
Abstract
Objective:
To compare the efficacy and safety of video endoscopic inguinal lymphadenectomy through a hypogastric subcutaneous approach (VEIL-H) with a leg subcutaneous approach (VEIL-L) in the surgical management of penile cancer.
Materials and Methods:
Between October 2012 and October 2016, 72 penile cancer patients who underwent VEIL-H (n = 37) or VEIL-L (n = 35) by one experienced surgeon in our hospital were retrospectively included. Data associated with demographic characteristics and perioperative outcomes were evaluated and compared between two groups.
Results:
No intraoperative complications occurred and no deaths were recorded. No difference was noted with respect to demographic and clinicopathological data, operative time, estimated blood loss, spare of the great saphenous vein, dissected inguinal lymph nodes, patients with inguinal lymph node metastasis, positive inguinal lymph nodes, duration of drain, postoperative hospital days, and postoperative complications between two groups (p > 0.05). Two patients of each group received a bilateral laparoscopic pelvic lymphadenectomy in one session. The pathological results of all dissected pelvic lymph nodes were negative. Median follow-up was 16.2 months, during which time three patients in VEIL-L group and two patients in VEIL-H group developed regional or distant metastases.
Conclusions:
Hypogastric approach is as effective and safe as VEIL-L for penile cancer. Moreover, VEIL-H can avoid the operation on both the limb and abdomen if laparoscopic pelvic lymphadenectomy is required.
Introduction
T
Video endoscopic inguinal lymphadenectomy (VEIL) has been well developed in recent years. In 2003, Bishoff and his colleges were first to report the use of endoscopy for inguinal lymph node dissection in two cadavers and one patient. 8 Since then, several studies have shown that fewer complications and a significantly lower morbidity were observed in endoscopic surgeries than open surgeries. Moreover, it was believed that there was little difference in the counts of dissected inguinal lymph nodes between two surgical procedures. 9,10
Surgeons have two different options of leg subcutaneous approach and hypogastric subcutaneous approach when performing VEIL. VEIL through a leg subcutaneous approach (VEIL-L) is applied to penile cancer patients, which has been reported as a less invasive alternative way to open surgery. 11 In recent years, VEIL through a hypogastric subcutaneous approach (VEIL-H) has been presented, which benefits to conduct a bilateral VEIL through the abdomen rather than both legs in VEIL-L. When a laparoscopic pelvic lymphadenectomy is needed during the operation, a hypogastric subcutaneous approach that avoids port placements on the leg may be ultilized. 12 However, most urological surgeons are more familiar with the surgical technique of VEIL-L and preferred using such an approach.
To date, there are few studies on the experience of VEIL-H in penile cancer patients. It is of vital importance to find its value of VEIL-H for penile cancer. We therefore designed a comparative study on the difference between two approaches for VEIL in penile cancer patients at our hospital to evaluate the efficacy and safety of VEIL-H.
Materials and Methods
Patient selection
The study was approved by the Ethics Committee of Xiangya Hospital, Central South University. Penile cancer patients who underwent VEIL by one experienced surgeon were retrospectively collected in our center between October 2012 and October 2016. All patients before gave their written consent form, and their clinical information was saved in the hospital database. This patient cohort underwent resection of their primary penile tumor with partial or total penectomy. VEIL was performed through a leg subcutaneous approach in penile cancer patients between October 2012 and October 2014. The hypogastric subcutaneous approach has been subsequently applied in November 2014. Patients who were initially diagnosed with primary squamous cell carcinoma of the penis and received a bilateral VEIL without neoadjuvant chemotherapy or radiotherapy were included. Patients were excluded from the study in the following cases: (1) turned to the open surgery during the operation; (2) had a prolonged length of hospital stay because of some unexpected conditions which were not associated with surgical complications; and (3) the length of follow-up was <6 months.
Preoperative preparation
Inspection, including medical history, physical examination, chest X-ray, electrocardiogram, groin ultrasonograph, and laboratory blood tests were included in the preoperative workup of each patient. Patients were required to stop using anticoagulant or antiplatelet agents 2 weeks before the surgery. All patients underwent bowel preparation and received preoperative antibiotic therapy.
