
Abstract
Adrenalectomies are increasingly performed using minimally invasive approaches. The widespread adoption of robot-assisted laparoscopy for other urologic surgeries has dramatically increased the popularity of this approach for adrenal surgery.
Indications
Robot-assisted laparoscopic adrenalectomy can be performed for all adrenal lesions, especially with increased surgeon experience (Supplementary Video S1). Broadly, lesions are suspected to be malignant based on size >5 cm. Benign lesions include large symptomatic nonfunctional adenomas, myelolipomas cysts, or functional lesions of any size, including pheochromocytoma, cortisol-secreting adenomas, or aldosterone-secreting adenomas. Malignant lesions most commonly are primary adrenocortical carcinomas or secondary metastases. Especially for less experienced surgeons, open surgery remains an important approach for select indications: large adrenal adenomas, caval involvement, need for concurrent abdominal procedures, anatomic concerns, primary adrenal cancer, and some pheochromocytomas.
Preoperative Preparation
Preoperative preparation hinges on careful operative planning and endocrine management for hormonally active lesions (Supplementary Video S2). For operative planning, computed tomography can assess adrenal anatomy, size, and relation to other structures. Endocrine management is primarily relevant for pheochromocytoma, cortisol-secreting adenoma, and aldosterone-secreting adenomas. Metabolic evaluation for these lesions is mandatory.
Pheochromocytoma classically presents with the clinical triad of sustained hypertension, palpitations, and headache. However, they can also confer no symptoms. Biochemical evaluation includes drawing plasma-free metanephrine and normetanephrines. An irreversible alpha-adrenergic antagonist, phenoxybenzamine, is typically initiated before surgery. The initial dose is 10 mg twice a day, and is up-titrated by 10 mg to a goal normotensive blood pressure. Alternatively, reversible alpha-adrenergic antagonists such as terazosin, doxazosin, or prazosin may be utilized. Beta-blockers can be added to manage tachyarrhythmias. An alternative to alpha antagonists is calcium channel blockers. Importantly, chronic vasoconstriction can result in dehydration, and thus, preoperative fluid repletion can be necessary.
Cortisol-secreting adenomas cause Cushing's syndrome, and can present clinically with weight gain, central adiposity, and virilization. Other effects of excess cortisol can be seen, including hypertension, hirsutism, and abdominal striae. Work-up most commonly involves an overnight low-dose dexamethasone suppression, late night salivary cortisol, or 24-hour urinary-free cortisol testing. Cushing's syndrome is distinguished from Cushing's disease based on a suppressed corticotropin level. Perioperatively, management must include tight electrolyte and glycemic control. Stress dose steroids can be required.
Aldosterone-secreting adenomas, or aldosteronomas classically present with hypertension and hypokalemia, although these are often subclinical. Other stigmata of hyperaldosteronism include alkalosis or elevated aldosterone with concomitant hyponatremia. Before biochemical screening with serum aldosterone and morning aldosterone-to-renin ratio, potassium sparing and mineralocorticoid receptor blocking diuretics should be discontinued for 6 weeks. The confirmatory test is 24-hour urine collection after salt loading. If localization is unclear, adrenal vein sampling can be utilized. Perioperatively, potassium repletion and administration of a potassium sparing diuretic are beneficial.
Patient Positioning
Place a Foley catheter and position the patient in lateral decubitus depending on laterality of the lesion (left side up for left-sided lesions, right side up for right-sided lesions) (Supplementary Video S3). Place an axillary roll and create an incline of 45° to 70° with incline wedges or a beanbag. Flex the table slightly. Secure and pad the upper arm and legs, bending the bottom leg and straightening the upper leg. Secure the chest, waist, and knees using towels and silk tape to prevent movement when the bed is airplaned (Fig. 1).

Robotic right-sided patient positioning.
Surgical Steps
Port placement
Various port configurations can be used. Our configuration is similar to other robotic upper urinary tract procedures (Fig. 2). Initially, mark the camera port 5 cm below the costal margin along the lateral border of the rectus muscle. In obese patients, anatomy can be distorted and it is helpful to rely on the midclavicular line rather than the rectus muscle. Obtain Veress access and insufflation from this site. After insufflation and expansion of the abdomen, the camera port ideally ends 10 cm below the costal margin. Use a 30° camera to examine for injuries and place the remaining ports under vision. Place the upper robotic arm port 8 cm superior to the camera port and the lower arm port angled 90° to 120° from the camera and upper robotic port. These ports should be at least two finger-breadths from the costal margin and anterior superior iliac spine. Place the 12 mm assistant port inferior to the umbilicus. In right-sided cases, a 5 mm port is placed below the xiphoid to accommodate a liver retractor. The fourth robotic arm can be desirable to assist with retraction, especially in obese patients, and can be placed inferiorly to the camera in the midline or lateral border of the rectus muscle. If additional retraction is necessary, another 5 mm assistant port may be placed in the midline between the upper and camera ports. Dock the robot and use bipolar forceps in the left arm, monopolar curved scissors in the right arm, and grasping forceps in the fourth arm.
