
Abstract
Introduction:
We provide primary patency rate of metallic ureteral stents in cancer patients and investigate the factors affecting primary patency.
Methods:
All cancer patients who had received metallic stents for malignant ureteral obstruction between July 2009 and November 2012 in our institute were included. No patients were excluded. Patient profiles, imaging studies, and laboratory data were collected. Patient profiles included age, gender, body height, body weight, body mass index, cancer types, treatment for cancer, response to cancer treatment, methods of stent insertion, and prior ordinary stents. Imaging studies included renal ultrasonography, antegrade pyelography, CT, and MRI. Laboratory data included urinalysis, urine culture, and serum creatinine. Complications were defined according to the Clavien–Dindo classification. Primary patency was defined as a complete resolution or downgrading of hydronephrosis shown by imaging studies or success in the removal of a preexisting nephrostomy tube; otherwise the procedure was considered a primary failure. The primary endpoint was the primary patency rate of the stents. The secondary endpoints were risk factors for primary stent failure.
Results:
A total of 124 stents were inserted into 96 patients with malignant ureteral obstruction. There were no grade 3/4 complications. The overall primary patency rate was 87.9% (109/124). In univariate analysis, antegrade insertion (OR = 24.15, p-value = 0.0086) and urinary tract cancer (OR = 4.18, p-value = 0.0164) were significantly associated with primary failure. Those with prior ordinary stents (OR = 0.20, p-value = 0.0158) or response to cancer treatment (OR = 0.25, p-value = 0.0228) were associated with stent patency. In multivariate analysis, antegrade insertion (OR = 22.04, p-value = 0.0041) and response to cancer treatment (OR = 0.15, p-value = 0.01081) remained significant factors.
Conclusions:
In this large cohort of cancer patients requiring urinary diversion to preserve renal function, several factors were associated with the success rate of metallic stents.
Introduction
Malignant ureteral obstruction often results from the compression of intra-abdominal cancers. Although the obstruction caused by primary cancers may be relieved after surgical treatment, obstruction caused by recurrent or metastatic cancers often requires permanent drainage. To relieve such obstruction, internal drainage with ureteral stents is usually the first-line management. However, the patency rate of ordinary stents is low. 1,2 As the life expectancy is generally shorter than 1 year in patients with advanced cancer causing ureteral obstruction, 3 it is important to maintain kidney function as well as quality of life. Ureteral stents of different materials were invented aiming to achieve better drainage. Permanent metal stents in a form of segmental mesh provide short-term patency, 4 but long-term patency was compromised by restenosis. 5,6
A unique design of ureteral stent is the Resonance metallic ureteral stent (Cook Medical, Bloomington, IN). Made of a continuous unfenestrated coil of nonmagnetic nickel–cobalt–chromium–molybdenum alloy, the full-length stent allows a 1-year indwelling time, according to the manufacturer. The stents have a fixed diameter of 6F with different lengths (20–30 cm) available. The positioning of the full-length stent is the same as with conventional stents: the upper end is placed in the renal pelvis and the lower end in the urinary bladder (Fig. 1).

Plain X-ray showing a more radio-opaque resonance metallic stent in the right ureter and a conventional polymeric stent in the left ureter.
Since the first use of a Resonance stent in 2006 in a 64-year-old woman with metastatic breast cancer, 7 several studies have reported their experience with patients of either benign or malignant diseases. 8 –20 Ten of these studies have included patients with malignant ureteral obstructions, 8 –17 and four of them have analyzed the risk factors of stent failure. However, these were small cohorts with up to 17 antegrade stents in 27 cancer patients at most, and none have clearly defined the primary patency rate of Resonance stents. Thus, the purpose of this study is to provide primary patency rate of the Resonance stents in cancer patients and to investigate the factors affecting primary patency.
Materials and Methods
Ethics statement
The research meets all applicable standards for the ethics of experimentation and research integrity. The local institutional review board (IRB) approved this retrospective study and waived the informed consent requirement. The IRB case number was 201208052RIC.
