
Abstract
Purpose:
Nephrolithiasis is an increasingly common ailment in the United States. Ureteroscopic management has supplanted shockwave lithotripsy as the most common treatment of upper tract stone disease. Ureteral stricture is a rare but serious complication of stone disease and its management. The impact of new technologies and more widespread ureteroscopic management on stricture rates is unknown. We describe our experience in managing strictures incurred following ureteroscopy for upper tract stone disease.
Materials and Methods:
Records for patients managed at four tertiary care centers between December 2006 and October 2015 with the diagnosis of ureteral stricture following ureteroscopy for upper tract stone disease were retrospectively reviewed. Study outcomes included number and type (endoscopic, reconstructive, or nephrectomy) of procedures required to manage stricture.
Results:
Thirty-eight patients with 40 ureteral strictures following URS for upper tract stone disease were identified. Thirty-five percent of patients had hydronephrosis or known stone impaction at the time of initial URS, and 20% of cases had known ureteral perforation at the time of initial URS. After stricture diagnosis, the mean number of procedures requiring sedation or general anesthesia performed for stricture management was 3.3 ± 1.8 (range 1–10). Eleven strictures (27.5%) were successfully managed with endoscopic techniques alone, 37.5% underwent reconstruction, 10% had a chronic stent/nephrostomy, and 10 (25%) required nephrectomy.
Conclusions:
The surgical morbidity of ureteral strictures incurred following ureteroscopy for stone disease can be severe, with a low success rate of endoscopic management and a high procedural burden that may lead to nephrectomy. Further studies that assess specific technical risk factors for ureteral stricture following URS are needed.
Introduction
N
As the surgical management of upper tract stone disease has transitioned from primarily noninvasive (SWL) to primarily invasive (URS) techniques, evaluating the morbidity and complications of URS remains critical. New URS techniques and technologies, including ureteral access sheaths (UAS), improved baskets, digital ureteroscopes, and changes in practice patterns, such as staged URS for large renal stones, continue to advance the specialty of endourology. 5 Ureteral stricture is believed to be a rare (<1%–4%) complication, with known risk factors, including ureteral perforation and stone impaction. 6 –8 Prior series have suggested a synergistic increase in risk of ureteral stricture with stone impaction and perforation, but other precise technical risk factors remain unclear. 9 –11
The goal of minimally invasive surgery is to maximize effectiveness of treatment while minimizing the morbidity and invasiveness of the procedure. Complications should thus be both rare and mild. Development of a ureteral stricture following URS can be a very morbid complication, as it leads to additional testing, procedures, and the possibility of major reconstruction or nephrectomy. As URS technologies evolve and the number of URS performed increases, awareness of the severity of complications and discussion of methods of preventing complications is critical. We describe the morbidity of ureteral strictures incurred following URS for upper tract stone disease.
Patients and Methods
Study protocols were approved by the Institutional Review Board (IRB) at each institution. Records for patients referred to and managed at four tertiary care centers that participate in the Western Endourology Stone (WEST) research consortium, with the diagnosis of ureteral stricture following URS for upper tract stone disease, were retrospectively reviewed. Excluded were strictures developed following percutaneous nephrolithotomy with or without antegrade URS, radiation, or other nonstone-related etiologies, including endometriosis, retroperitoneal fibrosis, and psoas abscess. All patients were initially evaluated between December 2006 and October 2015.
Ureteral stricture was defined as having at least one of the following: presence of hydronephrosis (Fig. 1, right panel) with abnormally elevated t1/2 on renal scintigraphy, direct visualization of luminal narrowing on URS, or demonstration of narrowing on retrograde or antegrade pyelography (Fig. 1, left panel). In instances of multiple URS before diagnosis of ureteral stricture, the most recent URS before definitive diagnosis of ureteral stricture served as the referent URS procedure. Patient factors, including demographics (age, body mass index [BMI], American Society of Anesthesiologists [ASA] score, and comorbidities), and stricture characteristics (location, side, and length) were evaluated.
