
Abstract
Objective:
To evaluate early continence rates with a novel modified vesicourethral anastomosis technique based on prevention of urethral retraction using anastomosis sutures as stay sutures (PURS) during robot-assisted radical prostatectomy.
Materials and Methods:
Sixty patients operated by a single surgeon were enrolled and data collected prospectively. This cohort was compared with another consecutive 60 patients operated with standard anastomosis. The new technique is based on preventing urethral retraction of the posterior urethra with two anastomosis sutures being used as stay sutures. The outcomes were prospectively followed and groups compared regarding early continence. International Consultation on Incontinence Questionnaire Short Form was used to assess incontinence and its impact on the quality of life. Pad use (yes or no pads) was evaluated as a more stringent criterion.
Results:
Preoperative patient characteristics were similar between the two groups. Anastomosis was completed faster in PURS group (15.1 vs 18.5 min, p = 0.05). At postoperative week 1 and month 1, the severity and bother of incontinence were significantly less in the PURS group (12.7 vs 4.1 and 10.1 vs 2.6, p < 0.001). PURS cohort reported significantly superior pad-free rates at both postoperative month 1 (73% vs 35%, p < 0.0001) and month 3 (83% vs 53%, p = 0.0004). On multivariable analysis, younger age and the new anastomosis technique were two independent predictors to improve early continence. Four patients in modified anastomosis group (4/60) and 1 in standard anastomosis group (1/60) necessitated temporary urethral recatheterization because of urinary retention.
Conclusion:
We describe a simple and time-efficient modified urethrovesical anastomosis technique by using anastomosis sutures as stay sutures to prevent perineal retraction of the urethral stump. Our results demonstrated that the technique is an independent factor impacting early recovery of urinary continence. Future randomized controlled studies would be required to further test the reproducibility of this technique.
Introduction
D
Materials and Methods