In our hospital, the retrograde method of stent insertion is performed under general anesthesia by urologists. Initially, an introduction set similar to an 8F/10F dilator is passed over a guidewire into the renal pelvis. The wire and inner catheter are removed, and the Resonance stent is passed through the 10F introducer sheath. The inner catheter is then used to push the stent proximally until the pigtail is placed in the renal pelvis. Finally, the 10F sheath is retracted with the inner catheter held in place until the distal pigtail is deployed in the bladder. The whole procedure is performed under fluoroscopy. The technique is similar to the antegrade method, only that a percutaneous nephrostomy (PCN) must be created before the insertion of a guidewire, and the antegrade procedures are performed under local anesthesia by radiologists. Renal ultrasonography or antegrade pyelography is performed within 1 day after stent placement. Before attempts of PCN removal, PCNs are clamped for 1 day, and the patients are observed for flank pain, urine leak from wound, or signs of urinary tract infection (UTI). Urinalysis, urine culture, serum creatinine, and renal ultrasonography are performed monthly to evaluate stent patency. CT or MRI is performed at least trimonthly to evaluate cancer status. Patients were followed until death.
All cancer patients who received Resonance stents for ureteral obstruction between July 2009 and November 2012 were included. No patients were excluded. Bilateral ureters in the same patient were counted as separate ureteral units. Patient profiles, imaging studies, and laboratory data were collected. Patient profiles included age, gender, body height, body weight, body mass index (BMI), cancer types, treatment for cancer, response to cancer treatment according to RECIST 1.1, methods of stent insertion, and prior ordinary stents. Imaging studies including renal ultrasonography, antegrade pyelography, CT, and MRI were used to determine the degree of hydronephrosis (Grades 0–4) using the Society for Fetal Urology hydronephrosis grading system. 21 Tumor size was measured from CT or MRI. Laboratory data included urinalysis, urine culture, and serum creatinine. Stent-related urinary symptoms were recorded in electronical medical records. A UTI was defined as a positive culture with urinary symptoms. Complications were defined according to the Clavien–Dindo classification of surgical complications. 22
The primary outcome measure was the primary patency rate of the stents. Primary patency was defined as a complete resolution or downgrading of hydronephrosis shown by imaging studies (Fig. 2) or success in the removal of a preexisting nephrostomy tube (PCN); otherwise the procedure was considered a primary failure. Secondary outcome measures included factors that might result in the difference of stent duration. The factors included age, gender, preoperative serum creatinine, method of insertion (antegrade vs retrograde), prior ordinary stents, cancer types including gynecologic (GYN), upper gastrointestinal, lower gastrointestinal, urinary tract, and others (Table 1), degree of hydronephrosis, tumor ≥3 cm (indicating any solid lesion that measured 3 cm or more with ureteral compression, including intra-abdominal recurrence, metastasis, or lymphadenopathy), previous treatment for underlying cancer, and response to cancer treatment (partial response (PR); stable disease (SD); progressive disease; no treatment). Generalized linear model was used to calculate odds ratio and p-value for each factor. Statistical analyses were performed using free software (R® version 3.0.1). All statistical tests were two-tailed, with p < 0.05 indicating significance.

Antegrade pyelography revealing ureteral obstruction and a torturous proximal ureter
Number of Patients and Ureteral Units According to Type of Malignancy
GYN = gynecologic; LGI = lower gastrointestinal; UGI = upper gastrointestinal.