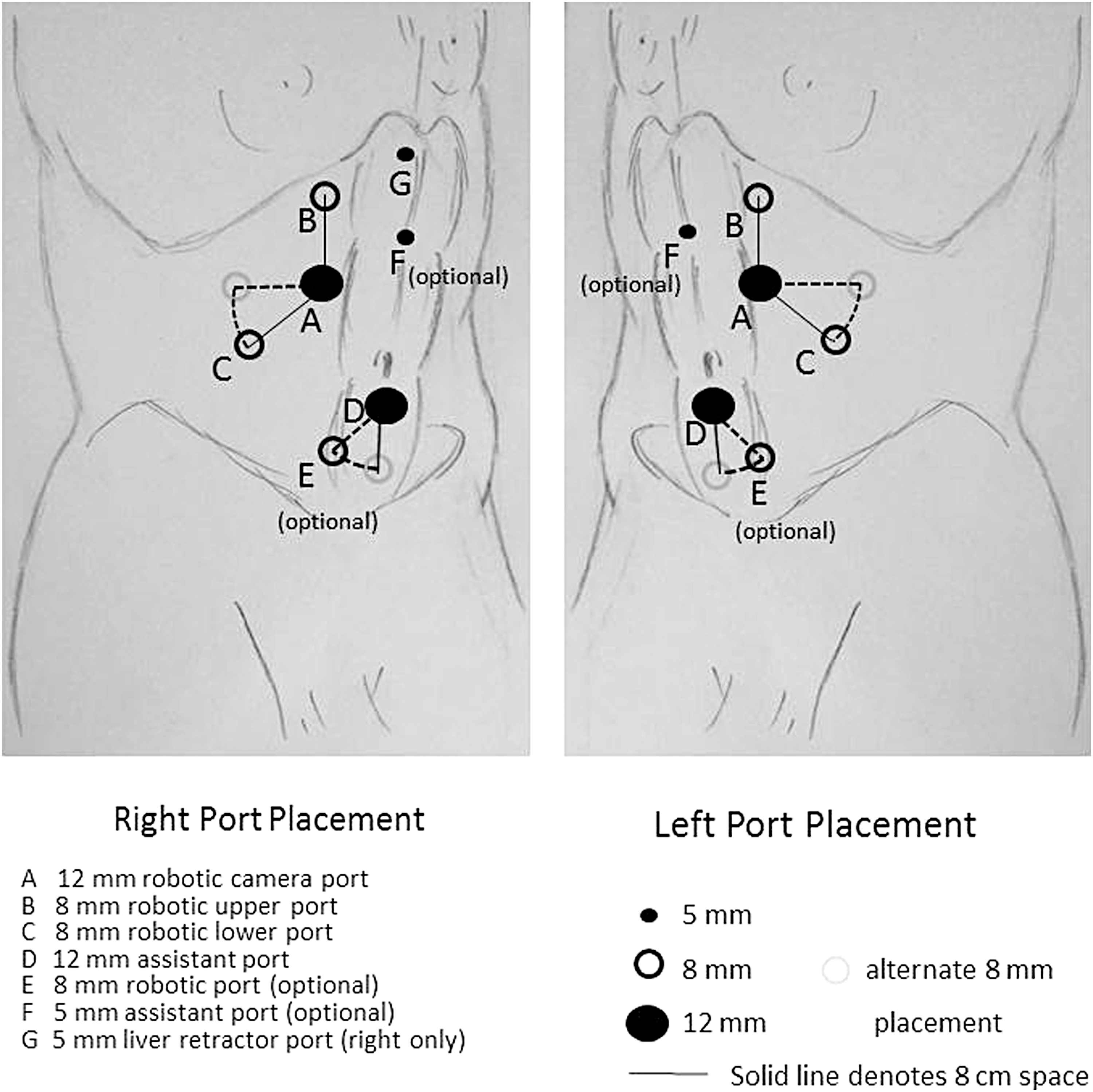
Robotic port placement.
Surgical Steps: Left
Mobilize the colon medially, incising the white line of Toldt (Fig. 3 and Supplementary Video S4). Incise the phrenocolic and lateral splenic attachments to allow the spleen to fall medially and superiorly by its own weight because of gravity (Fig. 