Patients and preoperative data
Patients with localized prostate cancer, who underwent RARP between the dates October 2015 and March 2016, were enrolled. The study received an institutional review board approval. The novel modified anastomosis technique, which prevents urethral retraction with two stay sutures “PURS” (detailed in the next paragraph), was performed starting from January 2016. Anastomosis was performed in the standard manner (detailed in the next paragraph) in patients who underwent surgery before January 2016. These two cohorts were compared. There were no exclusion criteria regarding patient selection. Surgeries were performed by a single surgeon (A.R.K.) with extensive robotic experience over 1500 cases. Preoperative data recorded included age, serum prostate specific antigen (PSA) level, prostate volume, biopsy Gleason score, body mass index (BMI), American Society of Anesthesiologists (ASA) score, and EAU risk group.
Surgical technique of apical dissection and anastomosis
We do not routinely preserve the puboprostatic ligaments and/or the bladder neck. Maximum effort is shown to preserve a thick and long urethral stump with meticulous dissection using minimal cauterization. The dorsal venous complex (DVC) is secured with two bulldog clamps, as previously described. 11 By this maneuver, the DVC is controlled and later selectively sutured without compromising the external urinary sphincter. Anterior reconstruction is performed by securing the DVC suture to the pubic bone. Subsequent to the DVC control, urethra is divided anteriorly and two 3/0 barbed sutures are placed at the posterior aspect of the urethra at 5 and 7 o'clock positions (outside in), although still intact (Fig. 1). These two sutures are then situated on the ipsilateral pelvic walls on both sides, followed by the transection of the posterior urethra and release of the prostate. Bladder neck is reconstructed, when necessary. A modified single sliding “Rocco stitch” is placed for posterior musculofascial plate reconstruction. 12
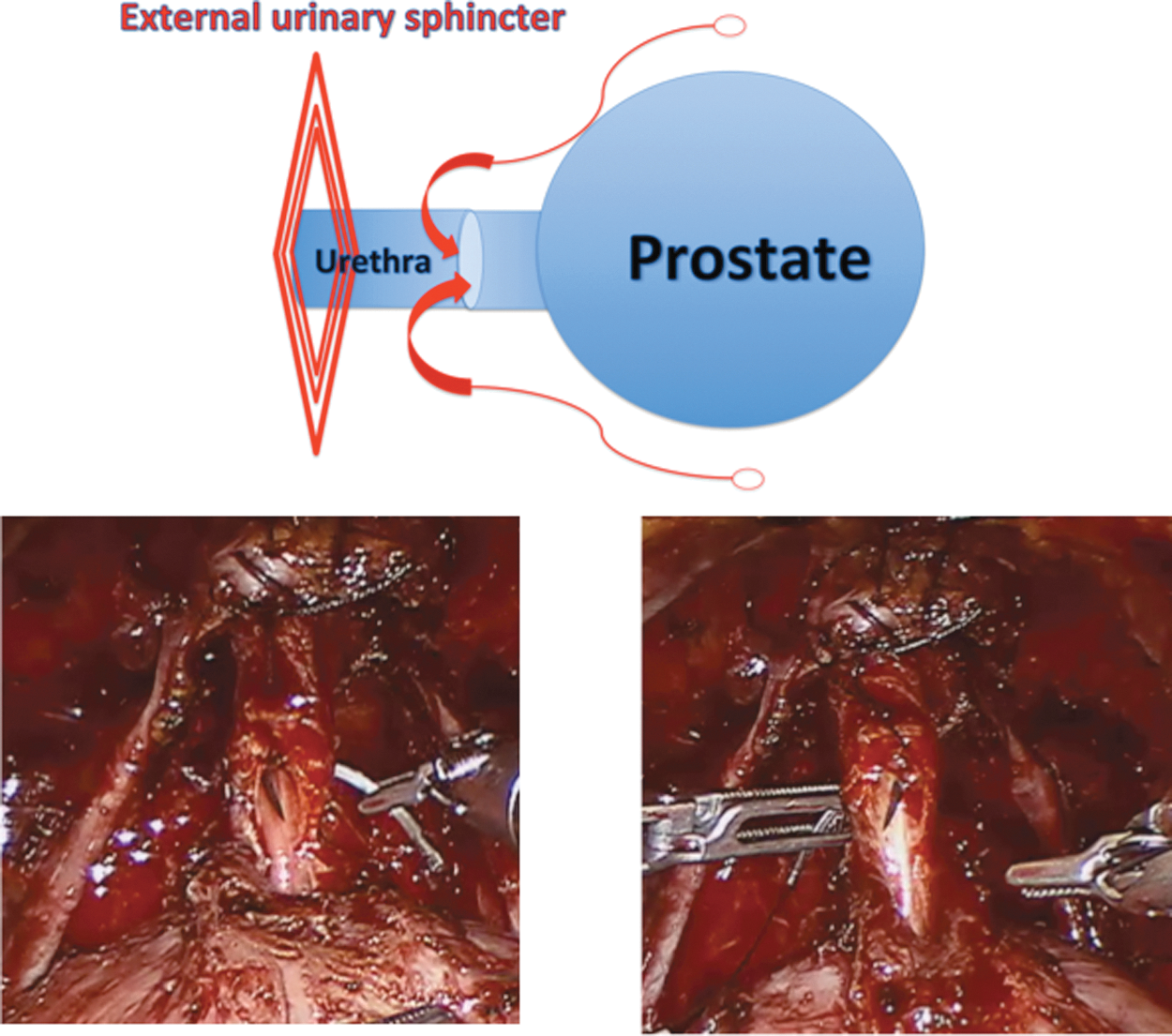
First maneuver of modified anastomosis technique.