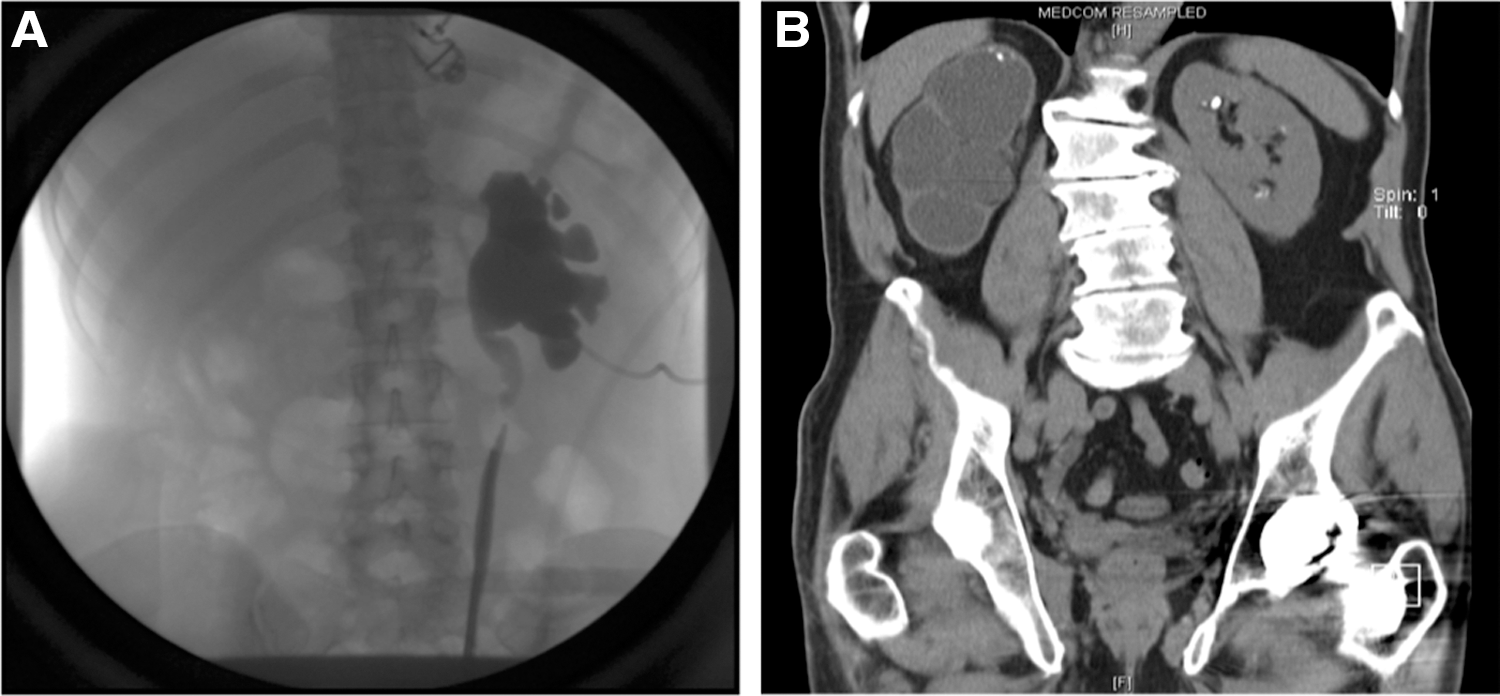
Imaging of postureteroscopy ureteral strictures. Left panel: Retrograde pyelogram of left proximal ureteral stricture requiring robotic ureteroureterostomy. Right panel: Noncontrast CT scan showing incidental finding of silent hydronephrosis and poorly functioning right kidney secondary to severe ureteral stricture years after URS.
