
Abstract
The past decade has witnessed a dramatic increase in utilization of robot-assisted radical cystectomy (RARC). RARC has been shown to offer some perioperative benefits in terms of blood loss, transfusion rates, hospital stay, and recovery when compared with its open counterpart without jeopardizing oncologic outcomes. In this article, we review the indications, perioperative care, and describe the “Technique of Spaces” of RARC employed at our institution, and highlight the key steps for male RARC.
Introduction
The past decade has witnessed a dramatic increase in utilization of robot-assisted radical cystectomy (RARC) (from 0.6% in 2004 to 23% in 2012). 1 RARC has been shown to be more superior in terms of blood loss, transfusion rates, hospital stay, and recovery than its open counterpart without jeopardizing oncologic outcomes. 2 –6 The technique for RARC has evolved since it was introduced in 2003. 7 In this article, we describe the “Technique of Spaces” employed at our institution, and highlight the key steps for male RARC.
Indications
Radical cystectomy (RC) is the standard of care for patients with localized muscle invasive bladder cancer (T2–T4a, N0, M0). It is also indicated in patients with nonmuscle invasive bladder cancer (NMIBC) not responding or tolerating transurethral resection and Bacillus Calmette Gurein intravesical therapy. 8 RC is an option to patients with NMIBC who are at high risk of progression, for example, high grade T1 and concurrent carcinoma in situ. 9 RC can be offered as a palliative management for locally advanced and metastatic disease to alleviate local symptoms such as hematuria, pain, or fistulation.
Preoperative Preparation
Incorporation of enhanced recovery after surgery or fast track protocol in the perioperative period has been shown to promote recovery, shorten hospital stay, return of bowel function, and improve quality of life. 10 Thorough counseling and education regarding procedure details and possible complications in addition to discussion of the patient expectations are vital. Optimization of the nutritional status of the patient has been shown to minimize surgical morbidity and also help early return of bowel function. Smoking cessation helps improve preoperative pulmonary and cardiac reserve. For patients who are planned to receive ileal conduits, the role of stoma nurse is crucial to help patients understand the changes that will happen to them in terms of body image, as well as determine the most suitable position of the stoma and explain the main principles of stoma care. Teaching intermittent self-catheterization should be provided for patients eligible to neobladders. Comprehensive preoperative counseling has been shown to motivate patients, improve recovery, and reduce complications. 11
A comprehensive preoperative evaluation of the patient's medical conditions including detailed medical and surgical history and comprehensive assessment are mandatory. Given the strong association between smoking and bladder cancer, and also that the average age is 67 years, patients usually have multiple comorbidities, especially pulmonary and cardiac diseases. The steep Trendelenburg position also poses additional challenge. Addressing the modifiable risk factors is crucial by encouraging breathing exercises, smoking cessation, diet counseling, and nutritional supplementation for malnourished individuals. 12 –14
Patients are instructed to abstain from eating vegetables 24 hours before surgery. Oral intake of solids and liquids is allowed up to 6 and 2 hours, respectively, before surgery. Carbohydrate loading (e.g., apple juice) 2 to 3 hours before surgery has been shown to reduce the surgery-associated catabolic effects, promote postoperative muscle strength and bowel function. 11 There is level I evidence to support skipping mechanical bowel preparation. 15 –17 Venous thromboembolic prophylaxis includes mechanical methods such as compression stockings or intermittent pneumatic compression. 18 Single dose broad-spectrum antibiotic is administered before incision in concordance with American Urological Association and Surgical Care Improvement Project guidelines. 10
Patient Positioning
The patient is placed in steep Trendelenburg position (to increase the intraperitoneal working space as it displaces the bowel cranially. A Veress needle or Hasson technique is used to achieve the pneumoperitoneum. A standard six-port transperitoneal approach is used. The 12 mm camera port is first placed an inch above and to the left of the umbilicus. A 30-degree lens is then introduced to inspect the abdominal cavity. All other ports are introduced under vision. Three 8 mm robotic trocars are introduced in addition to 15 mm assistant port, and a 5 mm suction port. An additional 12 mm short suprapubic port is placed later to facilitate bowel anastomosis (Fig. 1). A 22F Foley catheter is inserted. Some surgeons prefer to insert a rectal tube as well.