Results
From July 2009 to November 2012, 96 cancer patients with malignant ureteral obstruction received Resonance stents in our hospital. The male-to-female ratio was 31:65. The mean ± standard deviation of age was 60.1 ± 12.4 years old (range: 32–88 years old). The mean ± standard deviation of body height was 158.4 ± 7.6 cm (range: 130–174.2 cm), and the mean ± standard deviation of body weight was 55.8 ± 14.7 kg (range: 35.8–115.4 kg). The mean ± standard deviation of BMI was 22.2 ± 5.1 kg/m2 (range: 13.4–42.2 kg/m2). Cervical cancer was the most frequent type of malignancy (19 patients), followed by colorectal cancer (13 patients) and gastric cancer (12 patients) (Table 1).
A total of 124 stents were inserted into 96 patients because there were 28 patients having bilateral stents. Primary stent failure occurred in 15 out of the 124 stents. The overall primary patency rate was 87.9% (109/124). Of the 15 failures, 3 of them were marked by progressive hydronephrosis, 4 by nonpatency on antegrade pyelography (Fig. 3A), and the other 8 by severe pain or persistent leaking from the PCN after clamping their PCN. Stent-related symptoms were reported, including nine patients with hematuria, eight with dysuria, six with fever, five with urinary frequency, and three with flank pain. Bacteriuria occurred in 44 stents in 34 patients. Symptomatic UTI occurred in 35 stents in 28 patients. Sepsis was noted in three patients. These were managed conservatively. There were no grade 3/4 complications.
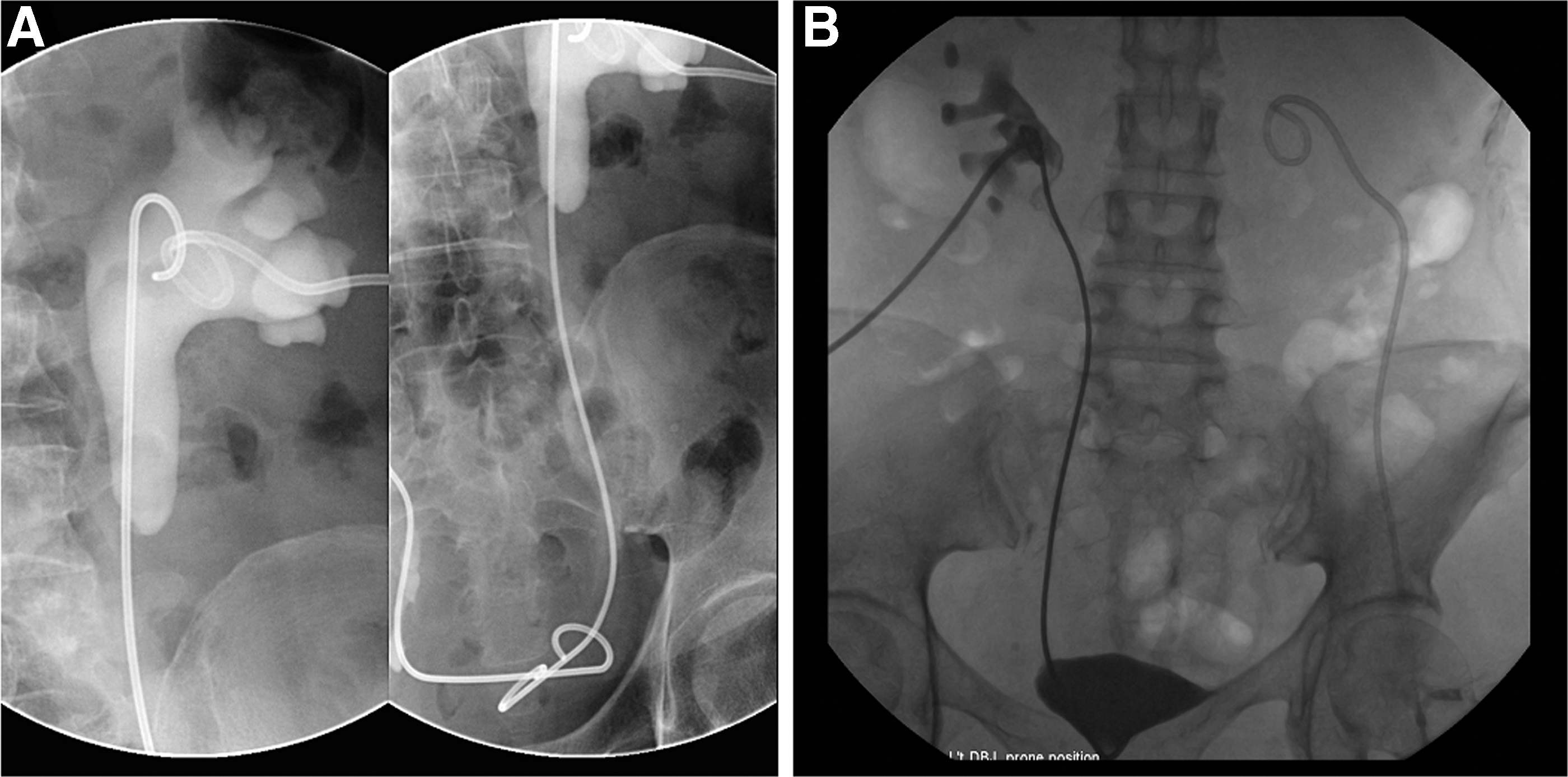
Antegrade pyelography showing accumulation of contrast medium in the renal collecting system with no contrast medium passing into the urinary bladder, indicating a primary stent failure
In univariate analysis, antegrade insertion (OR = 24.15, p-value = 0.0086) and urinary tract cancer (OR = 4.18, p-value = 0.0164) were significantly associated with primary failure. Prior ordinary stent was associated with primary patency (OR = 0.20, p-value = 0.0158). Those with prior treatment for underlying intra-abdominal cancer (OR = 0.12, p-value = 0.0018) were associated with primary patency. Specifically, previous