Study outcomes included number and type of procedures following diagnosis of ureteral stricture and kidney loss. The number and type of procedures requiring sedation or general anesthesia performed for stricture treatment was evaluated; these included procedures performed after stricture diagnosis both before and after referral to the tertiary care center. Diagnostic procedures (such as retrograde pyelogram or diagnostic URS), drainage procedures (such as ureteral stent or nephrostomy tube placement), and therapeutic procedures as outlined in Table 2 were included in the total procedure count. Procedures not performed under sedation or general anesthesia, including ureteral stent or nephrostomy tube removal, were not included. We secondarily examined the success of subsequent stricture management and defined success as either resolution of hydronephrosis or obstruction on imaging, or resolution of ureteral narrowing on endoscopic evaluation.
Results
Thirty-eight patients with 40 ureteral strictures following URS for upper tract stone disease were included for analysis. Table 1 displays demographic information on patients included for analysis. Most patients (84%) were referred from outside centers; the remaining 15.8% had their index URS at the reporting tertiary care center with a resultant stricture. The mean follow-up interval from definitive operative repair, resolution of stricture, or nephrectomy to most recent imaging study was 17.1 ± 20.2 months (range 1–84 months).
Values are mean unless otherwise specified.
Most (73%) strictures were left sided. Half of strictures were located in the proximal ureter or ureteropelvic junction (UPJ), 43% were in the distal ureter or ureterovesical junction (UVJ), 5.0% were pan-ureteral, and 2.5% were mid ureteral. Forty-eight percent of strictures were ≤2 cm, 33% were >2 cm, and in 20% stricture length was not quantified before repair. The mean number of known URS procedures before stricture diagnosis was 2.5 ± 2.5 (range 1–10). Thirty-five percent of patients developed ureteral stricture after a single URS. Thirty-five percent of patients had hydronephrosis or known stone impaction at the time of initial URS, and 20% of cases had known ureteral perforation at the time of initial URS. The mean interval from URS associated with ureteral stricture to evaluation at tertiary center was 13.6 ± 16.8 months.
Table 2 shows definitive management strategies for patients with post-URS ureteral strictures. After stricture diagnosis, the mean number of procedures requiring sedation or general anesthesia performed for stricture treatment was 3.3 ± 1.8, range 1–10 procedures. Eleven strictures (27.5%) were successfully managed with endoscopic techniques alone. The success rate for any stricture that warranted at least one attempt at endoscopic management was 47.8% (41.2% left-sided strictures, 66.7% right-sided strictures). For those with complete sizing data, 20% of strictures managed successfully with endoscopic techniques were >2 cm, whereas 50% of those requiring reconstruction or nephrectomy were >2 cm (Pearson Chi-2 p = 0.11). Age, gender, ASA score, and BMI were not related to success of endoscopic management.
n = 40.
Ten percent of strictures were primarily managed with chronic internalized ureteral stenting or nephrostomy drainage (Table 2). Three of these four patients had failed prior attempts at endoscopic repair, whereas the fourth patient had chronic ureteral stenting due to patient preference; complicating factors included poor surgical candidacy due to comorbidities and periureteral inflammation or infection.
Fifteen strictures (37.5%) required complex open, laparoscopic, or robot-assisted laparoscopic reconstruction. These procedures included ureteroureterostomy, pyeloplasty, ureteroneocystostomy, ileal ureter, and autotransplant as outlined in Table 2. Sixty-percent of reconstruction cases failed prior endoscopic repair, all of which were left sided, and 13.3% of reconstruction cases required additional endoscopic management or chronic ureteral stenting following reconstruction. There was no relationship between stricture location within the ureter and risk of endoscopic or reconstructive failure.
Ultimately, 25% of patients required nephrectomy to manage their stricture, either due to poor renal function as assessed by renal scintigraphy or, in a single case, due to intraoperative insult during attempt at autotransplant. Twenty-percent of nephrectomy cases had failed prior reconstruction. Age, gender, ASA score, and BMI were not related to risk of nephrectomy. Patients referred from outside centers were not more likely to require nephrectomy. There was no relationship between stricture location within the ureter and risk of nephrectomy.