4 and Supplementary Video S5). The pancreas is exposed by this maneuver (Fig. 5). Sometimes further mobilization of the colon is needed to completely dissect the spleen medially.
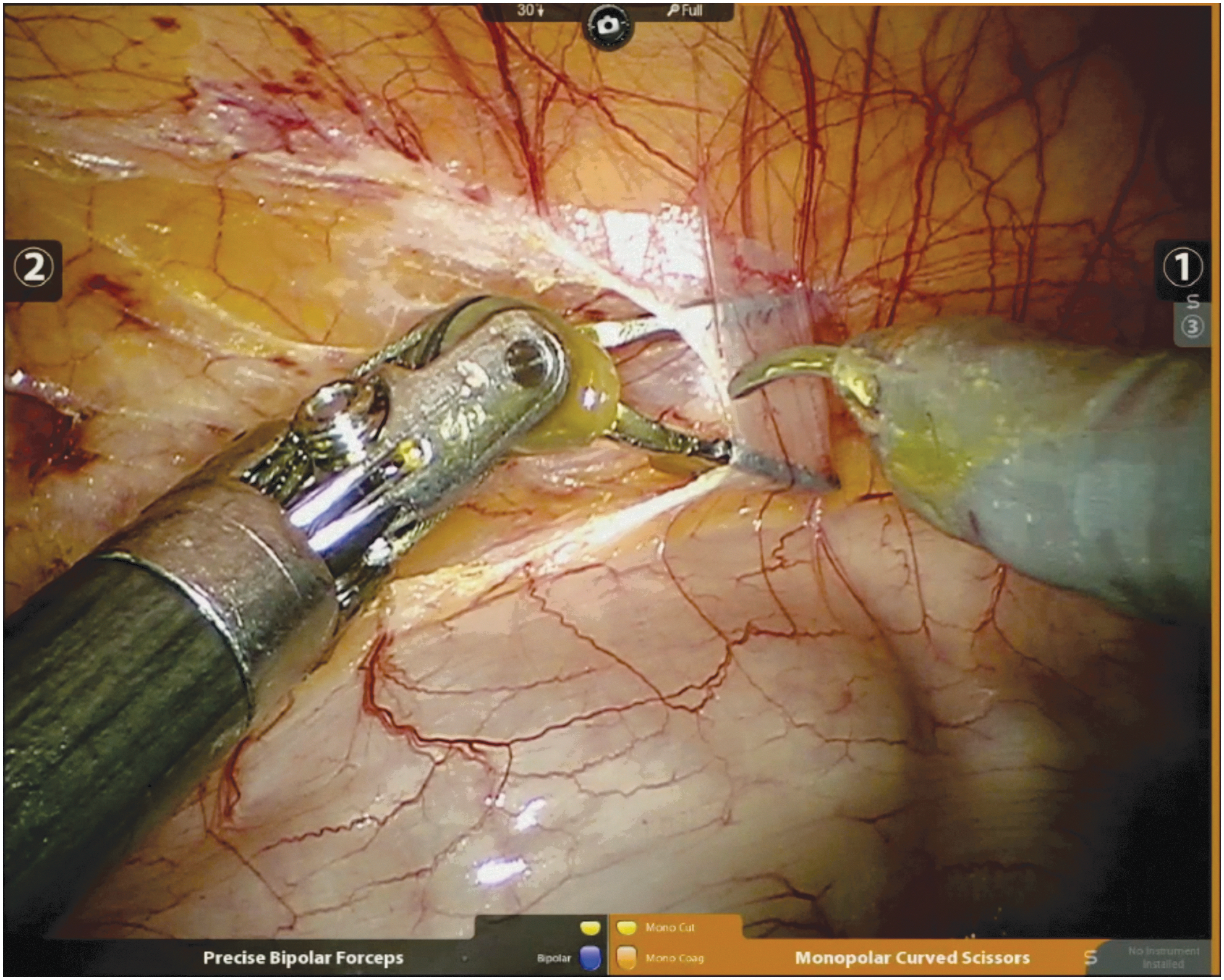
Incise white line of Toldt.
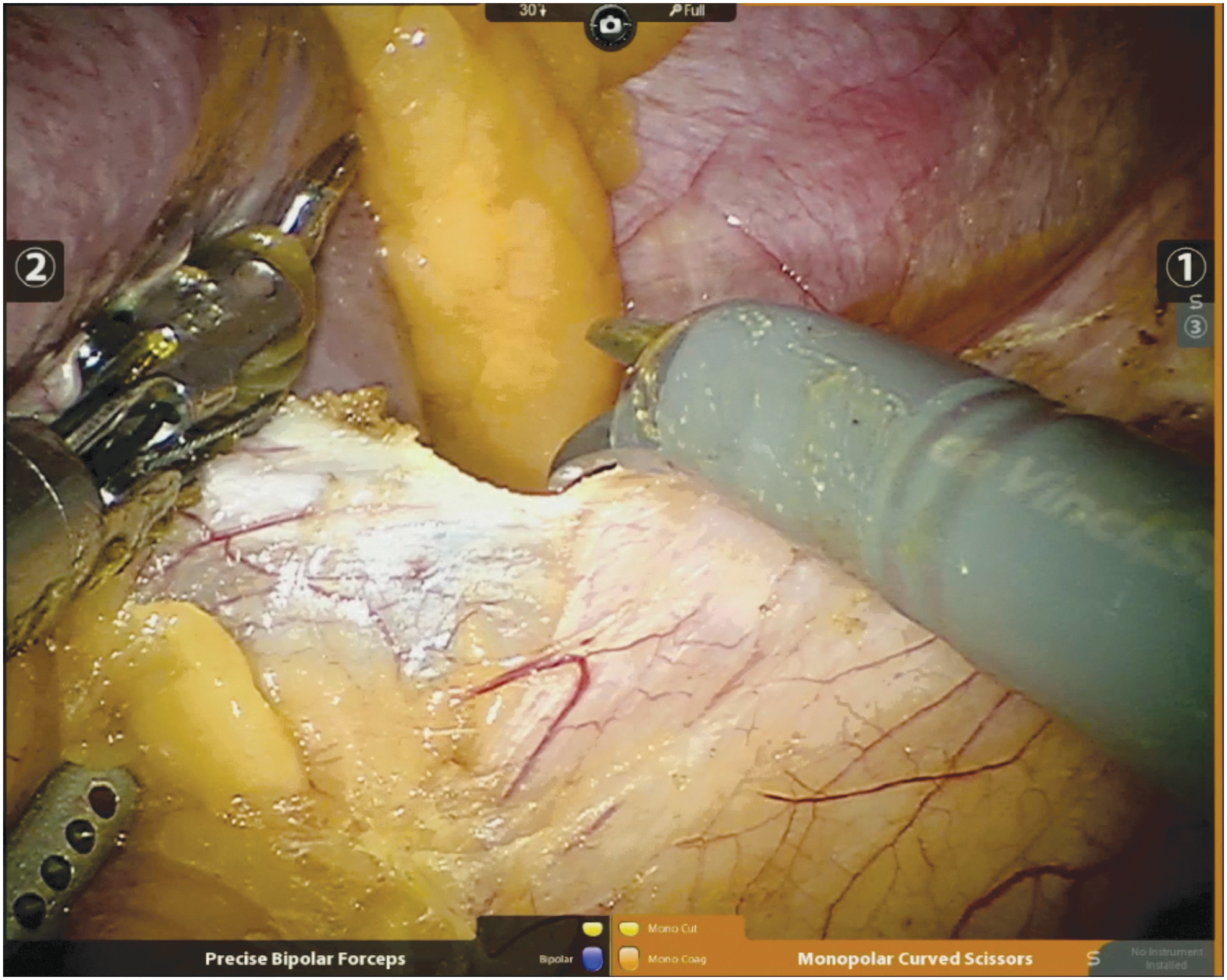
Mobilize spleen medially.
Expose pancreas.
