
Abstract
Robotic laparoendoscopic single site (RLESS) for upper tract procedures is safe and feasible in the correctly selected patient. An ideal candidate is young, has a low body mass index, and is undergoing surgery for benign indications. For RLESS procedures, we utilize a GelPOINT® access platform for “single-port” placement and ports are configured in a diamond shape. Five millimeter EndoWrist® robotic instruments are placed under direct vision. Range of motion is increased by utilizing the chopstick technique. The surgeon must always be aware of the orientation of each instrument to prevent counter-springing associated with their crossing at the level of the abdominal wall. The robotic camera lens and instruments must be moved synchronously, given their coaxial orientation relative to each other. In this chapter, we describe our technique for two of the most common RLESS upper tract procedures: pyeloplasty and nephrectomy.
Introduction
Current indications for laparoendoscopic single site (LESS) come from the interaction of three main factors: patient body habitus, pathological conditions, and surgeon experience. 1 Indications are broadening as surgical experience improves and new technology is available. In 2009, Kaouk et al. 2 were the first to report the use of the da Vinci Surgical System® (Intuitive Surgical, Sunnyvale, CA) to perform robotic LESS (RLESS) upper tract surgery in humans. With enough experience, procedures such as RLESS nephrectomy and pyeloplasty are safe and feasible in the correctly selected patient.
An ideal candidate is young, has a low body mass index, and is undergoing surgery for benign indications. 1,3 The challenges of RLESS are amplified in obese patients because of specimen weight, abdominal wall restrictions, and distance from the umbilicus. Benign indications for surgery such as pyeloplasty are ideal as there is no specimen removal and thus no need to extend the umbilical incision preserving the RLESS cosmetic advantage. Furthermore, benign indications for nephrectomy are also appropriate for RLESS since the specimen can be morcellated as pathologic analysis is not crucial. Patients confronted with an oncologic diagnosis may be less concerned about cosmesis and, therefore, traditional laparoscopy is preferred to avoid the technical challenges of RLESS. However, if RLESS is desired when there is a malignancy, central intraparenchymal tumors that are smaller and not amenable to partial nephrectomy are ideal for RLESS nephrectomy. 3
Preoperative Preparation
