
Abstract
Objective:
The aim of the present anatomic and radiologic study was to evaluate the location, extension, and characteristics of the Brödel's plane and eventually define its different patterns.
Materials and Methods:
We evaluated 15 human normal kidneys sampled from unembalmed cadavers without clinical history or anatomical evidence of renal diseases. Kidneys with the surrounding perirenal fat tissue were removed en bloc with the abdominal segment of the aorta. The renal artery was injected with acrylic and radiopaque resins. A CT examination of the injected kidneys was performed. After the imaging acquisition, the specimens were treated with sodium hydroxide for removal of the parenchyma to obtain the vascular casts. All the CT images were elaborated using dedicated three-dimensional (3D) software with the aim to improve the possibility to identify the Brödel's plane. The avascular plane was identified directly on the vascular casts and confirmed on the corresponding 3D images.
Results:
The avascular plane was located in all cases medially to the lateral convex border of the kidneys. The recorded mean distance was 2.04 cm (range 1.8–2.4 cm). Three patterns of distribution of the Brödel's line were identified. In five (33.3%) cases the avascular plane was extended from the apical to the inferior segment of the kidneys (type 1); in six (40%) from the superior to the inferior segment (type 2); and in four (26.7%) from the apical to the middle segment (type 3). Fourth and fifth order vessels crossing the Brödel's line were detected in all the analyzed cases.
Conclusions:
The renal avascular plane showed a different extension allowing us to cluster three different patterns. Preoperative identification of the Brödel's line patterns could help surgeons to minimize hemorrhagic complications during percutaneous and surgical procedures requiring an incision of the renal parenchyma such as traditional or robot-assisted nephrolithotomy or partial nephrectomy for endophytic renal tumors. Radiologic studies validated that the described patterns in the clinical practice are strongly needed.
Introduction
T
The recent renaissance of interest for pure laparoscopy and robot-assisted nephrolithotomy instead of multiple percutaneous procedures, as well as the wide diffusion of partial nephrectomies for totally endophytic tumor, propose again the attention of the urologists on anatomical and radiologic landmarks to identify the renal avascular plain. 3 –6
However, after the historical Brödel's description, the few available studies described a significant variation in the location of this plane highlighting the necessity of a careful preoperative delineation before incisures. 7,8 Recently, we confirmed the subdivision of the main renal artery in two first order arteries represented by a posterior and an anterior branch, the latter further divided in segmental arteries perfusing the apical, superior, middle, and inferior anterior segments of the kidney. 9 Casts and CT scan images obtained in previous study represent good models to study the Brödel's characteristics in human cadaver kidneys.
Therefore, we performed an extension of the previous study with the aim to evaluate the location, extension, and characteristics of the Brödel's plane and eventually define its different patterns.
Materials and Methods
We reviewed the vascular casts and the CT scan imaging obtained from 15 human normal kidneys sampled from unembalmed cadavers without clinical history or anatomical evidence of renal diseases. The scientific coordinator of the donation program approved the study. The protocol used to obtain vascular casts of the renal arteries and CT scan imaging acquisition has been previously described in detail. 9 –11 Briefly, kidneys with the surrounding perirenal fat tissue were removed en bloc with the renal segment of the aorta. Maintaining the specimen in water, the renal artery was injected with acrylic and radiopaque resins (200 mL, Beracryl; Troller, Fulenbach, Switzerland). A CT scan examination of the injected kidneys was performed to analyze the branches located deeply, result difficult to visualize in the surface analyses of the vascular casts. The CT axial scans (Philips Medical Systems, Best, The Netherlands) were performed according to the following parameters: slice thickness 1 mm, 140 kV, and 350 to 400 mA. After the imaging acquisition, the specimens were treated with sodium hydroxide for removal of the parenchyma to obtain the vascular casts. Then, a second CT scan examination of the obtained vascular casts was performed in all cases with the same parameters of the first CT scan.