Incise Gerota's fascia above the superior pole of the kidney to begin separating the adrenal gland (Supplementary Video S6). Primarily use bipolar cautery. Focus on the inferior and medial aspects of the adrenal gland, then work laterally to dissect away the kidney. However, it is important to maintain superolateral attachments to Gerota's fascia to keep the adrenal gland tethered and allow for self-retraction (Fig. 6). Use bipolar energy to control small veins and arterial vasculature during this dissection. The anterior and posterior adrenal gland generally has minimal vasculature. Gently retract surrounding fat rather than directly handling the adrenal gland.
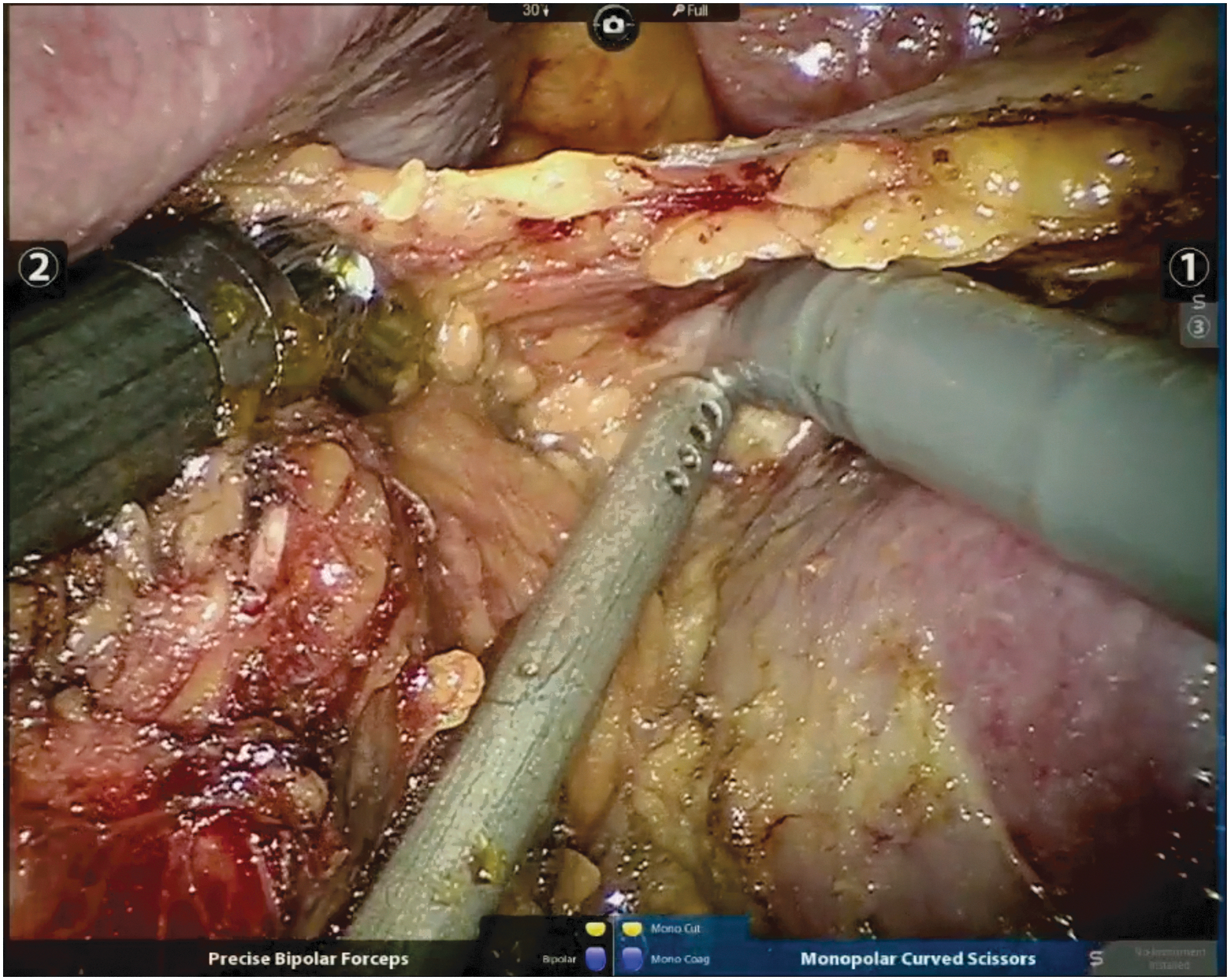
Preserve superolateral attachments.