Discussion
Ureteral stricture presents a unique challenge in the endoscopic management of upper tract stone disease. The ureter is a small, narrow, tubular structure that accommodates urine passage well, but not necessarily rigid objects such as stones or instruments, depending on size. Ureteral strictures can develop from ischemic or nonischemic injury, with endoscopic injury and stones classified as nonischemic etiologies. 12 Although ureteroscope design and technique has advanced over the last two decades, anatomical features of the ureter and sequelae of stone disease can predispose to the development of a stricture.
Our findings suggest high morbidity from URS-induced ureteral strictures, including a high number of procedures following diagnosis, a low overall success rate of endoscopic procedures for managing obstruction in stone formers, and a high rate of nephrectomy. This series also confirms previously described findings, including an association of ureteral stricture with ureteral perforation and a higher likelihood of success of endoscopic management with shorter ureteral strictures. 13 –15
It is not possible to ascertain whether operator error or improper technique contributed to ureteral stricture in these patients. It is possible to develop a ureteral stricture from complex stone disease alone. It is accepted that impacted ureteral stones and overly aggressive instrumentation may contribute to stricture formation with URS. 9 –11 In this series, 35% of stones had known hydronephrosis at the time of initial stone treatment, suggesting a high rate of stone impaction (Fig. 2). In instances of severe ureteral stone impaction, it is often difficult to determine the edge of the stone from the edematous ureteral wall. In these cases, if possible, we advocate considering placement of a ureteral stent and returning to complete treatment after edema has improved in approximately 1–2 weeks. This improves visibility, increases passive dilation, and, in our opinion, reduces the risk of ureteral injury. Leaving stone fragments embedded in the ureteral wall is also thought to portend a much greater risk of developing a subsequent stricture. Removing all embedded stone fragments (Fig. 2, right panel) from the ureter is necessary to prevent ureteral strictures.
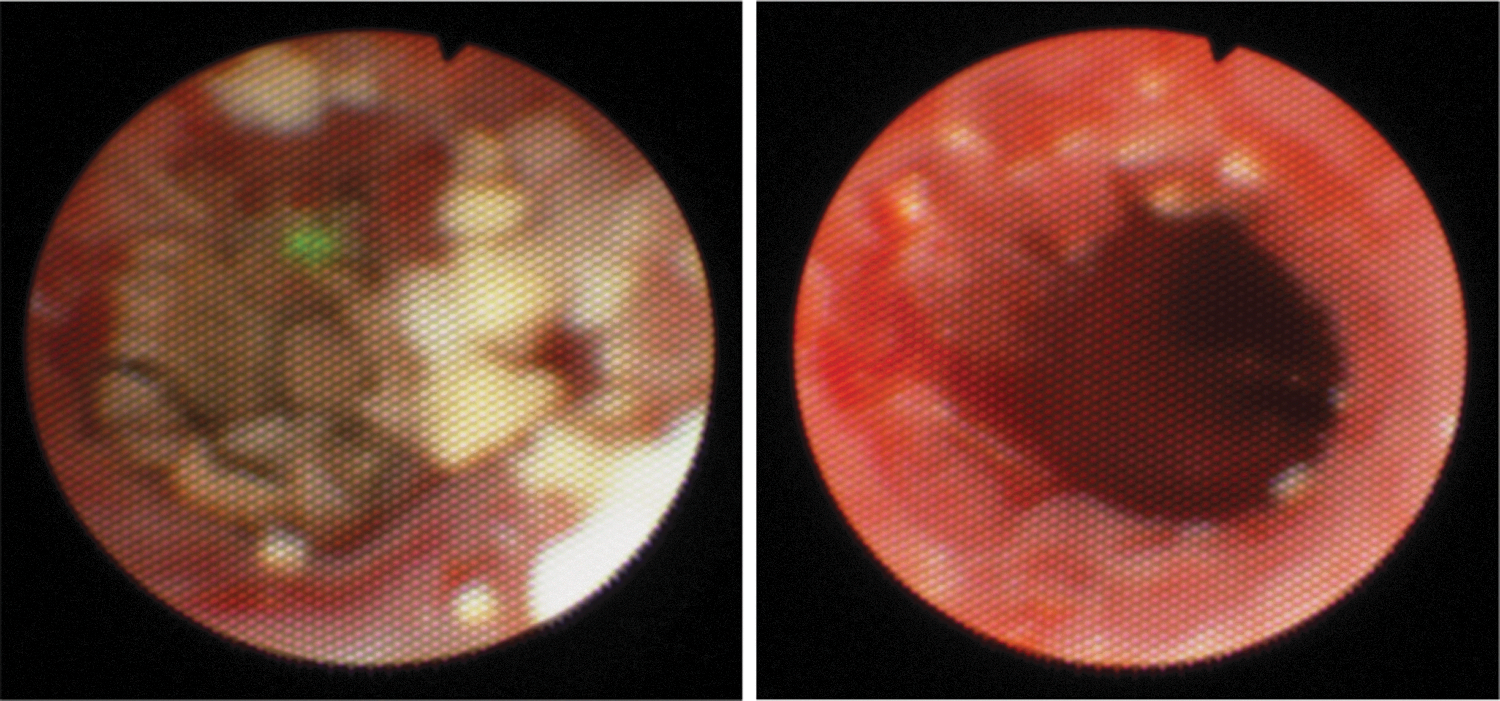
Ureteroscopic images of impacted ureteral stone. Stone treated without ureteral injury or development of stricture. Stone impaction of this type potentially increases risk of ureteral stricture.