Careful preoperative planning for RLESS upper tract surgery is crucial. Appropriate axial abdominal imaging is mandatory to reduce complications and conversion to standard laparoscopy. Aberrant vasculature at the renal hilum or potential crossing vessels for RLESS pyeloplasty should be identified preoperatively since the ability to control major bleeding is challenging due to range of motion constraints on the surgical assistant. A mechanical bowel preparation is helpful to increase working space and improve exposure. Retrograde pyelography should be considered before RLESS pyeloplasty to determine the extent of ureteropelvic junction (UPJ) stenosis. Placement of a preoperative or intraoperative stent may be detrimental especially to a novice robotic surgeon as the specific site and length of obstruction may be difficult to discern and mobilization of a decompressed renal pelvis can be difficult.
Patient Positioning
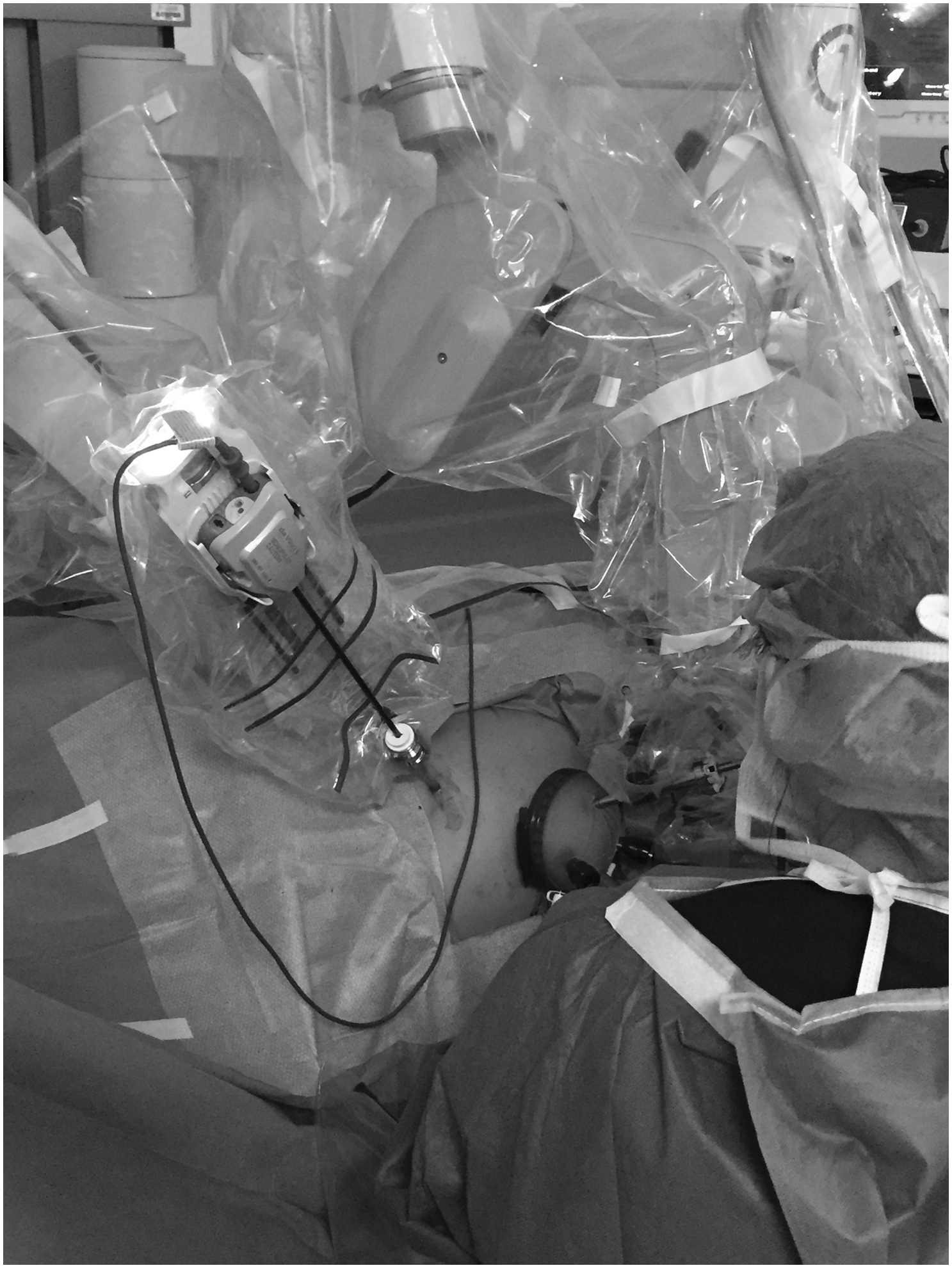
A Foley catheter is inserted before patient positioning. Hair is clipped around the umbilicus as needed. The patient is then positioned in a modified flank at 45° as shown in Figure 1. Foam and tape are used to secure the patient at the chest, hips, and legs. The lower arm is placed on an arm board and secured with tape. The upper arm is rested over the side and padded with foam. Since the fourth arm is not utilized with RLESS, this arm configuration will not interfere with docking. A slight break is made in the table to open the flank for more space. A warming blanket is placed over the hips to keep the patient warm.

The patient is placed in a modified flank position at 45°. The arm can be rested on the side without interfering with robot docking.
Surgical Steps
Access
An open Hasson technique is used to gain entry to the abdomen. The umbilicus is lifted upward with a Kocher clamp. A 15 mm scalpel is used to make a curvilinear incision around the umbilicus. Two stay sutures are placed on both sides of the fascia to help with retraction, and the fascia is scored. The fascial incision is then extended cranially and caudally using Metzenbaum scissors for a length of 2.5 to 3 cm.
Ports
We utilize a GelPOINT® (Applied Medical, Rancho Santa Margarita, CA) access platform for “single-port” placement through our incision. Benefits of these systems include reduced gas leakage, larger extracorporeal profile for port spacing, greater flexibility in port positioning, and the ability to have a small bedside assistant port. 4 An Alexis® wound retractor is placed through the incision and cinched to the abdominal wall. It is important to thoroughly sweep underneath the retractor to make sure no omentum or small bowel gets trapped. This can be confirmed visually using a laparoscopic camera. An instrument shield is placed. The system incorporates 10 mm sleeves, which function as ports, and are placed through the GelSeal® cap in a customizable configuration. We utilize a diamond-shaped configuration (Fig. 2) with an 8.5 mm trocar for the camera at 12 o'clock position, the two 10 mm purple sleeves at 3 and 9 o'clock positions, and a 12 mm AirSeal® (CONMED, Utica, NY) port at 6 o'clock position. The AirSeal is placed for the assistant and prevents loss of pneumoperitoneum. The GelSeal Cap is secured to the retractor, forming a tight seal and preventing any additional gas leakage.