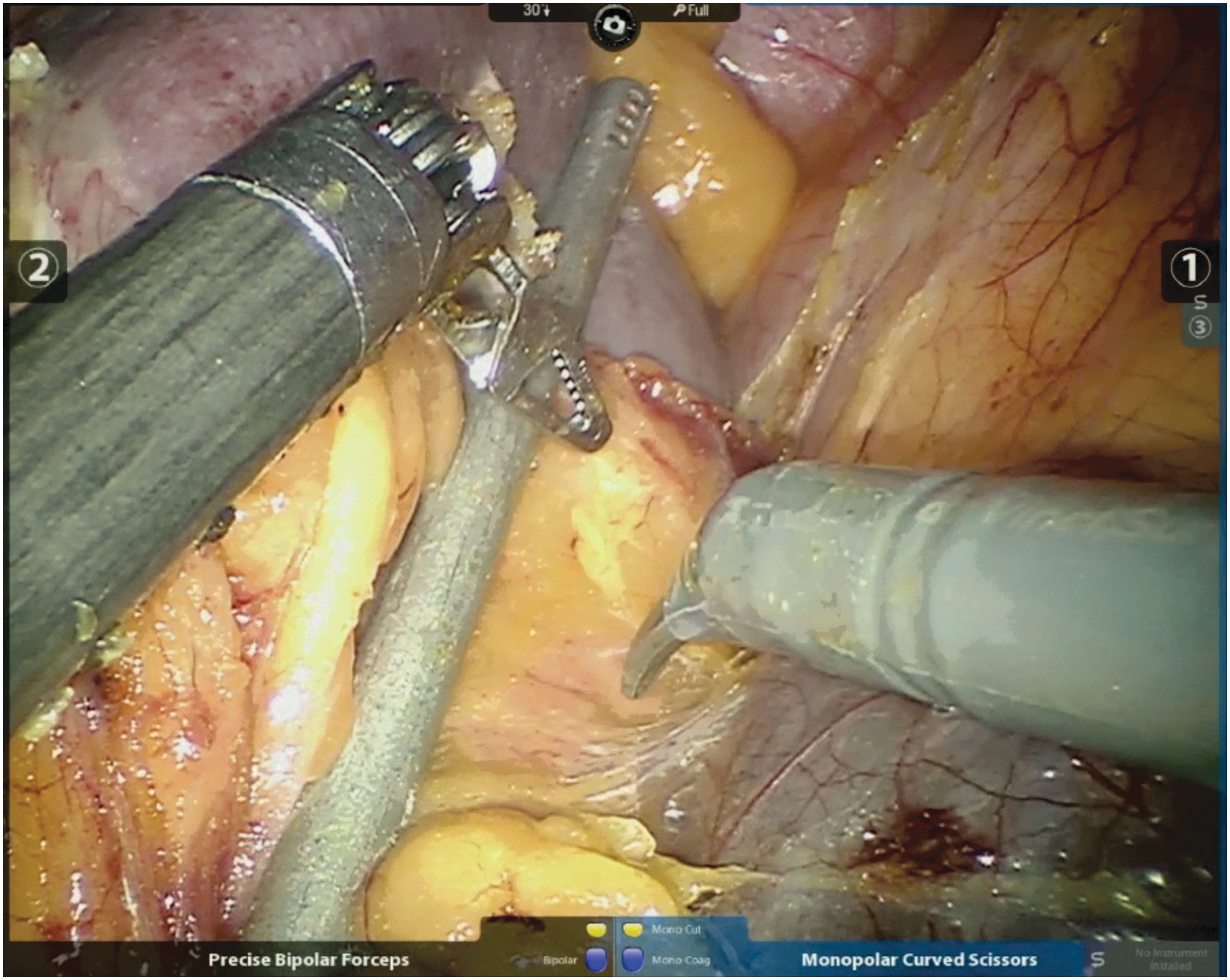
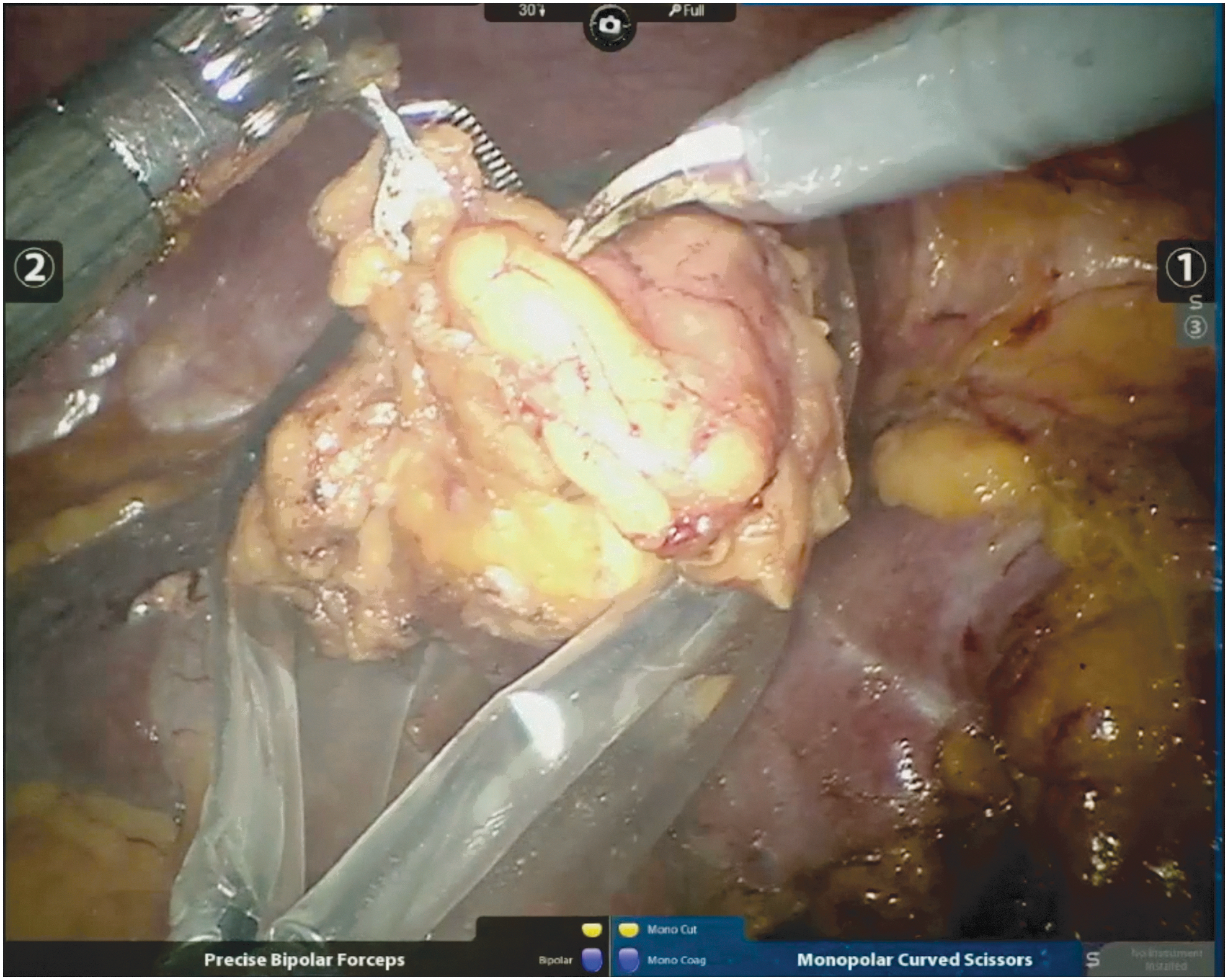
If anatomy is favorable, early control of the adrenal vein is possible, although we recommend initial dissection of the adrenal gland first. Small adrenal veins can be taken using bipolar cautery alone (Fig. 7 and Supplementary Video S7), whereas normal to larger adrenal veins require traditional clips. Place three clips on the adrenal vein and cut between the clips, leaving two clips on the renal vein side.