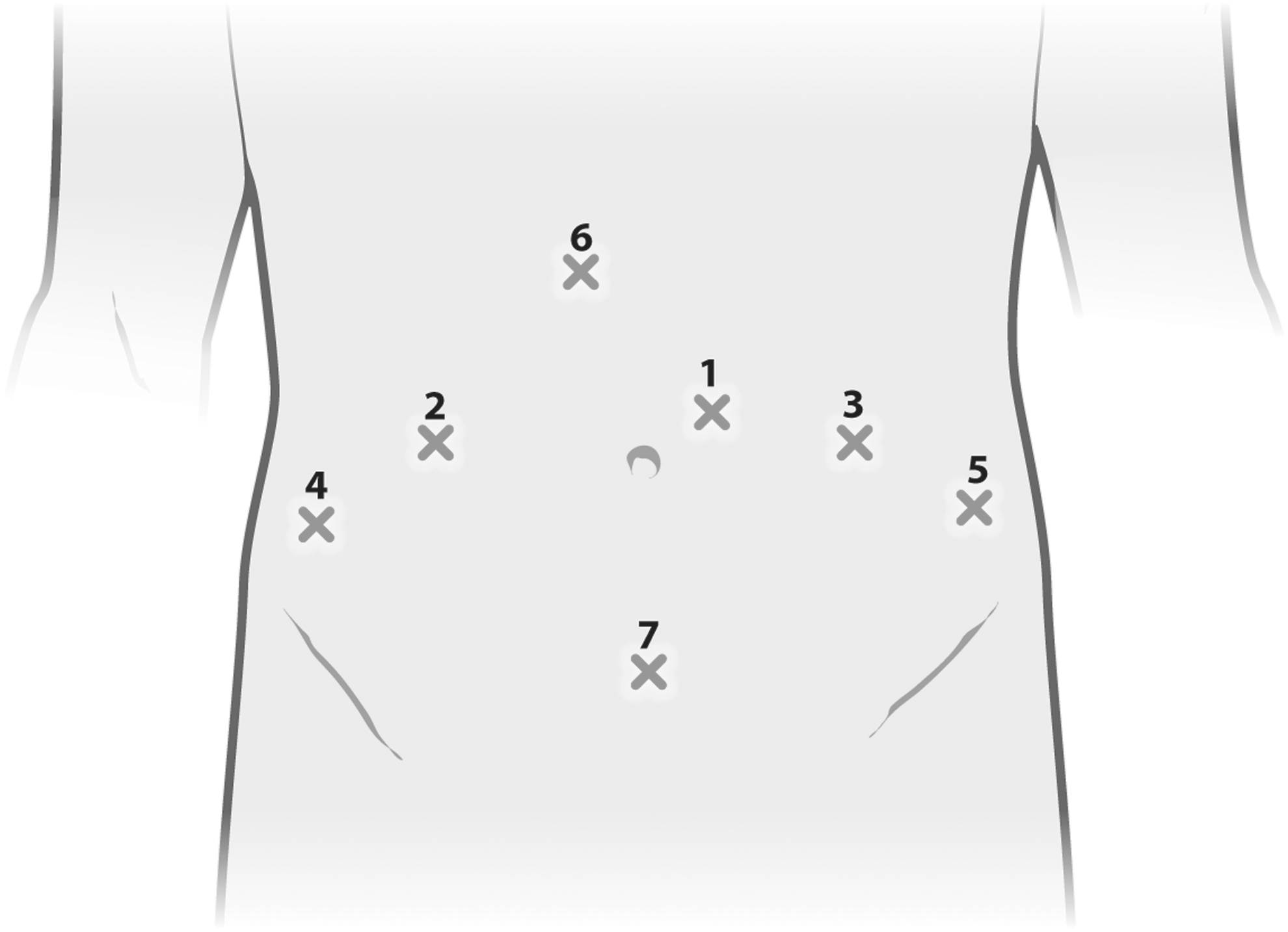
Six-port transperitoneal configuration:
Instruments
Robotic instruments—we use the following instruments: long tip grasper, monopolar hook, one pair round tip scissors, two needle drivers, bipolar forceps, and cobra grasper. Laparoscopic instruments—we use the following instruments: two graspers, one pair of scissors, one fan retractor, one suction irrigator, and one laparoscopic needle drivers. We use staplers for pedicle control and clips for the control of blood vessels and ureters. A specimen bag is used for specimen entrapment.