operation (OR = 0.15, p-value = 0.0013) and previous chemotherapy (OR = 0.29, p-value = 0.0271) were both associated with primary patency, but previous radiotherapy was not. Response to cancer treatment (PR/SD) was associated with primary patency (OR = 0.25, p-value = 0.0228). Age, gender, preoperative serum creatinine, degree of hydronephrosis, and tumor size ≥3 cm were not related to primary stent failure (Table 2). In multivariate analysis, antegrade insertion (OR = 22.04, p-value = 0.0041) remained significant for primary failure, and PR/SD (OR = 0.15, p-value = 0.01081) remained significant for primary patency (Table 3). The number of primary stents and patency rates for each stent group are shown in Table 4.
Univariate Analysis of Factors for Primary Stent Failure
CI = confidence interval; PR = partial response; SD = stable disease.
indicates p < 0.05, **indicates p < 0.01.
Multivariate Analysis of Factors for Immediate Stent Failure
indicates p < 0.05, **indicates p < 0.01.
Crude Patency Rates of Stents in Different Patient Groups
NT = no treatment; PD = progressive disease.
Discussion
In our study of 124 Resonance stents in 96 patients with malignant ureteral obstruction, the Resonance stents offered a primary patency rate of 87.9%. Our study showed that antegrade insertion and urinary tract cancer are associated with primary stent failure, and prior ordinary stent, previous operation, chemotherapy, and PR/SD cancers are associated with primary patency. Antegrade insertion (OR = 22.04, p-value = 0.0041) and PR/SD (OR = 0.15, p-value = 0.01081) remained significant in multivariate analysis.
The design of the Resonance stent aimed to sustain stronger extrinsic compressions. In 2006, Borin et al. presented the first use of the Resonance stent: a breast cancer patient with metastasis causing retroperitoneal fibrosis, and the stent lasted 4 months. 7 In other series with up to 27 patients, the overall patency rate was around 80% (ranged from 65%–100%) during a follow-up time of 5.7 to 11 months, 8 –14 and there were no major complications. The efficacy and safety of the Resonance stent is well recognized.