In the standard anastomosis, two barbed sutures are used. Suturing initiates posteriorly from 5 and 7 o'clock positions running anteriorly, as described by van Velthoven. 13 In the modified “PURS” technique, urethrovesical anastomosis is performed using the two sutures that served as stay sutures (placed before posterior urethral transection). Initially, needle on the right is passed from the bladder neck inside-out and then from the loop of the suture material, which will later help to expose the urethral stump. The same procedure is repeated for the left side. Using this maneuver, the urethral stump is withdrawn out of the pelvis and the external sphincter complex, allowing it to become prominent. (Fig. 2) Subsequently, the needle is passed again from the bladder neck outside-in and suture pulled upwards. (Fig. 3) These two sutures are then run anteriorly (the right suture clockwise and left suture counterclockwise) in the exact same manner as the standard anastomosis. Bladder is filled with saline and watertight anastomosis is ensured before completion.
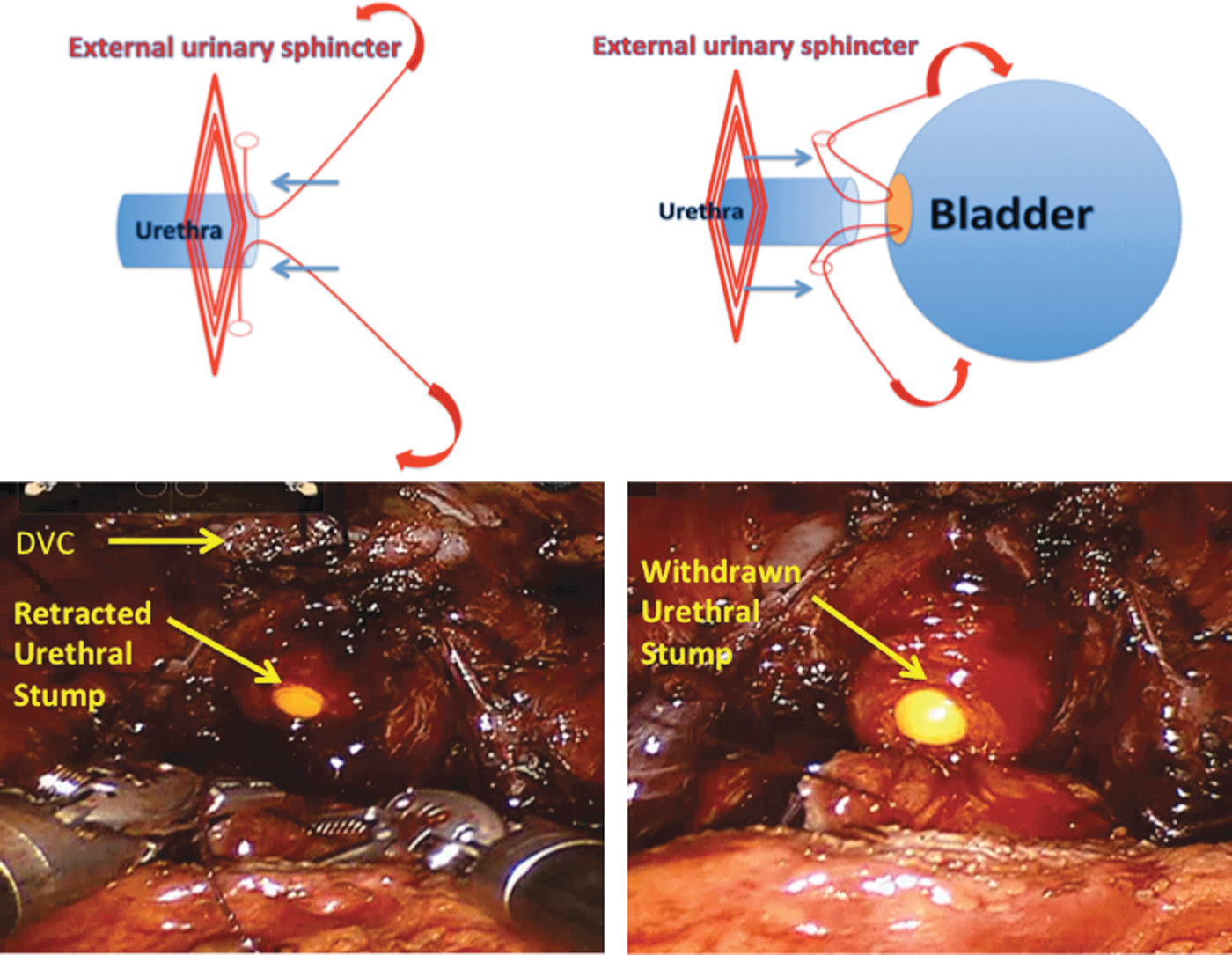
Urethral withdrawn out of pelvic floor and external sphincter complex using PURS technique. PURS = prevention of urethral retraction with stay sutures.