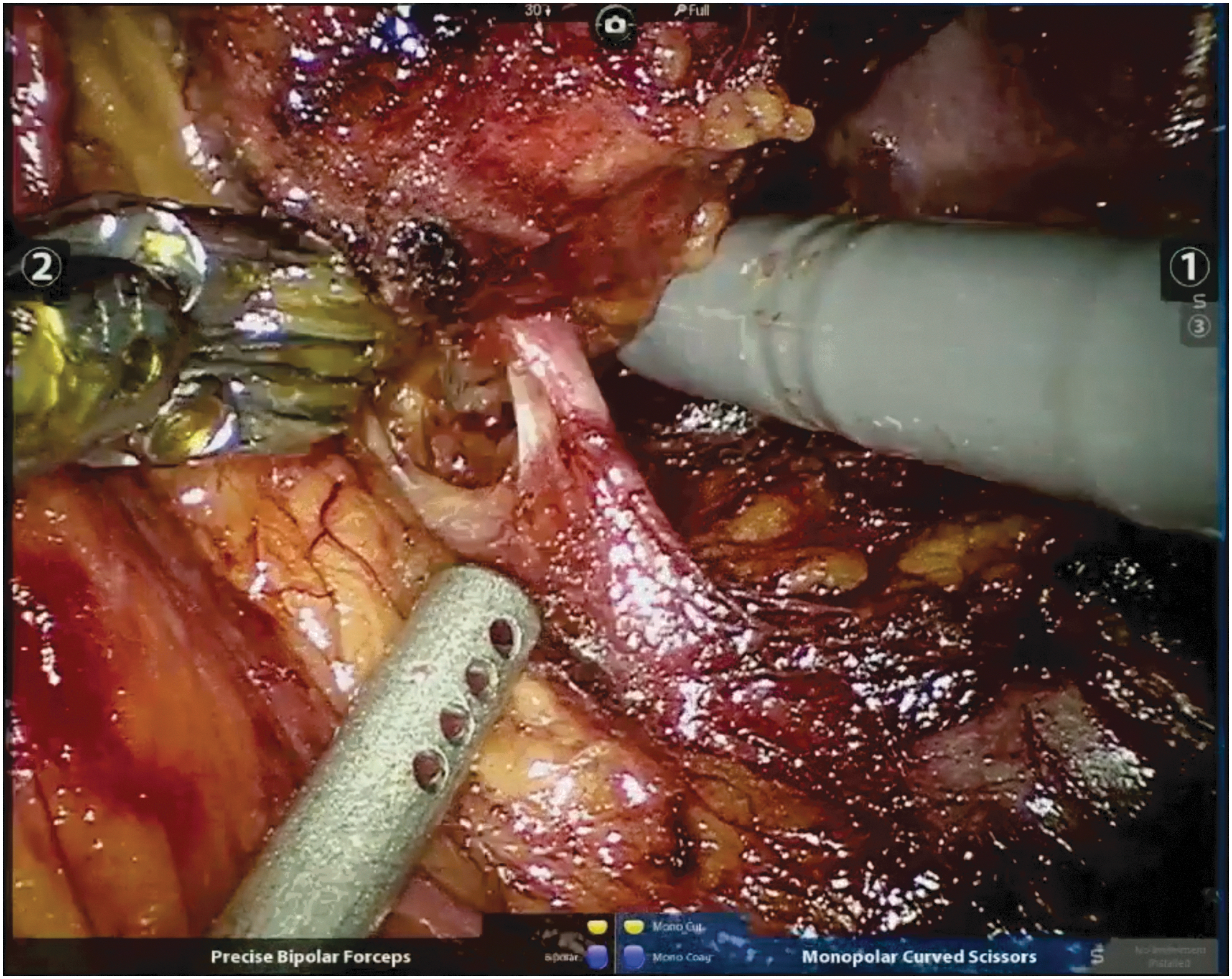
Small adrenal vein.
After the adrenal vein is controlled, complete dissection of the adrenal gland by disconnecting it from Gerota's fascia and remaining superior attachments (Fig. 8 and Supplementary Video S8). Be careful not to transect the superior adrenal gland during this process.