Differently from the previous study, all the CT images obtained from the casts were acquired and elaborated with an imaging software (Mimics in Print version 2.0; Materialise, DE) with the aim to improve the possibility to identify fissures between the different renal segments and the extension of the Brödel's plane. In Mimics inPrint the reconstruction of the patient's anatomy from DICOM images is performed based on the selection of gray values. The workflow can either be to define a range of gray values for the complete dataset and to crop and erase redundant parts or to mark and interpolate between slices and to apply a threshold locally. The region of interest can be edited by adding or erasing parts that should or should not be included in the final three-dimensional (3D) model using various tools. Finally, a stereolithography format file (STL) is generated from the marking on the 2D images to obtain a printable 3D model. Applying previous methodology, CT images were reconstructed to generate a 3D model comparable to vascular cast. The advantage of the 3D model is that in the real vascular cast it can be difficult to analyze its deepest part, while in the 3D model each order of renal branches can be virtually removed to better analyze them. The analysis of the branching of the renal artery was independently performed by two of the authors on the vascular casts and confirmed on the corresponding traditional and 3D radiologic images. A different color for each order of branching was applied.
The Brödel's line was identified as the presence of a fissure between the anterior (apical, superior, middle, and inferior) and posterior renal segments defined according to the Graves classification. 12 The avascular plane was identified directly on the vascular casts and confirmed on the corresponding 3D images. In all cases, we measured the distance (mm) between the lateral convex border of the kidney and the avascular plane using a digital caliber. Moreover, we classified the extension of the Brödel's line using as reference the renal segments where it was visible. Finally, we recorded the presence of fourth and fifth order vessels crossing the Brödel's line. When present, these small arteries were classified according to the renal segments in which they were located.
Results
The study was performed on 15 normal kidneys sampled from 8 unembalmed cadavers. In eight specimens the left kidney was evaluated and in the remaining seven cases the right ones. The mean age of the donors was 66 ± 12 years. Two cadavers were males and six females. In all cases an avascular fissure between anterior and posterior arterial branches was identified both on the vascular casts and on the 3D CT-scan images. This plane was located in all cases medially to the lateral convex border of the kidneys. The recorded mean distance was 2.04 cm (range 1.8–2.4 cm).
Three patterns of distribution of the Brödel's line were identified. In five (33.3%) cases the avascular plane was extended from the apical to the inferior segment of the kidneys (type 1) (Fig. 1); in six (40%) from the superior to the inferior segment (type 2) (Fig. 2); and in four (26.7%) from the apical to the middle segment (type 3) (Fig. 3).
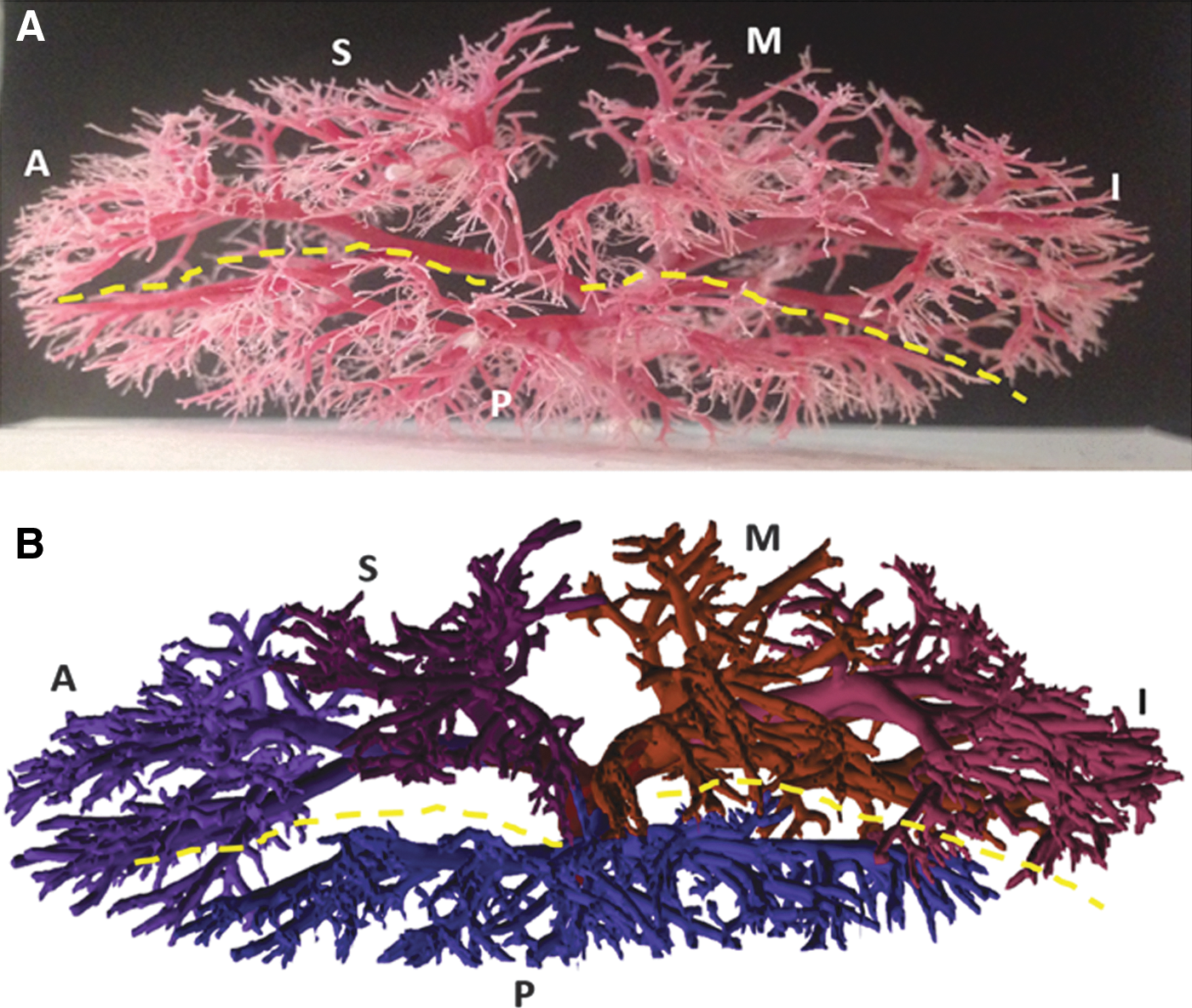
Pattern type 1 of avascular plane with extension from apical to inferior segments.
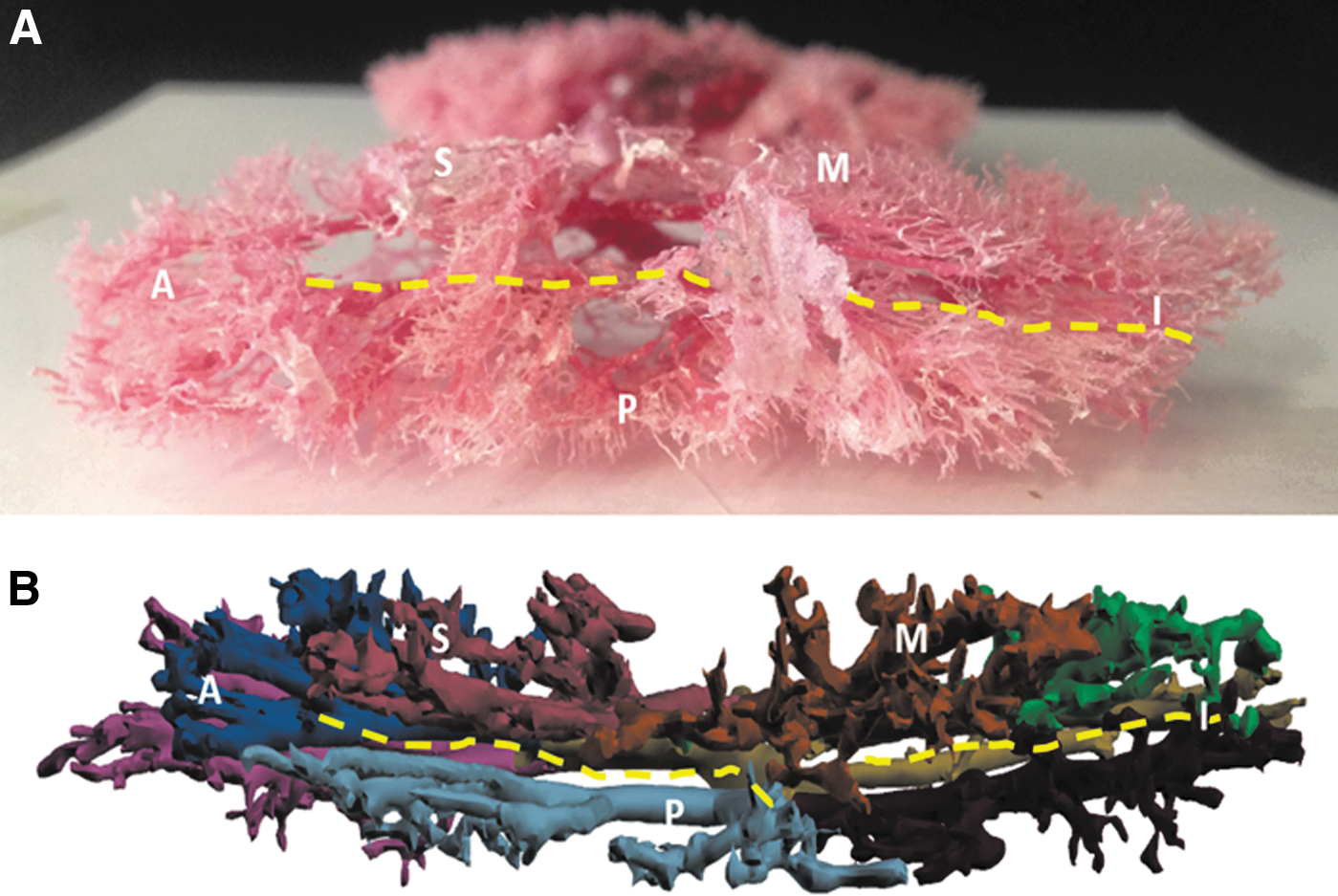
Pattern type 2 of avascular plane with extension from superior to inferior segments.