Surgical procedure
The VEIL-L procedure was carried out as described previously. 11
VEIL-H procedure: All the patients received the catheterization and general anesthesia during the operation. The patient was positioned in a supine position with slight external rotation of two limbs to provide adequate exposure to the inguinal region and perineum. The low abdomen, groin, and thighs were shaved, prepped, and draped in a sterile manner. The femoral triangle was marked on the skin of both legs. For left inguinal lymphadenectomy, the surgeon stood on the patient's right side, and the assistant stood on the left side. The surgeon and assistant changed places during the procedure to complete the right inguinal lymphadenectomy. A 12-mm incision was made at the level of 2 cm below the umbilicus (Fig. 1). The workspace was created between Scarpa's fascia and the surface of the obliquus externus abdominis muscle with blunt finger dissection and balloon dilation. The workspace is insufflated to a pressure of 12 mm Hg. One 5-mm port was inserted on the left side, whereas one 10-mm port on the right side. Both ports were placed at the lateral side of the rectus abdominis with the level of 2 cm below the first 12-mm port.

Patient positioning and ports placement.
The boundaries of the dissection were superior to the inguinal ligaments, inferior to the apex of the femoral triangle, medial to the adductor longus muscle, and lateral to the sartorius muscle. Dissection was closely along the aponeurosis of the obliquus externus abdominis muscle, beginning from 5 cm onto the anterior abdominal wall above the inguinal ligament. The fibrofatty packet containing the lymph nodes was dissected from the top down using the harmonic scalpel. The inguinal ligament was usually identified in the process of this dissection as being a transverse structure with white fibers (Fig. 2). The dissection proceeded downward to expose the fascia lata and fossa ovalis. Saphenous vein, femoral vein, and femoral artery could be identified within the femoral triangle by the dissection of fascia lata after the exposure of saphenofemoral junction. Inadvertent dissection to the depth of the fascia lata was apparent when reddish muscular fibers were seen. When meticulously separating the great saphenous vein and its branches, including the superficial circumflex, superficial epigastric, superficial external pudendal, superficial lateral, and medial cutaneous (Fig. 3), it was technically possible to preserve these veins as much as possible. The superficial lymph nodes on each side of the vein as well as the deep inguinal nodes (Cloquet's nodes) medial to the femoral vein up to the inguinal ligament were all removed. The femoral vein and artery were skeletonized with all of the tissue between them. The packet was then placed in an endoscopic specimen retrieval bag and withdrawn. Sutures from the inside issues to the skin on both legs were aimed to obliterate the subcutaneous dead space. After the bilateral dissection of inguinal lymph node, the left drain was exited from the 5-mm port on the left abdominal wall while the right drain was exited from the 10-mm port on the right side (Fig. 4). Finally, the port incisions were closed. (see Supplementary Video 1; Supplementary Data are available online at
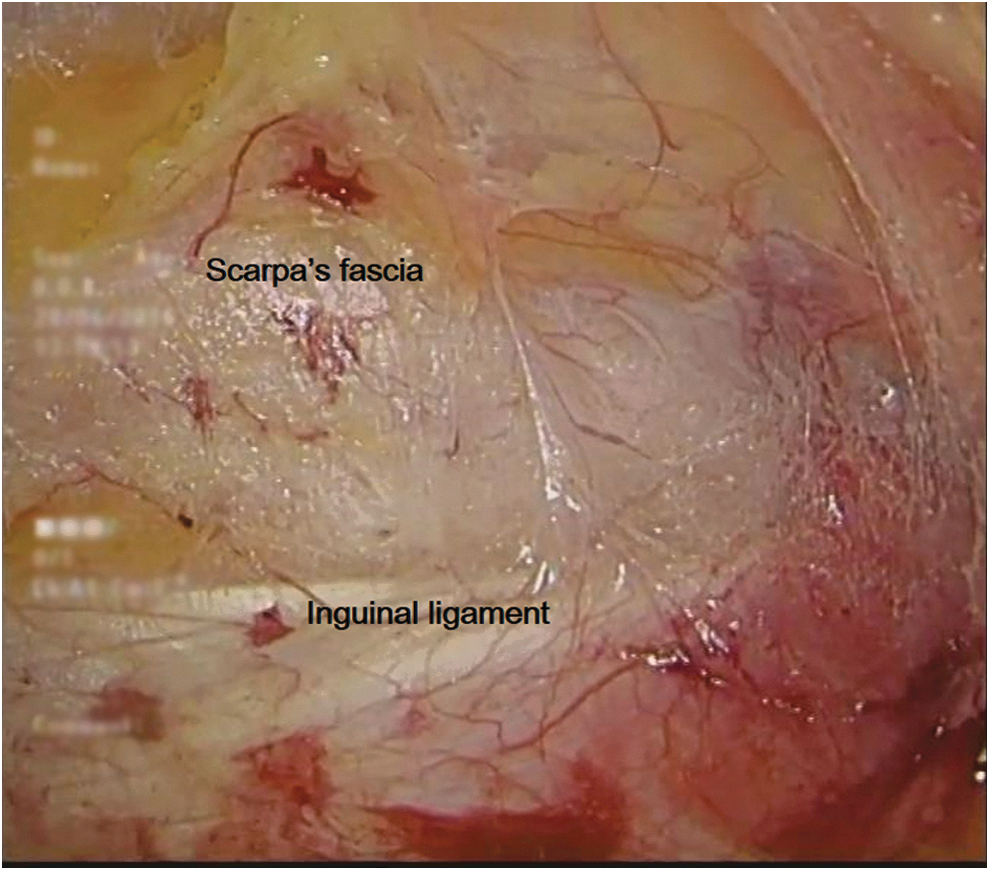
Identification of Scarpa's fascia and inguinal ligament.