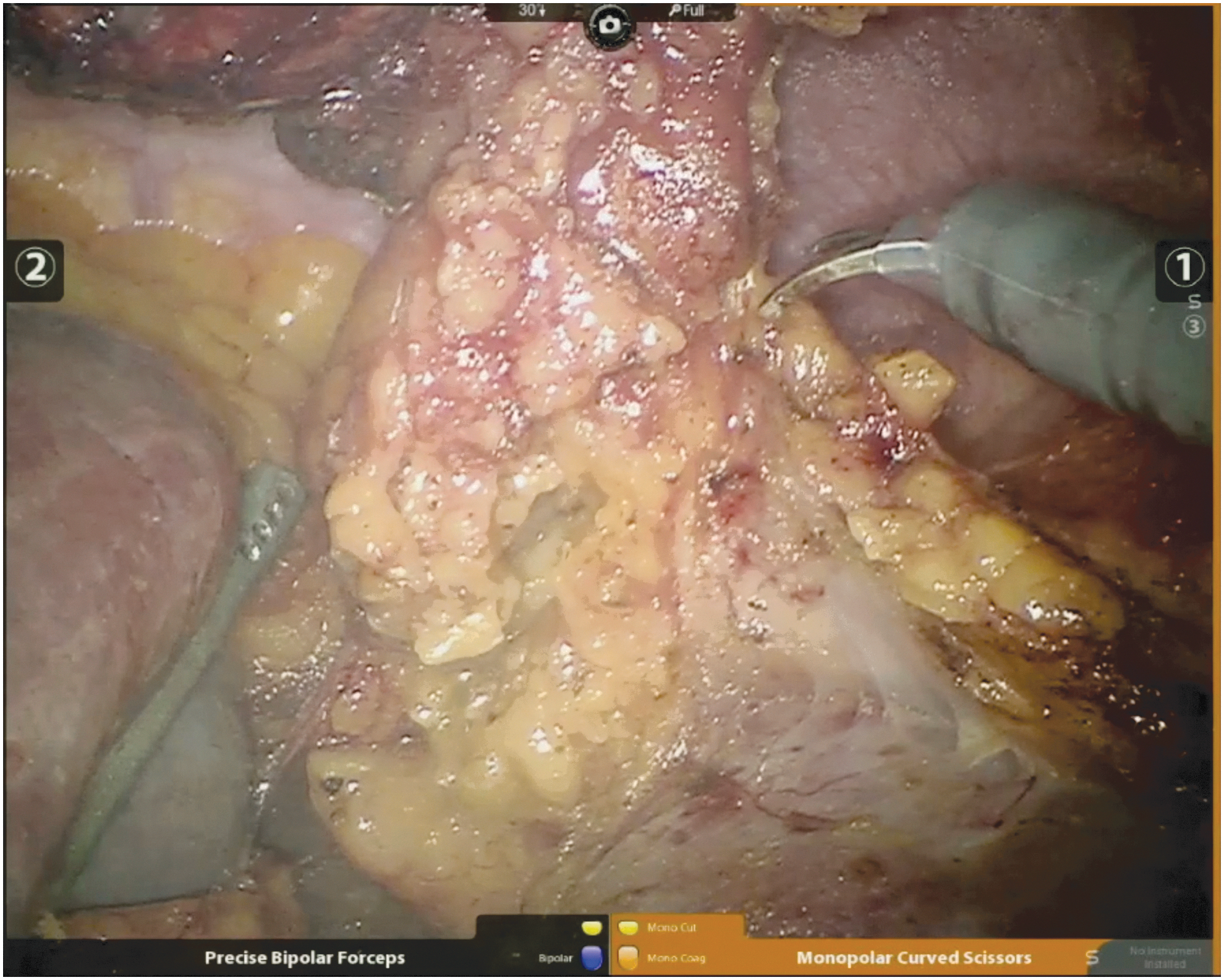
Disconnect superior attachments.
Surgical Steps: Right
First mobilize the liver superiorly by incising the hepatocolic ligament, and place a liver retractor (Fig. 9). Open the peritoneum under the liver arcing medially and inferiorly along the vena cava. Dissect the liver superiorly to expose the adrenal gland. Reposition the liver retractor if necessary. Mobilize the colon medially and kocherize the duodenum if needed. Dissect along the vena cava laterally and posteriorly to expose the medial aspect of the adrenal gland and adrenal vein. Complete adrenal dissection similarly as already discussed for the left-sided case, using clips to control the adrenal vein (Figs. 10 and 11). A caveat for right-sided cases is the unique anatomy of the right adrenal vein. The vein inserts posteriorly and superiorly into the vena cava, increasing the need for careful and meticulous dissection, as bleeding can be difficult to observe and control. Finally, coagulation with argon beam or bipolar energy can be used to control bleeding from the liver.

Liver retraction.

Clip right adrenal vein.