Four studies assessed the risk factors associated with the failure of Resonance stents, and the results were conflicting. Among all possible risk factors, radiotherapy was the most frequently explored. In a cohort of 20 cancer patients, Li and colleagues indicated that prior radiotherapy was significant for stent failure. 12 Wang and colleagues had a similar observation in a cohort of 19 patients with both malignant and benign diseases. 13 On the contrary, by analyzing 25 patients with malignant ureteral obstruction, Goldsmith et al. found that radiotherapy was not a risk for stent failure. 14 Nagele and colleagues also found radiotherapy to be insignificant in their cohort of 10 cancer patients. 9 In our study, we did not find radiotherapy as a factor for primary stent failure. Alternatively, our result showed that response to cancer treatment was associated with stent patency, indicating that disease status might be an important factor in addition to the treatments received.
Our study found urinary tract cancer to be significantly related to stent failure. Of note, there are no renal or ureteral cancers in our cohort because affected kidneys are typically removed, requiring no further drainage. Besides urinary tract cancer, other types of the underlying cancer might also influence stent outcome. Li et al. indicated that GYN cancer was associated with stent failure, 12 but there were no urinary tract cancer patients in their cohort. Possible explanation for these findings is that urinary tract or GYN cancers are more likely to form large pelvic mass and are more likely to invade urinary bladder. These tumor behaviors had been found to be possible factors, 8,14 and these findings might explain why urinary tract or GYN cancers tend to cause more stent failure. Another possible reason for higher failure rate in urinary tract cancers might result from intraluminal obstruction, which was not the designed target of Resonance stents. Among the 21 stents for urinary tract cancer, there were 7 stents with intraluminal obstruction (5 stents in 4 bladder cancer patients and 2 stents in 1 prostate cancer patient). Three of the stents (two stents in the prostate cancer and one in bladder cancer) had primary failure. In the 14 stents without intraluminal obstruction, there were 3 stents (1 stent in bladder cancer and 2 stents in prostate cancer) with primary failure. The OR of intraluminal obstruction for primary stents failure in urinary tract cancer was 2.75 (p = 0.3055). Intraluminal obstruction might play a role in the primary stent failure in urinary tract cancer. However, our number of cases was underpowered to show a difference.
Our study demonstrates higher failure rate in antegrade stents. In one previous series, more antegrade stents were found in the reocclusion group, 13 but this finding was not statistically significant. Previous studies did not show a similar finding probably because of their limited number of antegrade stents (17 stents at most). However, there might be some bias in our result. First, antegrade stents were probably technically more difficult stents, resulting from torturous ureter, severe compression by tumor bulk, or even invisible ureteral orifice by cystoscopy. Second, it might be easier to detect stent failure in antegrade stents. With the preplaced PCNs during the antegrade procedure, antegrade pyelography was always available for patients receiving antegrade stents, but patients receiving retrograde procedures did not necessarily have PCNs for antegrade pyelography. Among the 70 retrograde stents, 5 had pre-existing PCN and received antegrade pyelography before PCN removal. The other 65 retrograde stents had no antegrade pyelography. For the 54 antegrade stents, antegrade pyelography was done at the time of stent insertion. PCN was removed the next day, but antegrade pyelography was not repeated at the time of PCN removal. The mentioned reason might result in both selection bias and detection bias in our result. Hence, the large difference in patency rates between antegrade and retrograde stents (74.1% vs 98.6%) in our study probably reflects the severity of ureteral obstruction, which might be the ultimate determinant of primary patency.
In our study of the 124 Resonance stents, 60 of them were the first ureteral stents for their patients. The remaining 64 stents were replacements for prior ordinary stents. Prior ordinary stent was associated with primary patency of Resonance stents in univariate analysis (OR = 0.1967, p = 0.0158). This association might reflect that more challenging cases were offered Resonance stents up-front, leading to higher failure rate.