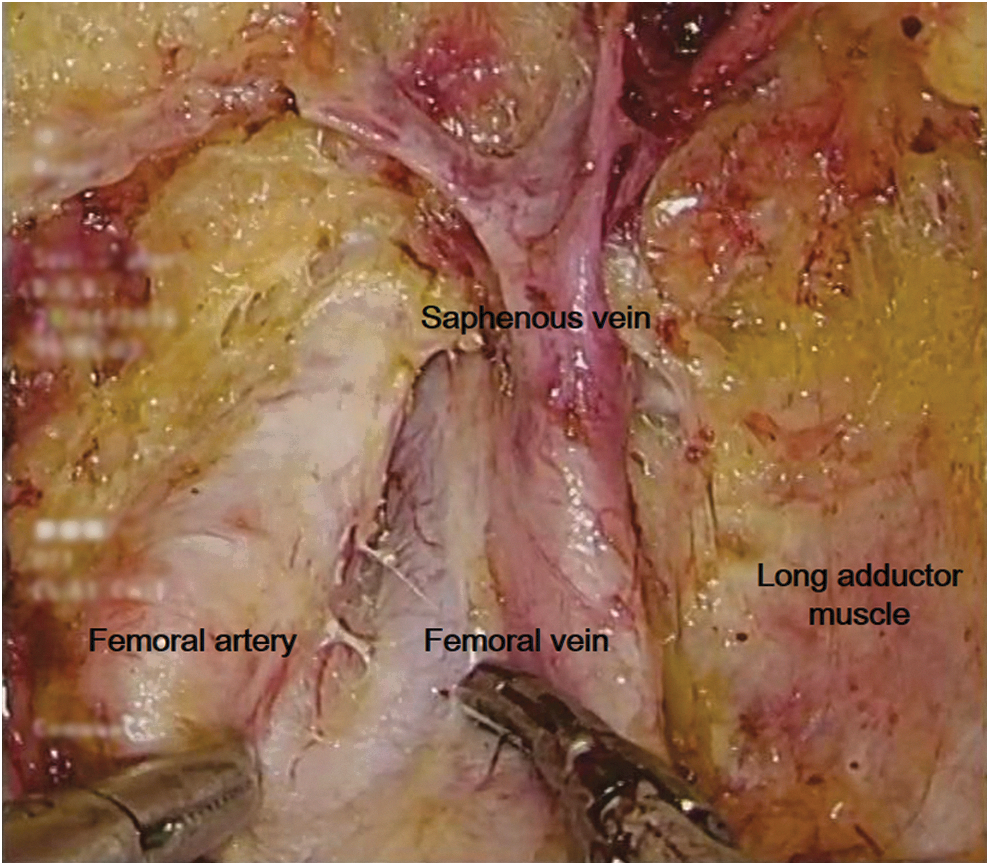
Dissection of the saphenous vein and its branches, removal of the deep inguinal lymph nodes.

Post video endoscopic inguinal lymphadenectomy through a hypogastric subcutaneous approach.
Pelvic lymphadenectomy
When the frozen sections of two or more inguinal lymph nodes were deemed positive for metastasis, a bilateral pelvic lymphadenectomy was performed simultaneously or as a secondary procedure following the definitive histology. 1 The surgeon would have a short talk with the relatives about the results of the quick-frozen pathological examination and then legal relatives decided whether a bilateral pelvic lymphadenectomy was performed simultaneously during the operation. Laparoscopic pelvic lymphadenectomy was performed by initial three ports during the hypogastric procedure. But the new ports in the abdominal wall were established in the leg procedure. The pelvic lymph nodes were dissected as previously described in patients with penile cancer.
