorVue (653 seconds) compared to the NGage basket. Handling and maneuverability of the BoaVision were both rated “good” when using both baskets (mean 1.83 and 1.92, respectively). In contrast, the performance ratings with the disposable device were significantly lower (p < 0.001) and were assessed as “poor” (mean 4.58 and 4.67). As with the visualization findings, the surgeons experienced the stone extraction task as demanding a much greater workload using the disposable device. The factors “frustration” and “effort” in particular were higher (Table 3).
When breaking down the results for the subjective workload (NASA-TLX), there is a significant difference between fellows and residents (p = 0.031) using the nondisposable devices (attending surgeons vs residents p = 0.067, attending surgeons vs fellows p = 0.94). When analyzing workload for the disposable device, no significant differences could be found.
Discussion
To our knowledge, this is the first in vitro study exploring the characteristics and performance of the disposable fURS device FlexorVue compared to a common reusable scope. Disposable devices for retrograde ureteroscopy have been experiencing a renaissance of late. Although the concept of disposable fURS devices is not new, significant technological improvement, the continuously rising costs of maintaining reusable fURS programs, and growing concerns about inadequate sterilization have prepared the ground for greater attention to this issue. The number of articles published on this subject has risen exponentially from around 16 in the past decade to over 20 just this past year alone. Although several devices from various different manufacturers have been tested and described, all the most recent publications have focused on LithoVue, an entirely disposable endoscope. 6 –9 However, despite comparable performance and expected advantages concerning cost-effectiveness and device sterility, disposable fURS devices are still struggling for their place in the broad armamentarium of endoscopes. Randomized trials will therefore help to explore their real potential in endourology.
Since first described by Bagley in the late 1980s, several disposable URS devices have been developed. 10 From the initially available semidisposable scopes, whereby the body was constructed for single use and the optic fiber was reusable, several stages of technical and mechanical improvement have led to today's digital, entirely disposable fURS devices. When semi-disposable FlexorVue was launched in 2013, it was advertised not as a replacement for the standard reusable ureteroscope in every case, but rather as an opportunity to expand upon procedural capabilities. 11 To compete favorably with modern reusable scopes, the disposable scope's image quality, handling, and maneuverability within the entire collecting system must be at least satisfactory. The results of our series of experiments show that the access to some areas of the kidney, in particular the lower calices, was significantly impaired using the disposable device. Our surgeons were unable to navigate the scope well enough, especially with an inserted basket for stone extraction access to poles where a >90° deflection was required.
According to Bagley et al., a maximum deflection angle of 175° is needed to enable access to all calices in the collecting system. 11 Although the FlexorVue allows a 180° deflection, accurate orientation, visualization, and maneuverability were significantly restricted. The main reason for this is most likely its unidirectional tip deflection. After active tip deflection, passive reflection into the neutral position (0° deflection) is not just incomplete; it remains at different degrees, as much as 45° (Fig. 2).
In addition, tip deflection does not move upward or downward as one would intuitively expect, but rather somewhat twisted to the left or right when the device is held in a neutral working position, requiring the surgeon to reorientate himself or herself after each tip deflection. These circumstances in effect hinder a clear orientation and maneuverability. Hence, these parameters are not only reflected in inferior results in terms of visualization and stone extraction but also proved to be time-consuming and increased the surgeons' workload significantly. The experience level had no significant impact on the success rate for any of the tasks given, regardless of the device used. Interestingly, when looking at the subjective workload (NASA-TLX), there is a significant difference between fellows and residents when using the nondisposable devices. We believe that urologists at the fellow level might have a beneficiary constellation of their already relatively high level of experience in retrograde intrarenal surgery (RIRS) with superior device handling skills and the fastest adaptation to a phantom kidney model. When analyzing workload for the disposable device, no significant differences could be found. Although most other disposable devices require an additional access sheath, FlexorVue with its hydrophilic coating acts as an integrated access sheath resulting in the largest shaft size (15F) and working channel (9F) among the disposable instruments on the market so far. Hence, the single working channel is large enough to recover small stone fragments through the instrument, although permitting good irrigation when using a basket or laser fiber inside. Concerning potential intraoperative or postoperative ureteral complications the instrument's size and diameter must be considered. If we take the device's length into consideration, it is possible that the 48 cm short FlexorVue does not accommodate the entire collecting system, especially in male patients. This may also cause ergonomic problems since the surgeon would have to insert the device up to the hand piece, although having to constantly adjust his hand position on the instrument once it has been inserted. In conclusion, we believe that the disposable fURS device FlexorVue may be useful for simple diagnostic or therapeutic purposes in the upper tract, or for easy to access calices, but may rather suffice as a cystoscope. The FlexorVue deflection characteristics will need to undergo major technical improvements to be able to compete with reusable renal scopes, in particular regarding the lower calices' complete visualization and accessibility. We believe that a better, updated second-generation version of this device could promote the concept of a single-use ureteroscope with an integrated access sheath.
Conclusion
FlexorVue offers a semidisposable deflecting endoscopic system with integrated access sheath allowing basic ureteroscopic and cystoscopic procedures. For routine clinical use as addition or even replacement for current reusable ureteroscopes, further substantial technical improvements are required.
Footnotes
Acknowledgment
External funding: this research trial was funded, in parts, by the Cook Medical Research Programme.
Ethical Standard
The study design was approved by the Institutional Ethics Committee of the University of Freiburg Germany (Project-ID: 24/17) and performed in accordance with the ethical standards defined by the Declaration of Helsinki.
Authors' Contribution
D.S.: data collection, data analysis, article writing, project development, project coordination; S.H.: article editing and project development; M.A.O.: data collection and article editing; Konrad Wilhelm: article editing; A.M.: project development and article editing; M.S.: project coordination/supervision and article writing.
Author Disclosure Statement
No competing financial interests exist.