The severity of ureteral obstruction is probably the most important factor for stent patency and duration. However, there is no standard measurement in the clinical setting and no consensus on the surrogates in the trial setting. The degree of hydronephrosis certainly does not equal the severity of ureteral obstruction. However, it can be easily assessed by different image modalities, and it correlates well with disease progression in same individuals. Until now, it is still the most widely used parameter for ureteral obstruction across different studies. One way to estimate the ureteral resistance is by applying Ohm's law (ΔP = QR, in which ΔP is pressure gradient, Q is flow rate, and R is ureteral resistance) in the Whitaker test. By infusion into the PCN under a constant flow rate, one can measure the pressure gradient between renal pelvis and urinary bladder with urodynamic instruments, thus the ureteral resistance can be calculated. Whitaker test is historically used for distinguishing nonobstructive hydronephrosis from obstructive hydronephrosis, and has been largely replaced with diuretic nephrogram. Although we did not perform Whitaker test in our study cohort, it could be a useful tool in determining the ureteral resistance in prospective trials. Another way to calculate ureteral resistance is by referring to the Poiseuille's law of vascular resistance: R = 8ηl/πr4, in which R is vascular resistance, η is fluid viscosity, l is the length of vessel, and r is the radius of the lumen. Assuming urine has a constant viscosity, the resistance of ureteral stenosis is determined by the length and the radius of the stenotic site. However, cross-sectional image with ultrahigh resolution is required before this method can be used in real practice.
The first metallic stent used in the ureter was the Wallstent (Boston Scientific). The stainless steel mesh wire formation results in hyperplasia of the urothelium and thus frequent occlusion. The largest series with 40 cancer patients reported a 49% reintervention rate. 23 There are other types of metallic ureteral stents designed for long-term ureteral obstructions. The Memokath stent (PNN Medical, Denmark) is a thermoexpandable segmental mesh stent with nickel–titanium shape memory. First reported by Kulkarni and Bellamy in 2001, 24 the Memokath stent is widely used for both benign and malignant ureteral obstructions. In the largest series consisting of 73 patients, the average indwelling time of an individual Memokath was 11.2 months. 25 Uventa (Taewoong Medical, South Korea), another mesh metallic stent, was first reported in 2012. 26 In its largest series of 71 ureters in 54 patients, Uventa demonstrated a 64.8% primary patency rate. 27 In a small retrospective series (n = 27) comparing Uventa and Memokath stents, Uventa demonstrated a higher clinical success rate than Memokath (82.4% vs 42.9%; p = 0.031). 28 However, frequent major complications were noted in a long-term series of Uventa, including ureteroarterial fistula (three cases, 6.0%), ureteroenteric fistula (three, 6.0%), ureterovaginal fistula (one, 2.0%), ureter perforation (one, 2.0%), and uncontrollable bleeding (one, 2.0%). 29 The Allium ureteral stent (Allium Medical, Israel) is the latest mesh stent made of alloy of nickel and titanium. In a series of 92 patients with mixed etiology, only one stent was obstructed during a mean follow-up of 27 months. 30 The efficacy of Allium stent seems promising, but data from other series are lacking. There is currently no study comparing full-length and segmental metallic stents.
Compared with other studies, our study has several advantages: a large number of patients receiving Resonance stents, a large number of antegrade stents, a homogeneous cohort consisting of only cancer patients, and a multivariate regression model to control confounding factors. However, our study does have some limitations. First of all, this is a retrospective study with its intrinsic bias. Second, without the use of diuretic renography, which is largely limited by the local health reimbursement system, split renal function could not be accurately evaluated. Third, other than the degree of hydronephrosis and tumor size, we do not have additional assessment for ureteral obstruction available. Finally, data are insufficient for cost and quality-of-life analyses.
Conclusion
In this large cohort of cancer patients requiring urinary diversion to preserve renal function, several factors were associated with the success rate of the Resonance stent.
Footnotes
Author Disclosure Statement
No competing financial interests exist.