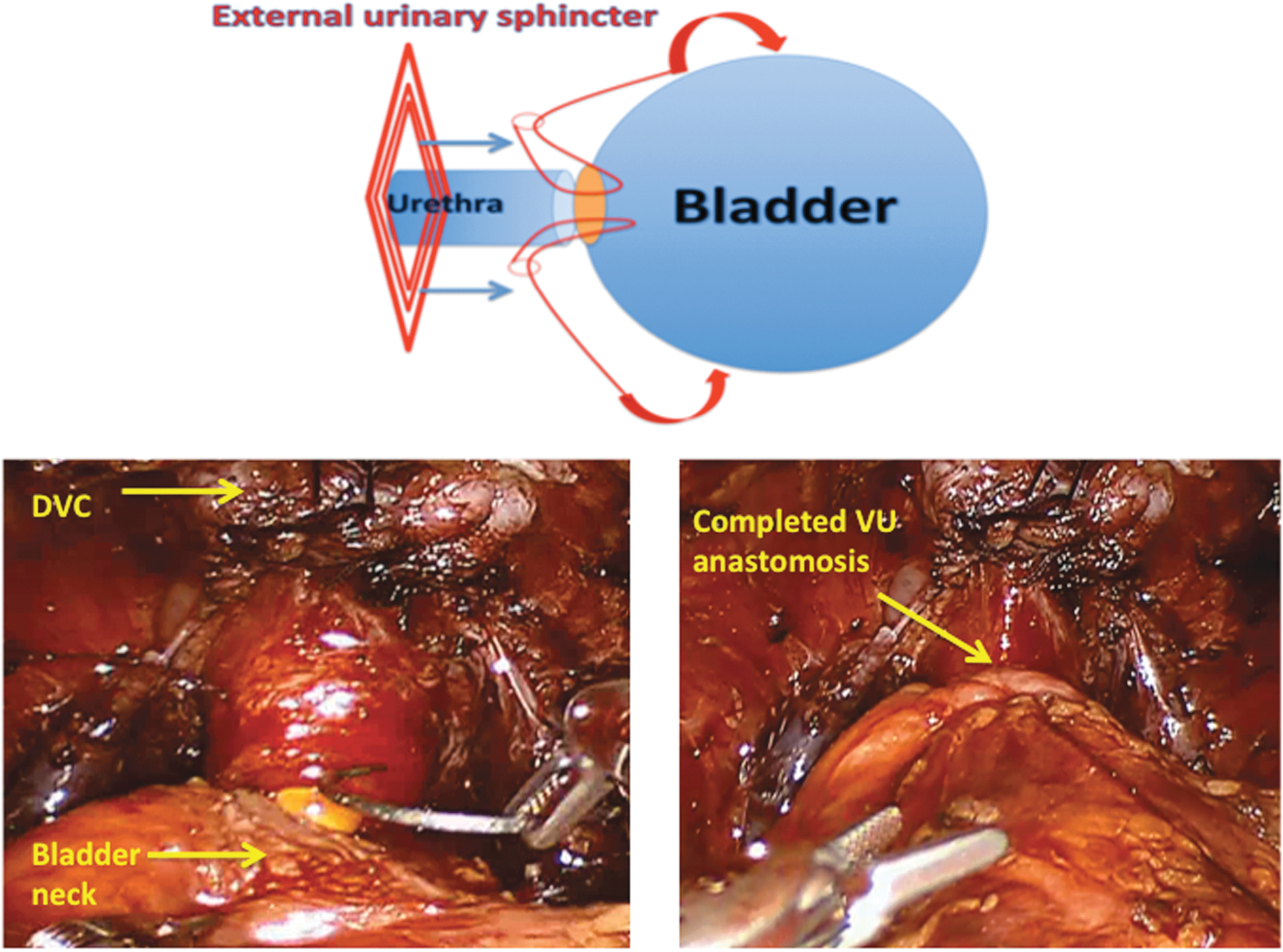
Finalization of the modified anastomosis technique.