Surgical Technique
The “Technique of spaces” deconstructs the procedure into measurable steps, which, in turn, facilitates the description of the procedure and the teaching process. The four spaces of dissection are the periureteral, lateral pelvic, anterior rectal, and retropubic spaces. 7,19
Periureteral space
Using a cobra grasper in the fourth arm, we retracted the sigmoid colon medially to improve exposure and facilitate further dissection. The posterior peritoneum is incised above the iliac vessels using hook or hot scissors. The ureter is then dissected while preserving adequate periureteral tissue to avoid ischemia of the distal ureter. Occasionally, dissection on the left side may be more challenging owing to inflammatory adhesions associated with diverticulitis. Distal dissection of the ureter is continued toward the ureterovesical junction.
Lateral pelvic space
Lateral pelvic space is identified by incising the peritoneum just lateral to the umbilical ligament. Dissection is then extended toward the ipsilateral ureter. Blunt dissection in a sweeping manner of the areolar tissue is performed from lateral to medial to avoid injury of the external iliac vessels until the endopelvic fascia is observed. The vas is encountered during this dissection and can be divided with the hook cautery. Incision of the endopelvic fascia can then be performed (Fig. 2).

Incision of the endopelvic fascia.
Anterior rectal space
Once both left and right lateral pelvic spaces are developed, the posterior peritoneum of the Douglas pouch between both ureters is incised horizontally across the midline (Fig. 3). The plane between the urinary bladder, seminal vesicles and prostate (anteriorly) and the rectum and overlying Denonvillier's fascia (posteriorly) is then opened, blunt dissection is continued distally down to the urethra.
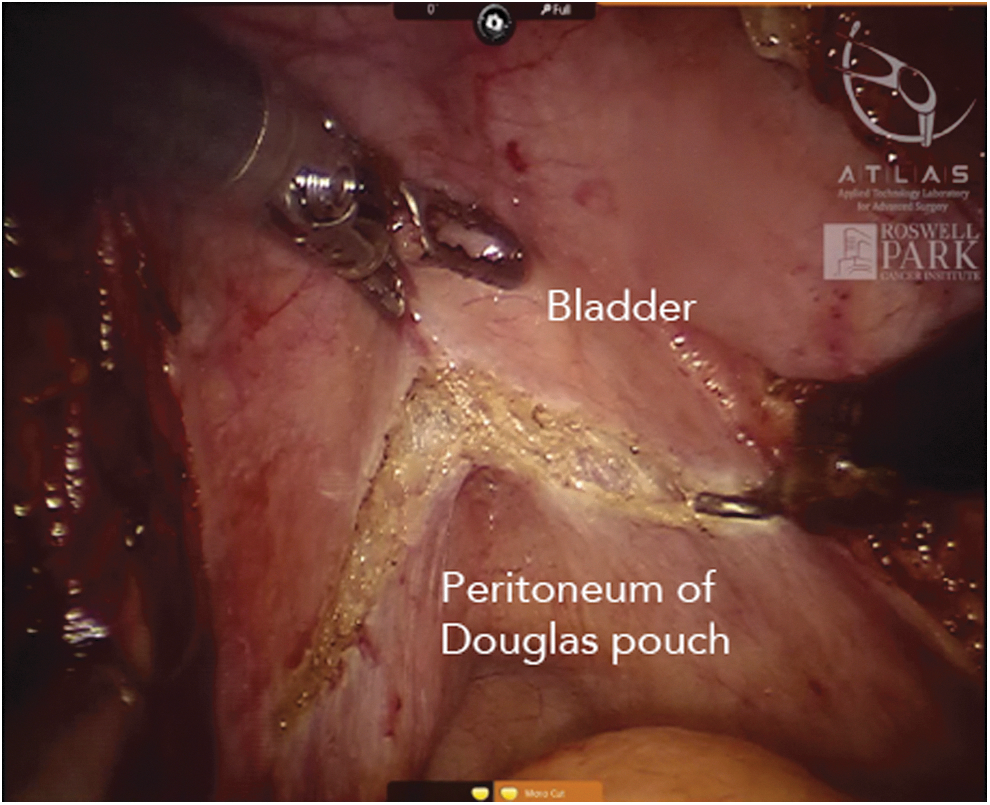
Anterior rectal space incision.