Our series exhibited a 2:1 predominance of left-sided ureteral strictures. Both proximal and distal ureteral strictures had a similar left-sided predominance. Congenital UPJ obstruction has a similar 2:1 left-sided predominance of unknown etiology. Ureteroenteric anastomotic strictures also show a higher rate of left-sided stricture, which is believed to be related to increased mobilization and transposition of the left ureter beneath the sigmoid mesentery during ileal conduit formation. Left-sided ureteroenteric anastomotic strictures also have a lower response rate to endoscopic management. 16,17 Altogether, these points suggest that the left ureter may have an anatomic or functional predisposition to obstruction.
Prior studies have demonstrated reduced success of endoureterotomy with strictures over 2 cm. 16,17 The success rates of endoureterotomy and balloon dilation for benign ureteral strictures are 62%–100% and 50%–76%, respectively, with a suggestion based on published series of higher success rate (85%) managing benign iatrogenic strictures. 18 The success of holmium laser endoureterotomy is between 66% and 83%. 18 Our series shows a much lower success rate of 27.5% with endoscopic management. There are many potential explanations for this finding, including a bias in patient complexity, with 84% of patients referred for management at tertiary care facilities. Alternatively, strictures incurred from ureteroscopic injury are potentially more complex and challenging to manage; this suggestion was also made by Gdor et al., who demonstrated a lower (56%) success rate in managing ureteral strictures incurred following stone impaction and URS. 8
We were not able to completely evaluate the impact of commonly used surgical technologies and techniques, including use of repetitive basketing, UAS, or semirigid ureteroscopes. UAS have a number of potential advantages in the management of nephrolithiasis, including facilitation of URS access, reduction of intrarenal pressures, and improved visibility. 19 The effect of UAS on stone-free rates following URS is unclear. 20,21 Although there are advantages to UAS, they have been associated with an increased risk of ureteral injury and reduced ureteral perfusion, particularly with larger diameter (>12–14 French) sheaths. 19,22 A recent prospective study of 359 patients undergoing retrograde URS with UAS showed a 46.5% overall rate of ureteral wall injury, with a 13.3% rate of severe injuries involving ureteral smooth muscle. 23 Additionally, recent reports demonstrate a higher risk of stricture with increased dwell time of UAS in a porcine model. 24 Review of the Manufacturer and User Facility Device Experience (MAUDE) database of ureteral avulsions during URS did report two instances of ureteral avulsion in the setting of UAS, although due to insufficient reporting of UAS use, a definitive link between UAS and avulsion could not be established. 25 Although a higher rate of ureteral stricture with UAS has not been definitively shown in clinical studies, the known association with ureteral injury and ischemia suggests that UAS may contribute to some ureteral strictures. This warrants further prospective investigation.