Intraoperative and postoperative data and assessment of continence outcome
Intraoperative and postoperative data documented consisted of operative time, estimated blood loss (EBL), duration of anastomosis, surgical margin positivity, nerve sparing status, presence or absence of bladder neck reconstruction, tumor volume of prostatectomy specimen, lymph node dissection status, catheter removal day, and hospitalization period. Complication rates were evaluated using the modified Clavien–Dindo system. 14
Postoperative management protocol: Urethral catheters were routinely removed on day 8 after surgery without cystography. Urine analysis and culture were performed at the first week and first month of catheter removal to rule out urinary tract infection. Each patient was instructed to perform Kegel's exercises starting on day 2 of catheter removal. Pelvic ultrasonography (to rule out lymphocele) and postmicturition residual urine volume measurement were done one month after surgery. The outcomes were prospectively followed and the two groups compared regarding continence rates.
Incontinence evaluation: International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF), previously validated in Turkish, was used to assess the level of incontinence and its impact on the quality of life. 15,16 It was performed at three points in time: (1) before surgery, (2) at first week of catheter removal, and (3) at first month after catheter removal. In the ICIQ-SF short form, the questions addressing stress urinary incontinence were subjected to a subanalysis to demonstrate patients suffering from this specific type of incontinence. Then, the patients suffering from stress urinary incontinence and their ICIQ-SF scores were compared between prevention of urethral retraction with stay sutures (PURS) and the standard technique cohort. Moreover, pad use was evaluated as a more stringent criterion for continence status and was questioned at first and third month of surgery. The response to pad test was either a yes or no. The same urology nurse, blinded to anastomosis type, performed the ICIQ-SF and pad use evaluations.
Statistical analysis
Patient characteristics were tested using Pearson's chi-square test for categorical and the independent samples t-test for continuous variables. All results for continuous variables were expressed as means (range), and the frequencies and proportions were reported as percentages. The recovery of urinary continence was measured with the ICIQ-SF scores using independent univariable/multivariable binary logistic regression models. The following covariates were tested as risk factors (independent variables): age at surgery, BMI, prostatic volume, nerve sparing status (no sparing vs partial vs full) and EAU risk scores (low vs medium vs high), bladder neck reconstruction status, and preoperative PSA. These variables were defined based on the most common factors that have an impact on continence in this literature. All reported p-values were obtained using the two-sided exact method. The statistical significance was set at <0.05.
Results
Data on 120 consecutive patients were analyzed. Preoperative characteristics of the two groups are presented in Table 1. Mean patient age, PSA, prostate volume, BMI, EAU risk groups, operative time, EBL, frequency of bladder neck reconstruction, performance of lymphadenectomy, incidence of positive margins, and details of final pathology (tumor volume, Gleason score, and pathologic stage) were similar between the groups. Anastomosis was completed in a shorter time in the PURS group. (15.1 min vs 18.5 min, p = 0.05).
BMI = body mass index; EAU = European Association of Urology; PSA = prostate-specific antigen; PURS = prevention of urethral retraction with stay sutures.