Control of vascular pedicle
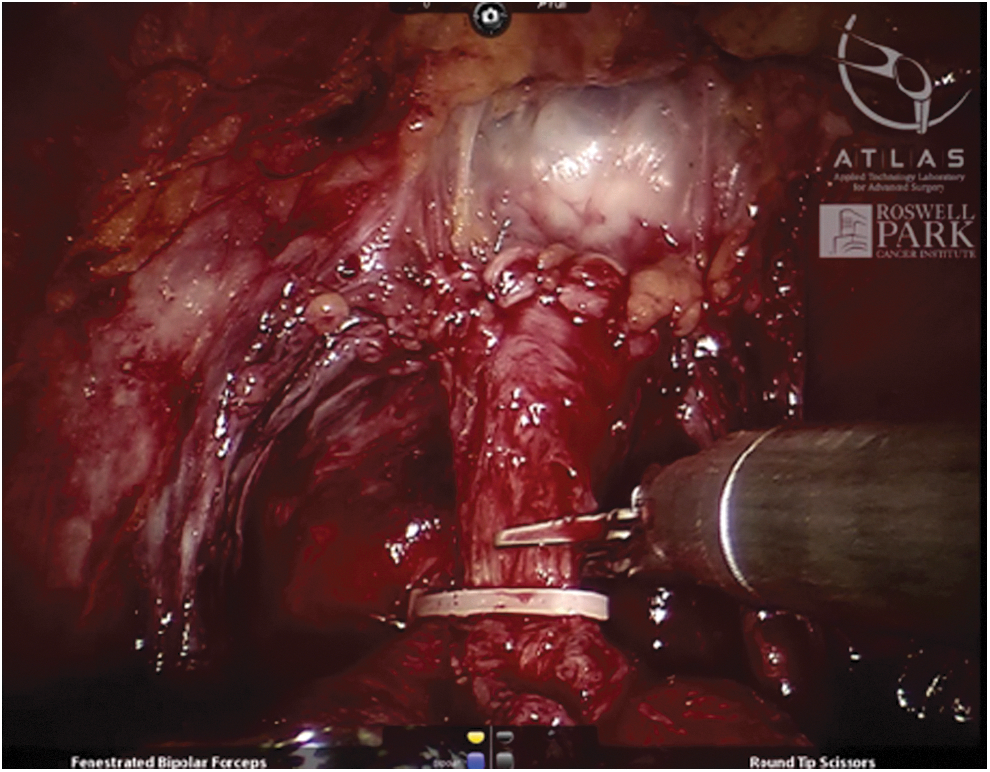
Once the lateral pelvic and anterior rectal spaces are developed, the vascular pedicle is defined. The ureters are then clipped and distal margins are sent for frozen section. The Endo GIA™ stapler (Medtronic) is used to divide the lateral vesical pedicle (Fig. 4).