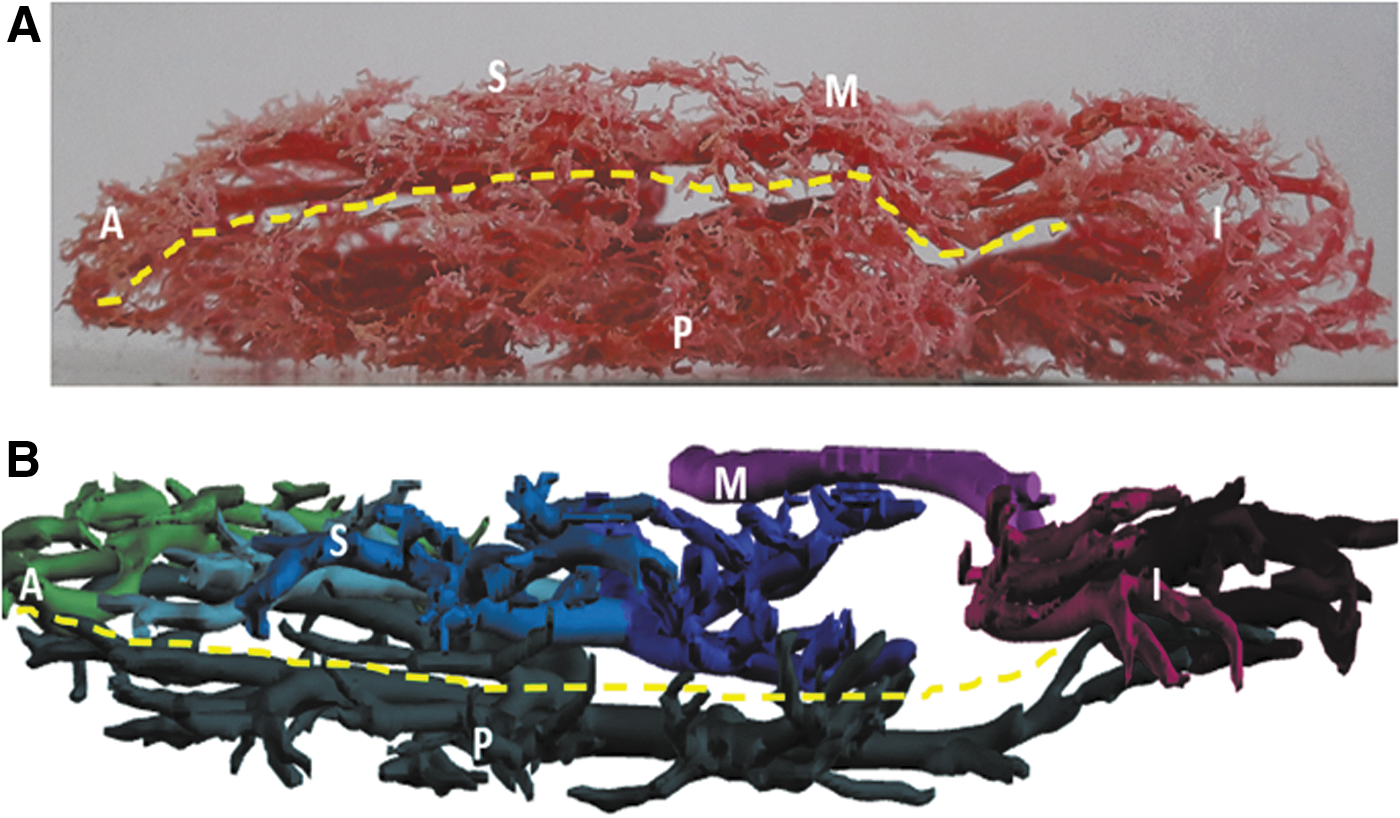
Pattern type 3 of avascular plane with extension from apical to middle segments.
Fourth and fifth order vessels crossing the Brödel's line were detected in all the analyzed cases. Specifically, these arteries were located at level of the middle segment in 15 (100%) cases, at level of the superior segment in 4 (26.7%) cases, and at level of the inferior segment in 5 (33.3%) cases. Interestingly, crossing vessels are presented at the level of middle segment in all the type 3 Brödel's line. Therefore in two cases too, the superior segment area was characterized by the presence of crossing vessels. Only in 2 (18%) of remaining 11 type 2 and 3 cases we observed crossing vessels at level of superior, middle, and inferior segments (Table 1).
Discussion
The present anatomical and radiologic study showed that the renal avascular plane located about 2 cm medially to the lateral convex border of the kidneys showed different extension and characteristics. Interestingly, we described three different patterns according to the anterior renal segments used as topographic reference. This Brödel's line variability can be explained considering the embryologic development of the kidney at the 4th week stage, when the glomeruli develop from the ventral wall of the nephroceles (internal glomeruli) or from the roof of the coelom adjacent to the peritoneal funnels (coelomic or external glomeruli). The two groups of glomeruli receive proper branches from the aorta called lateral splanchnic arteries: one for the internal glomeruli ventrally located and destined to disappear and another for the external glomeruli dorsally located. 