Preoperative evaluation of the patients revealed that only one patient in the modified anastomosis group was suffering from mild urinary incontinence. ICIQ-SF scores were similar in both cohorts. The mean follow-up period was 20.4 months for the standard anastomosis group and 16.2 months for the modified anastomosis group. Patient-reported adherence to performing Kegel exercises was 100%.
Based on the ICIQ-SF results at first week (mean ICIQ-SF score 4.1 ± 5.73 vs 12.7 ± 4.15) and first month (mean ICIQ-SF score 2.6 ± 4.35 vs 10.1 ± 4.43) after catheter removal, the severity and bother of incontinence were significantly less in the PURS group (Table 2). When the questions designed specifically to evaluate stress incontinence within ICIQ-SF questionnaire were analyzed, the PURS group reported significantly lower stress urinary continence compared to the standard anastomosis group. (p < 0.001). Patients in the PURS cohort reported significantly more pad-free rates at both postoperative month 1 (73% vs 35%, p < 0.0001) and month 3 (83% vs 53%, p = 0.0004) (Table 3).
In univariable analysis, none of the evaluated parameters was found to be an independent predictor for postoperative continence (degree of neurovascular bundle preservation; p = 0.13, bladder neck reconstruction; p = 0.07, lymph node dissection; p = 0.06, and surgical margin positivity; p = 0.67) (Table 4)
In multivariable analysis, two variables independently had an impact on early continence based on pad use results. Undergoing anastomosis with PURS technique and younger age significantly improved gaining continence early. The only independent factor effecting continence status based on ICIQ-SF score was undergoing surgery with the PURS technique. (Table 5)
Only statistically significant parametres (p < 0.05) presented at the table to simplify the view.
OR = odds ratio.
Recatheterization rate was more common in the PURS cohort. One patient (1.6%) in the standard anastomosis and 4 patients (6.6%) in the PURS group required recatheterization (Clavien-Dindo Grade 3a); however, this difference did not reach statistical significance (p = 0.38). Urinary leakage was the underlying reason for recatheterization in two out of four in the PURS group and one in the standard anastomosis group. All patients recovered uneventfully with prolonged catheterization and there was no need for an additional surgical intervention attributable to urinary leakage. There were three patients in each group with positive urine culture and high fever after surgery, and were successfully treated with antibiotics (Table 6). There were no lymphocele development, pelvic hematoma, and rectal injury in both groups.
UTI = urinary tract infection.
Discussion
Urethrovesical anastomosis is an important step of the RARP procedure for achieving satisfactory continence outcomes. The male pelvis and urethral sphincter are highly complex anatomic and functional structures. 17,18 Many efforts have been made to appreciate these structures in more detail and subsequently reconstruct this complex configuration as close to its original as possible. Preservation of the puboprostatic ligaments or alternatively in cases in whom they are divided, performing an anterior reconstruction with securing the DVC suture to the pubic bone has been advocated. Severance of the relatively rigid posterior musculofascial plate by surgery weekens the urethral complex and results in caudal retraction of the urethra. 19,20 The “Rocco Stitch”, well known to robotic surgeons, aims to reconstruct this posterior plate for enhanced urethral coaptation and closure. 12,21 Bladder neck preservation and its impact on continence have long been studied, yet still remain controversial. 22 Recently, more complex posterior reconstruction techniques have been described and proven to improve continence outcomes. 23 Some of these studies incorporated a sling procedure into posterior reconstruction. 23 –26 Careful division of the DVC and preservation of the neurovascular bundle are other critical steps of meticulous apical dissection. 5
The technique described herein may hypothetically exert its effect by two potential mechanisms. By circumventing perineal retraction of the urethra, more precise bites may be taken from the urethral complex during placement of the anastomosis sutures. This could avoid entrapment and thus injury to the striated sphincter while suturing. The precise reapproximation of the urethral complex (mucosa, urethral wall, and surrounding internal sphincter) to its counterpart on the bladder side may translate into faster and superior bridging and recovery of this anatomical structure. The potential of smooth muscle regeneration has been demonstrated in both the gastrointestinal tract and the urinary system. 27,28 In a porcine model, Rehman and colleagues were able to show that after endopyelotomy, the ureter heals with smooth muscle regeneration bridging the defect completely within 3 months. 28 Although there is absence of similar data on the healing process of the internal sphincter after radical prostatectomy, it is tempting to extrapolate the information from the ureter attributable to very similar histology and hypothesize that more precise approximation of the two ends of the anastomosis may facilitate recovery of the smooth muscle of the internal sphincter. Another simple hypothetical explanation for why the PURS approach results in faster and better continence may be allowing for a greater degree of intra-abdominal/pelvic urethra associated with improved coaptation at times of increased intra-abdominal stress.