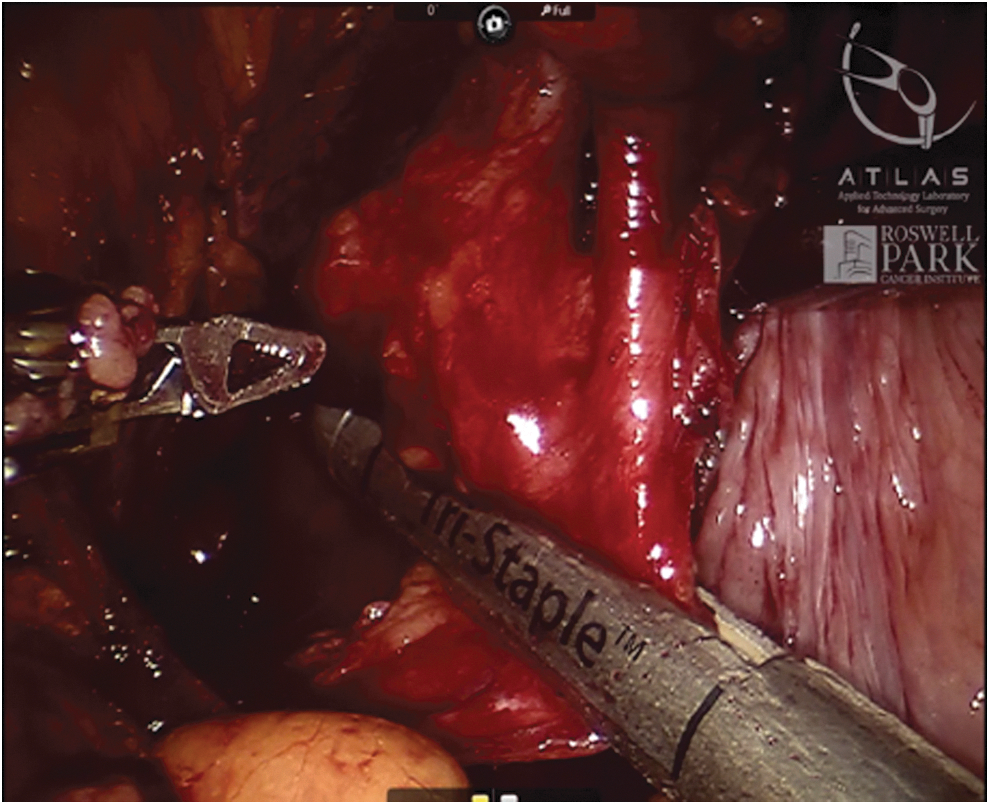
Control of the vascular pedicle using Endo GIA™ stapler.
Retropubic space of retzius (anterior vesical space)
The bladder is separated from the anterior abdominal wall by incising the urachus (Fig. 5). The incision should be as cranial as possible and continued till the urethrovesical junction and the dorsal venous complex (DVC) are seen.
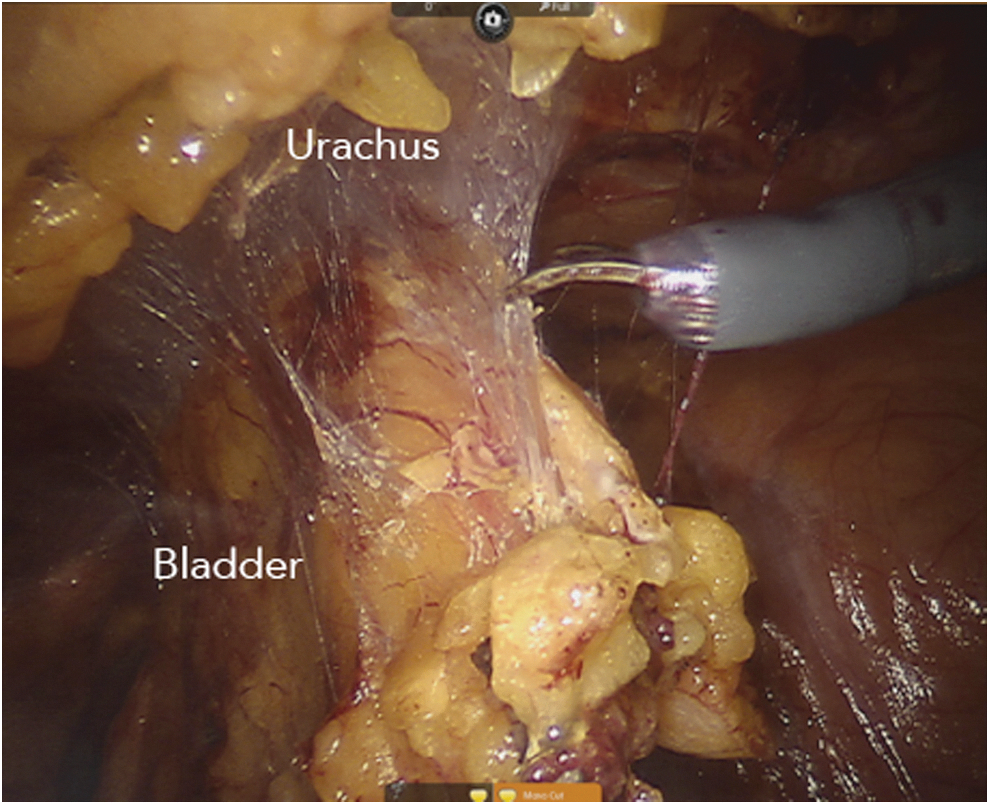
Incision of the urachus during bladder drop.