A diamond-shaped configuration is made with an 8 mm camera at 12 o'clock position, two 10 mm purple sleeves at 3 and 9 o'clock positions, and a 12 mm AirSeal® port at 6 o'clock position. The ports are placed through the GelSeal® cap first and then the cap is secured onto the retractor.
Robot docking
Maximizing instrument mobility is key and involves placing the robotic arm and camera ports slightly staggered from one another as well as the use of a 30° lens in the “up” position, which allows the camera to reside inferior to the working arms inside the patient. 5 We use a da Vinci Si robot that has smaller profile robotic arms than earlier generations, helping to reduce external clashing. The Xi has an even smaller arm profile that could be quite beneficial. Five millimeter flared trocars are predocked onto the robot arms (Fig. 3) and telescoped through the sleeves. The 5 mm robotic instruments are inserted under direct vision. Initial dissection is started with the EndoWrist® Maryland dissector and monopolar hook cautery. These 5 mm instruments have additional articulation at the wrists compared with the 8 mm robotic instruments. Range of motion is increased by the “chopstick” technique described by Joseph et al., 6 wherein crisscrossed instruments are reprogrammed for intuitive instrument control such that the left instrument is controlled by the right hand effector and vice versa.

The robot camera port is docked. The other arms of the robot are preloaded with 5 mm flared trocars. The trocars are then telescoped through the 10 mm sleeves on the GelPOINT.
RLESS nephrectomy
The procedure is started by mobilizing the colon medially and exposing the retroperitoneum. The robotic camera lens and instruments must be moved synchronously, given their coaxial orientation relative to each other. The assistant can help retract the colon as needed with the suction device. Gerota's fascia can be lifted upward with the Maryland and bowel can be swept medially until the gonadal vein is identified. An incision is made into Gerota's fascia and the ureter and kidney are swept up and off the psoas muscle. During dissection, it is often necessary to transpose the left- and right-handed instruments (switch which one is on top and bottom), to maximize retraction.
For a left-sided nephrectomy, the instruments are switched at this point to use the Maryland in the right hand (left arm) to lift the kidney and the hook cautery in the left hand (right arm) to complete dissection. With the kidney elevated, hook cautery dissection is performed in the cephalad direction to access the hilum (Fig. 4). The vessels can be clipped with Hem-o-lok® clips placed by the assistant and then transected with the hook cautery. Alternatively, the hilum can be taken en bloc using an endovascular stapler controlled by the assistant. Remaining attachments to the upper pole are ligated. The tail of Gerota's fascia can be