The pad-free rate at 1 and 3 months in this series was 73% and 83%, respectively. Results from the ICIQ-SF data support the significantly superior results as early as week 1 after catheter removal. Remarkably, these significantly improved results are obtained by a simple modification of using the anastomosis sutures as stay sutures compared to what was performed before. The reason for evaluation of patients' continence status with different tests at altered time periods (ICIQ-SF for the first and pad test for the third month) was to eliminate the potential impact of de novo over active bladder complaints after surgery on the actual stress incontinence status. De novo overactive bladder symptoms tend to occur early after surgery. Thus, we chose to assess the continence status with pad test at a later point in time (third month after surgery in this study design). Validation in native language and enabling a second objective measurement were the primary reasons of using ICIQ-SF questionnaire.
Head-to-head comparisons of results among various series and/or techniques in the literature are quite cumbersome. The assessment tools vary without a standard. Most series using pad as an outcome measure define continence as using 0–1 pads; however, our preference was to use a more strict criterion of 0 pad. Data suggest that there is a significant difference in quality of life in pad-free patients and those using a security pad. 29 Canvasser and colleagues recently published their results on continence with a posterior urethral suspension modification. 23 The pad-free rates were 54% and 60% at weeks 4 and 12 after catheter removal, which are considerably lower compared to the results presented in this study. Porpiglia and colleagues defined total anatomical reconstruction and assessed its implications on early recovery of continence. 30 The authors should be commended for an extremely detailed anatomic reconstruction. Yet, it may take quite an extra time and is not an easy reconstruction, supported by the authors' statement that “they were not over the learning curve after 252 procedures.” Nevertheless, their efforts were rewarded and the continence rates were superb; 89% at week 4 and 94% at week 12 after catheter removal. When we look at our results with standard anastomosis technique, our continence rates at 4th week and 12th week after catheter removal were lower. (35%, 53%) when compared with this recent study. Notably, this study used a different questionnaire and continence definition was zero or one safety pad and thus, a direct comparison with our results could not be made. In our study, pad usage even as a safety pad or any device to control urinary leakage was defined as incontinence. 30
In a meta-analysis of 17 studies, combined anterior and posterior reconstruction techniques were reported to result in a significant advantage in urinary continence recovery 3 months after RARP. 2
Using ICQ-SF allows for a more objective means to assess incontinence and stands out as one of the strong aspects of this series. This was a single and experienced surgeon series with the advantage of eliminating the surgeon factor, which has shown to be a major factor on continence rates. On the other hand, it raises the question whether these results are reproducible. Prospective randomized trials from further centers would be required to validate the results.
Conclusions
We describe a simple and time-efficient modified urethrovesical anastomosis technique by using anastomosis sutures as stay sutures to prevent perineal retraction of the urethral stump during robotic radical prostatectomy. Our results demonstrated that the technique (PURS) is an independent factor impacting early recovery of urinary continence. Future randomized controlled studies would be required to further test the reproducibility of this technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.