Postoperative management
An elastic compression bandage was applied to each leg in all patients. All patients continued to receive preoperative antibiotic therapy. But antibiotics were not routinely continued after discharge from the hospital. The drain stays in place until drainage volume was <50 cc in 24 hours. If the drainage volume was still more than 50 cc on the fifth day, a chyluria test for the liquid was conducted. Patients were diagnosed with lymphorrhea if the test was positive.
Outcome measures
Age, body mass index (BMI), smoking status, positive human papillomavirus (HPV) infection, the American Society of Anesthesiologists (ASA) score, clinical N stage of lymph nodes, pathological T stage of primary tumor (based on 2009 TNM clinical and pathological classification of penile cancer), pathological grade of primary tumor, operative time (defined as the time from the cutting of skin to the closing of port incisions), estimated blood loss, spare of the great saphenous vein, dissected inguinal lymph nodes, patients with inguinal lymph node metastasis, positive inguinal lymph nodes, duration of drain, postoperative hospital days, and complications were collected.
Statistical analysis
SPSS software version 19.0 was used for data analysis. All quantitative values are expressed as the median ± standard deviation, range. Continuous variables were compared by the Student's t-test or Mann–Whitney U test. Comparison of categorical variables was performed by Chi-square test or Fisher's test, as appropriate. All tests were two-sided, and the p value <0.05 was considered statistically significant in all tests.
Results
Demographic and clinicopathological characteristics
There was no significant difference between two groups in age, BMI, smoking status, positive HPV infection, ASA score, clinical N stage of lymph nodes, pathological T stage of the primary tumor, and pathological grade of the primary tumor (p > 0.05) (Table 1).
ASA = American Society of Anesthesiologists; BMI = body mass index; HPV = human papillomavirus; SD = standard deviation; VEIL = video endoscopic inguinal lymphadenectomy; VEIL-H = VEIL through a hypogastric subcutaneous approach; VEIL-L = VEIL through a leg subcutaneous approach.
Outcomes of pelvic lymphadenectomy
All of 72 patients successfully underwent a bilateral VEIL. Five patients in VEIL-L group and seven patients in VEIL-H group had more than two positive inguinal lymph nodes according to the results of the quick-frozen pathological examination. Two patients of each group received an additional bilateral laparoscopic pelvic lymphadenectomy in one session based on both surgeon's considerations and legal relatives' willing. Operative time of two patients in VEIL-L group was 185 and 181 minutes, whereas 165 and 157 minutes in VEIL-H group. The counts of dissected pelvic lymph node of two patients in VEIL-L group were 7 and 10, whereas 8 and 9 in VEIL-H group. No dissected pelvic lymph nodes were positive in these patients.
Perioperative data and pathological results
No serious complications or deaths occurred during the operation in both groups. With regard to operative time, dissected inguinal lymph nodes, estimated blood loss, spare of the great saphenous vein, patients with inguinal lymph node metastasis, positive inguinal lymph nodes, duration of drain, and postoperative hospital days, there was no significant difference between the VEIL-L and VEIL-H groups (p > 0.05) (Table 2).
Postoperative complications
There was no significant difference in the overall incidence of postoperative complications between the two groups (p > 0.05) (Table 3). All 16 patients in two groups with complications (including Clavien–Dindo I, II, and IIIa) had a good relief of the syndromes within the last follow-up visit. No postoperative complications associated with laparoscopic pelvic lymphadenectomy occurred.
The mean follow-up was 16.2 months (range, 6–27 months) during which time three patients in the VEIL-L group and two patients in the VEIL-H group underwent pelvic lymphadenectomy or salvage chemotherapy after regional or distant metastases. There was one death observed in each group, which was disease related.
Discussion
The incidence of penile cancer has been decreasing in China during the recent decades and is not common in malignant disease. However, it still remains a threat to males' health. Before the metastasis to distant sites, there is a long local regional period in penile cancer. Lymph node status is a considerable prognostic indicator of survival in patients with penile cancer. 13,14 Inguinal lymphadenectomy has been demonstrated to be an important part of the management of penile cancer. It has been indicated that inguinal lymphadenectomy should be helpful and curative. 15 Johnson et al. 16 pointed out that the overall survival was improved by the dissection of any number of lymph nodes.