13 The precocity of acquisition of the vascular source by the glomeruli placed dorsally with respect to the subsequent acquisition of the vascular source of glomeruli ventral placed may explain the existence of the branching pattern of the posterior artery (single vessel) with respect to the high variability of the branching of the anterior artery (one, two, or three branches). This different vascular supply and the different time of acquisition can explain the different extension of the Brödel's line.
Usually the Brödel's line is described as an avascular plane approximately at the lateral margin of the kidney, extending from the superior pole of the kidney (limited by the circulation of the apical segmental artery) to the lower pole of the kidney (limited by the circulation of the lower segmental artery). 14 However, some authors highlighted that the anatomical variations of this plane need a careful preoperative delineation to perform safer percutaneous or surgical procedures. 7,8 Interestingly, we described two different patterns in which the avascular plane was extended to the apical segment of the kidney (type 1 and type 3) and one pattern in which the lower extension of the Brödel's line was limited to the middle segment of the kidney. Moreover, we found that the avascular plane was located in all the evaluated cases about 2 cm medially to the lateral convex margin of the kidney. Of course, in our study the CT scan and 3D images were obtained using thin thickness of the slices and higher acquisition parameters in comparison with conventional angio-CT scan examination. Therefore, further studies should be performed to optimize the acquisition protocol of CT scan with the aim to obtain a good reconstruction of the arterial vasculature also in the routine examination.