To successfully manage complex ureteral strictures, a surgeon requires familiarity with a sophisticated armamentarium of procedures. In our experience, this requires a team-based approach to provide expertise in endoscopic, minimally invasive, and open repair. Of the strictures successfully managed with endoscopic techniques alone, 82% were managed with a single endoscopic incision or dilation; the remainder were successfully managed with two procedures. Sixty percent of patients managed with reconstruction procedures failed prior endoscopic repair. Considering the low success rate of endoscopic procedures and the morbidity of reconstruction, we advocate consideration of early referral to a specialized center for management if a single attempt at endoscopic management is not successful. This approach may reduce cost and preserve renal function. This mirrors recommendations for management of urethral strictures, as the difficulty of repair increases with each unsuccessful attempt. 26
Nephrectomy following URS for stone disease is a serious complication, especially given the recurrent nature of the disease. Renal obstruction from ureteral stricture may be asymptomatic and can rapidly lead to renal functional loss, necessitating nephrectomy. 27 There has been considerable debate regarding the role of imaging after routine URS. 11 A recent AUA best-practice document supports routine postoperative imaging to evaluate for silent hydronephrosis, a strategy that has been shown to be cost effective. 28,29 As of 2015, over 50% of patients in a national cohort of privately insured patients did not receive imaging following URS. 30 We recommend routine follow-up imaging with renal ultrasound following URS to reduce the risk of silent obstruction and renal functional loss.
This study has several limitations. As a retrospective series primarily comprised of referred patients, we cannot assess the rate of post-URS ureteral stricture because the total number of URS cases is unknown. A lack of complete preoperative and intraoperative information regarding the initial stone treatment–including stone size, renal or ureteral stone location, and use of UAS or basketing–made assessment of detailed risk factors beyond ureteral perforation and stone impaction challenging. Since risk factors, including ureteral stone impaction, ureteral perforation, and various operative factors may coexist, all ureteral strictures following URS were considered as a single group. Patients also commonly received URS with multiple urologists for both renal and ureteral stones before development of ureteral stricture. Despite these limitations, it is our belief that this topic is timely, and this series provides useful descriptive information moving forward regarding the management and morbidity of ureteral strictures incurred following URS for renal stone disease.
Conclusion
Ureteroscopy has become the most commonly used treatment for upper tract stone disease. Ureteral stricture is a rare complication, but the surgical morbidity of these strictures can be severe with a low rate of successful endoscopic management, a high rate of nephrectomy, and a high procedural burden. We favor a combination of conservative ureteroscopic instrumentation with ureteral stenting in the instance of severe stone impaction, routine postoperative imaging to hasten the diagnosis and mitigate the morbidity of ureteral strictures, and consideration of early referral to a specialized center if initial endoscopic repair of a stricture fails. This approach may reduce cost and preserve renal function. Further studies that prospectively assess specific technical risk factors for ureteral stricture following URS are needed.
Footnotes
Acknowledgments
This work is part of a multi-institutional effort to investigate urinary stone disease, and we appreciate the great support of our institutional faculty and staff in supporting this research.
Author Disclosure Statement
All study authors have no competing financial interests.