cauterized or stapled. Sometimes for benign indications, patients may have a stent in place and it should be identified and removed through the assistant port. A clip can be placed on the distal end of the ureter and then the ureter is transected above the clip. All lateral attachments to the side wall are transected with cautery until the specimen is completely free. At this point, pressure should be dropped to 5 mmHg and hemostasis confirmed.
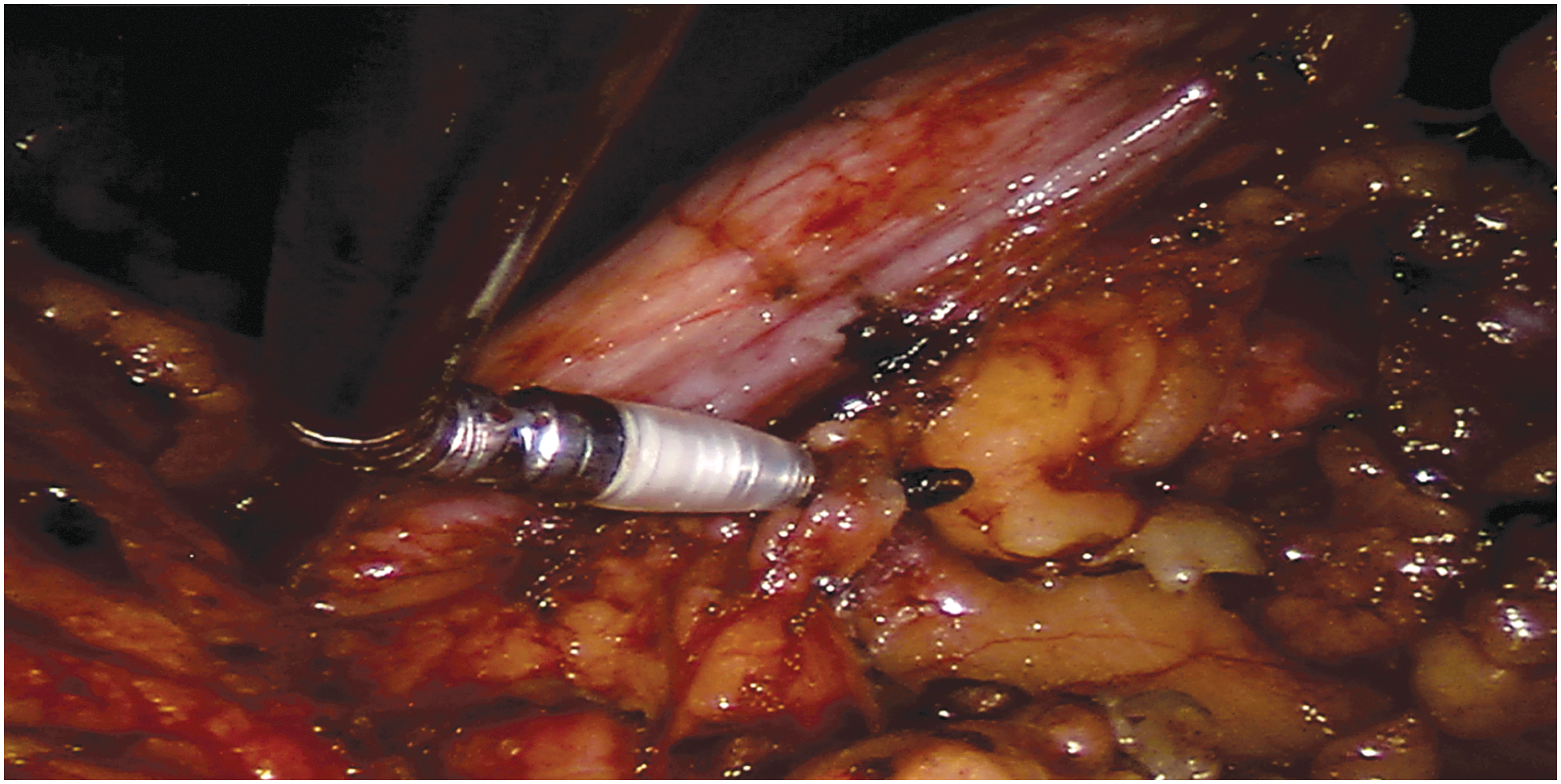
Using the Maryland to elevate the kidney, hook cautery dissection is performed in the cephalad direction toward the hilum.
The specimen is then placed in an Endo Catch bag and the robotic system is undocked. The GelPOINT and trocars are then removed from the umbilicus and then the specimen itself should be extracted through the umbilical incision. Usually, a benign hydronephrotic nonfunctioning kidney can be removed without further need to extend the incision. The fascia is closed with #1 polydioxanone. Skin is then closed with 4-0 poliglecaprone 25 followed by a liquid topical adhesive.
RLESS pyeloplasty
The procedure is commenced similarly to RLESS nephrectomy by mobilizing the colon medially and exposing the retroperitoneum. The ureter and renal pelvis are identified and mobilized. If present, crossing vessels are dissected and preserved, and the ureter and renal pelvis are circumferentially dissected posterior to the crossing vessels using a combination of cautery and blunt dissection. A sufficient amount of ureter and renal pelvis that would enable a tension-free anastomosis after UPJ dismemberment is mobilized. The ureter is sharply transected above the level of obstruction, and any abnormal segment of the UPJ is excised, care being taken to avoid cutting a preplaced stent. Next the renal pelvis and ureter are then both spatulated for approximately 1.5 cm, cutting the ureter along its lateral aspect. The instruments are then exchanged for two 5-mm robotic needle drivers.
We prefer to place a stent at this point during the procedure. An angiographic catheter is introduced subcostally and a Amplatz ultra stiff wire is advanced down the ureter through the ureterotomy and into the bladder in an antegrade manner. A 6F Double-J stent is then advanced over the wire to curl in the bladder. The anastomosis is started with a running 4-0 polyglactin suture to the posterior aspect. Once completed, the proximal curl of the stent is placed in the renal pelvis and the anterior aspect of the anastomosis is completed with another running 4-0 polyglactin suture. A 19F round drain is positioned lateral to the anastomosis and is retroperitonealized by reapproximating the colon to the lateral abdominal wall using Hem-o-lok clips. The GelPOINT and trocars are then removed from the umbilicus. The fascia is closed with #1 polydioxanone. Skin is then closed with 4-0 poliglecaprone 25 followed by a liquid topical adhesive.