The use of dedicated software for imaging elaboration can help significantly clinicians to better interpret the vascular anatomy and the definition of fissures demarcating different renal segments and the Brödel's line. Notably, this is the first study documenting the Brödel's line arrangement in a virtual vascular model generated from a real vascular anatomy. In alternative to the preoperative imaging evaluation, in patients who underwent robot-assisted procedures the renal avascular plane could be identified using the near-infrared fluorescence (NIRF) with indocyanine green (ICG) and Firefly™. However, this interesting application has been recently evaluated only in an animal model study simulating a robot-assisted anatrophic nephrolithotomy. Interestingly, in both porcine subjects the authors demonstrated that NIRF image guidance was able to identify the renal avascular plane.
The correct identification of the Brödel's line might deserve several potential applications in the field of renal surgery.
According to the Brödel description, a safe access route to the upper collecting system for nephrostomy insertion should be done at level of the lowermost posterior calix. However, bleeding, pseudoaneurysm formation, or arteriovenous fistulas can complicate percutaneous nephrostomy placement or operative procedure performed through this way in 1% to 12% of the cases. 15,16 Our study highlighted that in about 20% of cases the avascular plane is absent at level of the inferior segment of the kidney (Fig. 3). This anatomical pattern can explain some unexpected hemorrhagic complications theoretically avoidable using the avascular fissure located at level of middle or superior segments. Although our data demonstrated an avascular plane at level of superior segments in all cases, vascular complications after a puncture of superior or middle posterior calices can be present in 18% of cases. 17
Although percutaneous nephrolithotomy with prone or supine approach remains the gold standard treatment of large renal stones, recently some authors reconsidered the opportunity to reach the complete stone clearance in a single treatment performing laparoscopy or robot-assisted nephrolithotomy. 3 –6 Most of the authors highlighted the importance to identify and follow the right avascular plane to minimize the risk of vascular complications and renal failure after modern anatrophic nephrolithotomy. 5,6 Differently from the milestone article by Brödel, we believe that trained eye cannot be considered a sufficient tool to correctly identify the renal avascular plane, and dedicated imaging protocols able to identify almost first, second, and third order arteries should be implemented.
Interestingly, the analysis of vascular casts and their corresponding 3D reconstruction allowed us to visualize in all cases the presence of fourth and fifth order arteries crossing through the avascular plane. These crossing vessels are more represented in Brödel's plane with type 3 pattern and at level of middle segments of the kidney. Lesion of these small arteries during percutaneous procedures could justify potential hemorrhagic events also in cases in which the maneuvers are correctly performed. During traditional or robot-assisted procedures these small arteries can be easily sealed and cut using several hemostasis devices. 9 A further clinical application of the preoperative correct demarcation of the Brödel's could be represented by the conservative treatment of endophytic parenchymal renal tumors using partial nephrectomy. Indeed the avascular plane could be used to minimize the bleeding during the initial incision of the healthy parenchyma around the endophytic tumor.
The potential limitations of present study are represented by the small number of kidneys evaluated and by the fact that the majority of the analyzed specimens were from female cadavers. Renal cell carcinoma (RCC), indeed, is more frequent in male patients and differences in renal vasculature can be present according to the gender. 18 Another potential limitation is represented by the CT image acquisition obtained using a not conventional exposure dose. Therefore, the results of this study should be validated in clinical practice preferable using the angiographic CT scan with 3D technology. 19
Conclusions
The renal avascular plane is always consistent at level of the middle segment of the kidney, about 2 cm medially to the convex border, while the variability may occur at level of the apical superior or inferior segments. The type 2 pattern extended from superior to inferior segments seems to be more frequent followed by the type 1 extended from apical to inferior segments of the kidney. Type 3 pattern results are more interesting on the surgical point of view considering its extension limited from the apical to the middle segment of the kidney. Interestingly, in every case we documented the presence of fourth or fifth order arteries crossing the Brödel's line with predominance at level of middle portion of the kidney.
Preoperative identification of the Brödel's line patterns could help surgeons to minimize hemorrhagic complications during percutaneous and surgical procedures requiring an incision of the renal parenchyma such as traditional or robot-assisted nephrolithotomy or partial nephrectomy for endophytic renal tumors. Radiologic studies validated that the described patterns in the clinical practice are strongly needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.