VEIL is promoted and widely used in recent years with the consideration of the high risk of complications and mortality of open inguinal lymphadenectomy. 17,18 Laparoendoscopic single-site (LESS) technique has been applied in the VEIL. 19 But the special single-port platform and surgeons' limited surgical skill restrict the application of LESS technique at many hospitals. Robot-assisted inguinal lymphadenectomy, as a newest minimally invasive procedure, has been applied to both the diagnosis and treatment of penile cancer. More studies on robot-assisted inguinal lymphadenectomy are required to prove the safety and efficacy of this technique. 20,21 Besides, robot-assisted equipment are still unavailable in many medical institutions. VEIL, using either a leg or hypogastric subcutaneous approach has been regularly performed in penile cancer patients in China.
In VEIL-L, three ports were placed on each leg. VEIL-H with four ports in vulvar cancer patients was reported in previous studies. 12,22 We modified and refined the technique for penile cancer with conventional laparoscopic instruments. In our study, we used three ports in VEIL-H, which was practicably feasible to complete the surgery. Compared with VEIL-L, there were several potential advantages in performing VEIL-H. First, placing ports in inferior abdominal walls can serve the bilateral VEIL procedure and avoid port placements on both legs. It is beneficial to reduce the rate of postoperative dysfunction of lower limbs. Second, fewer incisions and port placements may lead to a better aesthetic visualization of the scar. Third, when a laparoscopic pelvic lymphadenectomy is needed during the operation in the hypogastric procedure, it can be directly performed through initial ports in the abdominal wall. In the leg procedure, however, extra work during the operation such as abdominal skin sterilization, change of surgeons' position, and new port placements in the abdominal wall are required, which may potentially prolong the operative time.
Short-term perioperative outcomes were analyzed and compared to investigate the efficacy and safety of VEIL-H. Only 18.92% of patients in VEIL-H group had postoperative complications. Compared with open inguinal lymphadenectomy in the previous study, 5 the incidence of postoperative complications in VEIL-H is much lower and the result of dissected inguinal lymph nodes in VEIL-H is quite satisfying. The mean operative times for VEIL-L and VEIL-H in our cohort were comparable, indicating that the port placement on both limbs resulted in no meaningful change in time. To perform a successful VEIL-H, surgeons should have a good knowledge of the anatomy of the abdomen and inguinal region. Separation and dissection of lymph nodes were based on landmarks such as Scarpa's fascia, inguinal ligament, fascia lata, long adductor muscle, sartorius muscle, fossa ovalis, and saphenofemoral junction, which should be clearly identified by surgeons.
In our studies, clinical and pathological positive lymph node rate differs quite widely (11.43% vs 25.71 in VEIL-L group, 16.22% vs 32.43% in VEIL-H group), and this discrepancy may be reduced by using imaging modalities preoperatively, such as 18 FDG-positron emission tomography/CT, to assess the inguinal and pelvis region. Studies have shown that nodal yield represents the dissection adequacy from an oncologic control standpoint. The mean number of nodes dissected was 19.77 in VEIL-L, which is similar to the mean of 21.05 nodes in VEIL-H. Together with the regional or distant metastases rate, it supports the hypothesis that VEIL-H provides the same oncological control with VEIL-L. All 5 patients in our series who developed metastases had the pN+ disease, and no patient with pN0 disease has developed metastases. Although the precise etiology of this metastasis is uncertain, it is likely related to the pathological status of the lymph nodes.
There were several limitations in our study. A larger sample is needed and longer follow-up time with more regular visits is beneficial for the further investigation in oncologic outcomes and long-term postoperative complications. Furthermore, as the limitation of our study design, potential bias can be caused by the nonrandomized, open-labeled retrospective design. More prospective multicenter, randomized, controlled clinical trials should be performed to study and compare the safety and efficacy of two approaches for VEIL.
Conclusions
The hypogastric subcutaneous approach is as effective and safe as leg subcutaneous approach in VEIL for penile cancer. More convenience can be obtained by VEIL-H if a laparoscopic pelvic lymphadenectomy is needed during the operation. Both inguinal and pelvic lymphadenectomy can be performed through the abdominal access, which avoids operations on two limbs.
Footnotes
Authors' Contributions
P.Y. and L.W. designed the study and wrote the main article text. C.Z., Z.L., Z.O., L.Q., and X.Z. collected the clinical data and performed data analysis. W.H., Y.W., and Y.C. prepared the tables and figures. All authors reviewed and approved the article.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.