Postoperative Care
Patients are admitted for overnight observation. Immediately after surgery, patients can have a clear liquid diet and advance to regular diet the following morning as tolerated. The patient is encouraged to ambulate as soon as possible after surgery. The Foley catheter is removed in the morning on postoperative day 1. For pyeloplasty, a drain creatinine level is checked after Foley catheter removal. If consistent with serum, the drain is removed as well. The ureteral stent is usually maintained for 4 weeks postoperatively and the patient is maintained on daily antibiotic prophylaxis during that period. Diuretic renogram is usually obtained 6 to 8 weeks after stent removal. Patients may resume normal activities after 2 weeks.
Any deviation from the normal postoperative course should be highly suspicious. We recommend all RLESS procedures be recorded and easily retrieved for review. Intraoperative complications may not be recognized until the postoperative period and reviewing the recorded video of the procedure may identify a critical error. CT evaluation should be requested when the patient's clinical status (pain, fever, leukocytosis, or decreasing hematocrit) cannot be explained by physical examination or routine clinical studies. 7 CT is the study of choice when evaluating a patient for decreasing hematocrit as it can help localize the site of bleeding. During early surgeon experience in RLESS pyeloplasty, certain postoperative complications may be noted more frequently, namely urine leak and ureteral obstruction. Interestingly, lower rates of urine leak are seen in RLESS pyeloplasty 8,9 than in conventional robot-assisted laparoscopic pyeloplasty 10,11 series. This is likely attributed to lower number of RLESS cases and highly experienced surgeons. Nonetheless, urine leak is associated with future pyeloplasty failure and should be managed urgently.
Troubleshooting
Although the adaptability of the robot has certainly helped improve the technical ease of LESS, the procedure is not without its own challenges. The robotic platform and instruments that we describe for our technique are not specifically designed for LESS surgery. The recent purpose-built da Vinci model SP1098 single-port robotic platform may help further eliminate some of the challenges such as clashing and triangulation. 12
Meticulous attention is paid to scaling down the degree of excursion of the instruments relative to the camera with each move. The chief limitation with the “chopstick” technique is the increase in intra-abdominal arm clashing at the point of crossing at the abdominal wall. 13 To prevent this, the surgeon must always be aware of the orientation of each instrument to prevent counter-springing associated with their crossing at the level of the abdominal wall. It is also important to anticipate the track of the surgical assistant's instruments to prevent clashing. Learning to use the assistant for retraction is advantageous as the fourth robotic arm is not employed. Judicious use of cautery is important to maintain hemostasis throughout the procedure as the assistant is only able to provide limited help given the space constraints at the bedside.
If the spleen or liver cannot be retracted adequately, an additional 3 mm trocar with grasper can be placed outside of the incision to retract the organ. If significant intraoperative hemorrhage is encountered, additional trocars or open conversion may be required. Failure to progress can be another reason for conversion from RLESS, especially in one's early experience. Placement of an additional trocar (Fig. 5) can salvage the minimally invasive benefit. Supplementary Video S1 available online at
Conversion from RLESS is sometimes required from failure to progress. In this case, an additional 5 mm trocar is inserted for the left arm. RLESS = robotic laparoendoscopic single site.
Recommended Videos from Videourology
1. Gahan JC, Stewart JW, Garcia-Gil M, Cadeddu JA. Robotic Single-Site Pyeloplasty Using Crossed Articulating Instruments and 5 mm Flared Cannulas. March 2015, 29.
2. Imkamp F, Kuczyk M, Nagele U, Herrmann TR. Single-Incision Pyeloplasty—As Feasible As Laparoscopic Pyeloplasty? Results of the Initial Nine Cases. Journal of Endourology Part B, Videourology. May 2013, 27.
Footnotes
Supplementary Videos
Click here for Supplementary Videos: RLESS Video_HI_VER2 NEW.mp4; RLESS Video_Part 1 positioning and setup_HI.mp4; RLESS Video_Part 2 Nephrectomy_HI.mp4; RLESS Video_Part 3 pyeloplasty_HI.mp4
Author Disclosure Statement
No competing financial interests exist.