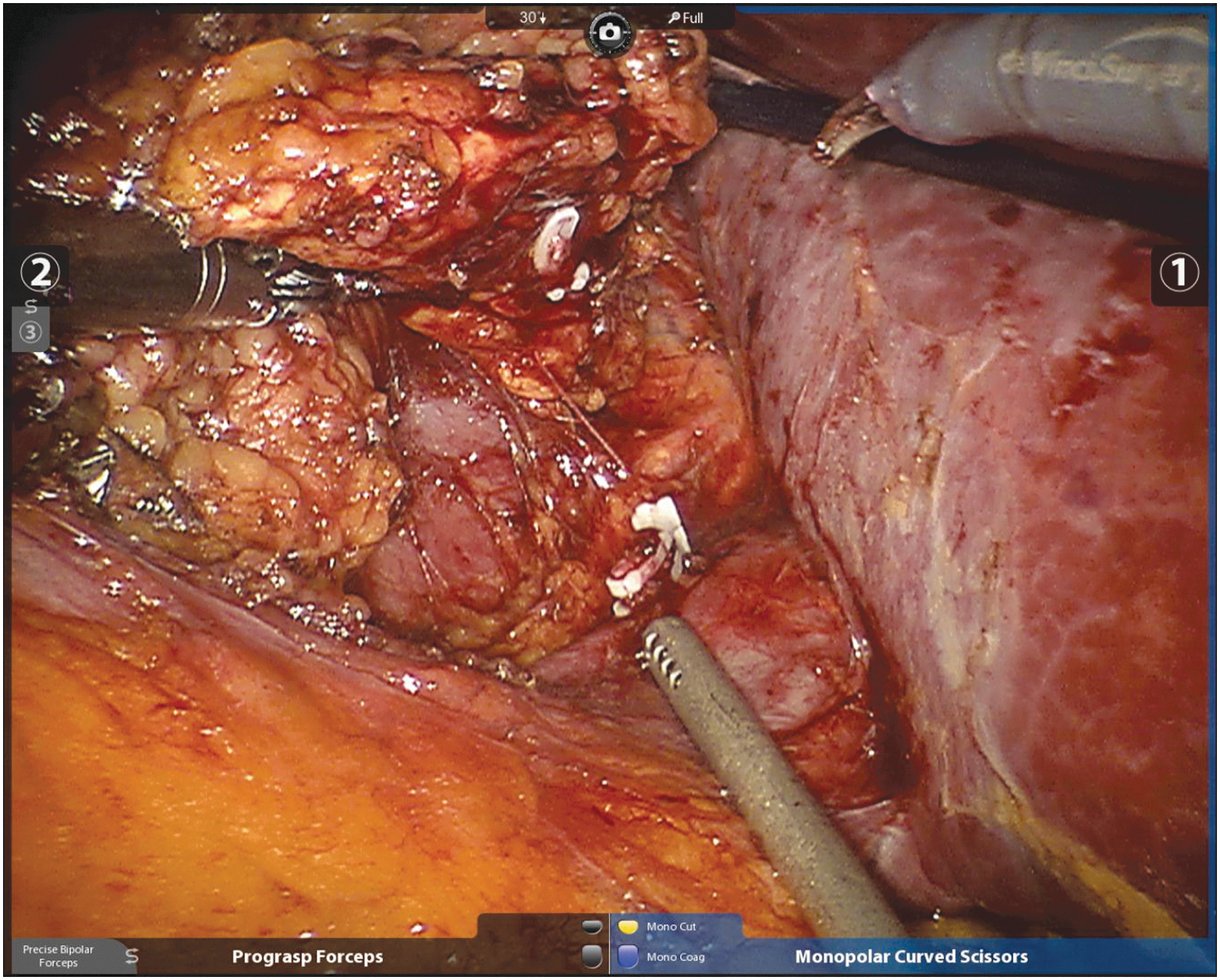
Cut right adrenal vein.
Closure
Place the adrenal gland in a bag (Fig. 12). Remove the specimen through a port site and close the fascia. We routinely reinsufflate the abdomen with 4 mmHg to confirm hemostasis (Fig. 13). Drain placement is not necessary unless concern for injury to associated structures.
Place adrenal gland in bag.

Confirm hemostasis.
Postoperative Care
Patients are routinely admitted overnight. For patients with hormonally active lesions, additional monitoring may be necessary. For pheochromocytomas, monitor for hypotension postoperatively, given preoperative alpha blockade. For cortisol-secreting adenomas, monitor for effects from pre-existing hypercortisolism, including osteoporosis, fracture risk, hyperglycemia, poor wound healing, and increased susceptibility to infections. For aldosterone-secreting adenomas, monitor for persistent hypokalemia. Finally, adrenal insufficiency is a life-threatening condition that may result from inadvertent removal of a solitary adrenal gland, requiring a high index of suspicion. Importantly, hypocortisolism and adrenal insufficiency can occur after adrenalectomy for cortisol-secreting adenomas, even with a structurally normal contralateral adrenal gland, which may require postoperative steroids.
Troubleshooting
Aberrant anatomy
The main arterial supply for the adrenal gland is a ring of small perforating arteries from the inferior phrenic artery, but also branches from the aorta and the renal artery. On the left side, a lateral accessory small vein can be present, draining to the renal vein. Care must be taken to avoid inadvertent ligation of apical branches of the renal artery that can be present near the adrenal gland. On the right side, the adrenal vein can be a challenging source to control bleeding from if injured, and can rarely merge with a hepatic vein. There can also be small arterial branches emerging from posterior to the vena cava.
Obese patients
Port placement must be modified for obese patients (Supplementary Video S9). Reliance on the umbilicus and rectus muscle can result in significantly medially displaced ports. Therefore, use the midclavicular line and costal margin to aid in port placement. Additional fat surrounding the adrenal gland and kidney can make dissection challenging. Observation and correct orientation with a flat horizon are crucial. There should be a low threshold to use additional ports, which can improve exposure.
Intraoperative complications
The most common intraoperative complications during adrenalectomy are injuries to surrounding organs and vasculature. Conceptually, adrenal surgery involves dissection of surrounding organs away from the gland, rather than vice versa. On the left side, care must be taken to avoid injuring the left renal vein, pancreas, and spleen. In the setting of pancreatic injuries, surgical consultation and drain placement are prudent. On the right side, one must be cautious when dissecting near the vena cava, liver, and duodenum. Splenic and liver injuries can generally be managed with pressure and hemostatic agents. Diaphragmatic injuries can result on either side, and can typically be repaired and managed without a chest tube (Supplementary Video S10).
Early venous control for pheochromocytoma
Massive catecholamine release can occur with manipulation of the adrenal gland in the setting of pheochromocytoma, and therefore, early control of the adrenal vein is recommended. Minimal manipulation of the adrenal gland and pheochromocytoma is critical to minimize hypertensive swings. Anesthesiology must be aware before and during control of the adrenal vein. Hypotension commonly occurs in the postoperative phase, especially secondary to lingering preoperative alpha-blockade, and must be monitored for closely. On the left side, the adrenal vein may be found efficiently by following the renal vein and assessing the relationship of the insertion of the gonadal vein. On the right side, careful dissection close to the vena cava will lead to the adrenal vein. To view full video, “Adrenalectomy Final – Arieh L. Shalhav.mp4,” click here.
Footnotes
Author Disclosure Statement
No competing financial interests exist.