Apical dissection: DVC control and urethral transection
After increasing the pneumoperitoneum pressure to 20 mm Hg, the DVC is divided using a hook cautery or cold scissors (if nerve-sparing RARC was planned). The DVC is then controlled using a 3/0 barbed suture (Fig. 6). Some surgeons prefer to control the DVC before dividing it. The Foley catheter is manipulated by the bedside assistant and the urethra is clipped and then transected using cold scissors, preserving as much urethral length as possible especially if orthotopic diversion is planned (Fig. 7). Proximal end of the urethra is sent for frozen section to determine tumor involvement, and whether a neobladder can be performed or a urethrectomy is necessary.

Dorsal venous complex control using 3/0 barbed suture.
Urethral transection
Postoperative Care
It is crucial to optimize pain control postoperatively to enhance recovery. Efforts should be made to avoid opioid analgesics unless indicated for its effect of bowel function. Baseline therapy should include acetaminophen. Epidural analgesia can be used and has shown its effectiveness. However, it limits patient mobility and is not necessary for RARC patients. 10
Early mobilization, breathing exercises, and gradual institution of oral diet should be encouraged as tolerated from day 1. 10,11,18 Appropriate use of the incentive spirometer improves patient respiratory functions and reduces the risk of lung infections. 20 Postoperative ileus is not uncommon, chewing gum, alvimopan, and mobilization have been shown to promote early return of intestinal functions. 21,22 The use of alvimopan should be with caution in patients with cardiovascular diseases. 22 Prolonged low-molecular weight heparin prophylaxis (LMWH) compression stocking reduce the risk of late thromboembolic events. 23,24 LMWH should be continued for 4 weeks after surgery. 10
Challenging Situations
The Pasadena consensus for best practices for RARC showed that prior abdominal surgery, pelvic irradiation, morbid obesity and locally advanced disease are not contraindications for RARC. However, these challenging cases should be only performed by high-volume experienced surgeons. 25 Disruption of the normal pelvic anatomy and associated adhesions, in addition to compromised vascularity of the bowel may all render RARC very challenging. In the setting of locally advanced disease, wider resection is prudent to ensure complete tumor resection and avoid surgical margins. It is also imperative to clip the ureters and urethra and avoid urine spillage; a concern that has been always there that urine spillage may lead to tumor seeding and contribute to local recurrence after RARC. 26
Thorough lymph node dissection is crucial for adequate tumor staging and also for removal of micrometastatic disease. There has been a growing body of evidence that extended lymph node dissection (up to the aortic bifurcation and including presacral lymph nodes) has been associated with improved survival when compared with standard and limited templates, and is not inferior to super extended dissection up to the level of the inferior mesenteric artery. However, the optimal template and level of dissection are yet to be determined. 27 –29
Recommended Video from Videourology
Tips and Tricks for Robot-Assisted Laparoscopic Radical Cystoprostatectomy and Pelvic Lymph Node Dissection. Chin Evan T and Chin Arnold I. DOI: 10.1089/vid.2017.0050.
Footnotes
Supplementary Video
Click here for Supplementary Video: MALE BB RARC_4.mp4
Author Disclosure Statement
No competing financial interests exist.