
Abstract
Background:
Cryoablation has emerged as an alternative to the more invasive partial nephrectomy for small renal masses. The approach can be carried out by two techniques, either laparoscopic cryoablation (LCA) or percutaneous cryoablation, (PCA) with CT guidance. We aimed to compare between the two procedures.
Materials and Methods:
A systematic review and meta-analysis was conducted, including studies comparing the two techniques. Outcomes included incomplete ablation, late local recurrence, cancer-specific survival, procedure time, transfusion rates, hospital stay, and complications.
Results:
A total of 1475 patients were included, 788 patients in the laparoscopic group and 687 patients in the percutaneous group. There was statistical difference favoring the laparoscopic group with regard to having less incomplete ablation (p = 0.0008) and higher cancer-specific survival patients (p = 0.04). However, there was longer hospital stays in the LCA group (p < 0.00001) and was found to be more costly than the PCA group. There was significantly more Clavien-I complications in the PCA group (p = 0.001) and more Clavien-III complications in the LCA group (p = 0.001). Otherwise, there were no differences in any other outcome parameter.
Conclusion:
LCA was found to have less incomplete tumor ablation rates and higher cancer-specific survival rates, however, higher hospitalization time, more major complications (Clavien III), and was costlier compared with PCA.
Background
R
Partial nephrectomy is the standard of care for the management of T1a renal tumors. 3 It offers the benefit of renal function preservation and solid local cancer control and with minimally invasive techniques offer less morbidity. 4,5 Ablative therapies have emerged as an alternative treatment modality to partial nephrectomy. Renal tumors are treated in situ by a heating or freezing technique. Ablative treatment is minimally invasive, associated with fewer complications, shorter hospitalization time, and quicker recovery compared to partial nephrectomy. 6
Cryoablation uses subzero temperatures to destroy cancer cells through direct injury caused by ice crystals formation and microcirculatory failure. 5,7 Renal cryoablation has evolved considerably since it was first used to treat renal cell tumors over 20 years ago. It is performed through a laparoscopic cryoablation (LCA) or percutaneous cryoablation (PCA) image-guided approach. The purported advantages of percutaneous approach over LCA are short hospitalization time, faster recovery, less pain relief requirement, and reduced cost, with a comparable oncologic outcome. 4,5 This has led more centers to adopt PCA rather than LCA.
In this systematic review and meta-analysis, we reviewed the contemporary literature to compare the outcome, complications, and cost of both laparoscopic and percutaneous image-guided cryoablation to treat small renal masses. We only included comparative studies of both procedures to reduce the risk of bias, as opposed to conduct a comparison of reported series of individual procedures.
Methodology
Search strategy and study selection
A review of the literature and meta-analysis was conducted using Cochrane guidelines and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist.
8,9
The search strategy was conducted to find studies for inclusion using the following databases MEDLINE (1990–May 2017), EMBASE (1990–May 2017), Cochrane Central Register of Controlled Trials—CENTRAL (in The Cochrane Library—Issue 1, 2017),
Search terms used included: “renal masses,” “percutaneous,” “renal tumors,” “Laparoscopic,” “Laparoscopy,” “cryotherapy,” and “cryoablation.”
Mesh phrases included:
(“Kidney Neoplasms‘[Mesh]) AND’ Cryotherapy”[Mesh])
((“Cryotherapy”[Mesh]) AND “Tomography, X-Ray Computed”[Mesh]) AND “Laparoscopy”[Mesh]
((“Laparoscopy”[Mesh]) AND “Cryotherapy”[Mesh]) AND “Kidney Neoplasms”[Mesh]))
Studies in languages other than English were included if data were extractable. If data were not provided or clarified and the data were not extractable, the study was excluded.
Two reviewers (O.A. and M.I.) identified all studies that appeared to fit the inclusion criteria for full review. Two reviewers (O.A. and M.I.) independently selected studies for inclusion in the review. Any disagreements were referred to a third reviewer (F.X.K.).
Data extraction and analysis
All studies comparing laparoscopic cryotherapy to percutaneous CT-guided cryotherapy for small renal masses were included. The primary outcome was to assess the difference between the two procedures regarding oncologic outcomes: incomplete ablation, late local recurrence, and cancer-specific survival. Secondary outcomes were to assess the procedure-related outcomes: operative time, transfusion rates, hospital stay, and complications.
We defined residual tumor or incomplete ablated tumor as an enhancing lesion at the site of ablation on the first postoperative CT scan, while late local recurrence was defined as enhancing lesion at the site of ablation following at least one contrast CT scan showing no residual tumor.
Results that were pooled from the included studies were meta-analyzed. For continuous data, a Mantel–Haenszel Chi-square test was used and expressed as the mean difference with 95%CI, and for dichotomous data, an Inverse Variance was used and expressed as risk ratio with 95%CI. In both cases, p < 0.05 was considered significant. 8,10
Heterogeneity was analyzed using a Chi-square test on N-1 degrees of freedom, with an alpha of 0.05 used for statistical significance and with the I2 test. 8,10 I2 values of 25%, 50%, and 75% correspond to low, medium, and high levels of heterogeneity. A fixed-effect model was used unless statistically significant high heterogeneity (I2 > 75% was considered as significantly high heterogeneity) existed between studies. A random-effects model was used if heterogeneity existed.
An assessment of the methodologic quality of the included studies into the meta-analysis was conducted in line with the Cochrane handbook. 8,10 Review Manager (RevMan 5.3) was used to plot the quality assessment.
Results
The literature search yielded 128 studies, of which 109 were excluded due to nonrelevance based on titles and abstracts (Fig. 1). Full articles were evaluated in 19 studies, of which, 12 were included into the systematic review. 11 –22 Of the 12 studies included, 6 were from same centers, 11 –13,15,17,20 therefore, their data were only included if unique to that study, therefore reducing the actual number of studies with extractable data to 8. All the included studies were published within the last 8 years.

Flowchart for article selection process of the review.
All the included studies were retrospective cohort comparative studies with no randomization and all reported on individual center's experience with laparoscopic and percutaneous cryotherapy.
Characteristics of the included studies
Although literature search was conducted between 1990 and 2016, comparison studies were published between 2008 and 2015, all of which were from centers in the United States, and the majority of the studies were single-center studies. 11,12,14 –17,19,21,22
In total, there were 1475 patients, 788 patients (age range of 56–80 years) in the LCA group and 687 patients (age range of 56–82 years) in the PCA group (Table 1). Four studies included patients with masses only <3 cm, 16,18,19,22 while one included masses <7 cm in size, 21 and the remaining included patients with masses <4 cm in size.
The borderless tables represent studies with data from the same centers. There, data used once were available.
BMI, body mass index; PCA = percutaneous cryoablation; LCA = laparoscopic cryoablation; NS = not stated.
Although all the studies reported on the patients and procedure demographics, only four studies depicted the data for inclusion into a meta-analysis for age, 15,16,20,22 six for sex, 13,15,16,19,21,22 three for body mass index (BMI), 16,20,22 and four for tumor size. 15,16,18,20
Figure 2 depicts the studies that reported on the oncologic outcome measures. All studies reported on incomplete ablation, five on late local recurrence rates, 15,16,18,20,22 four on cancer-specific survivals, 12,18,20,22 and all studies reported the 5-year recurrence-free survivals, however, only two studies had extractable data. 16,22
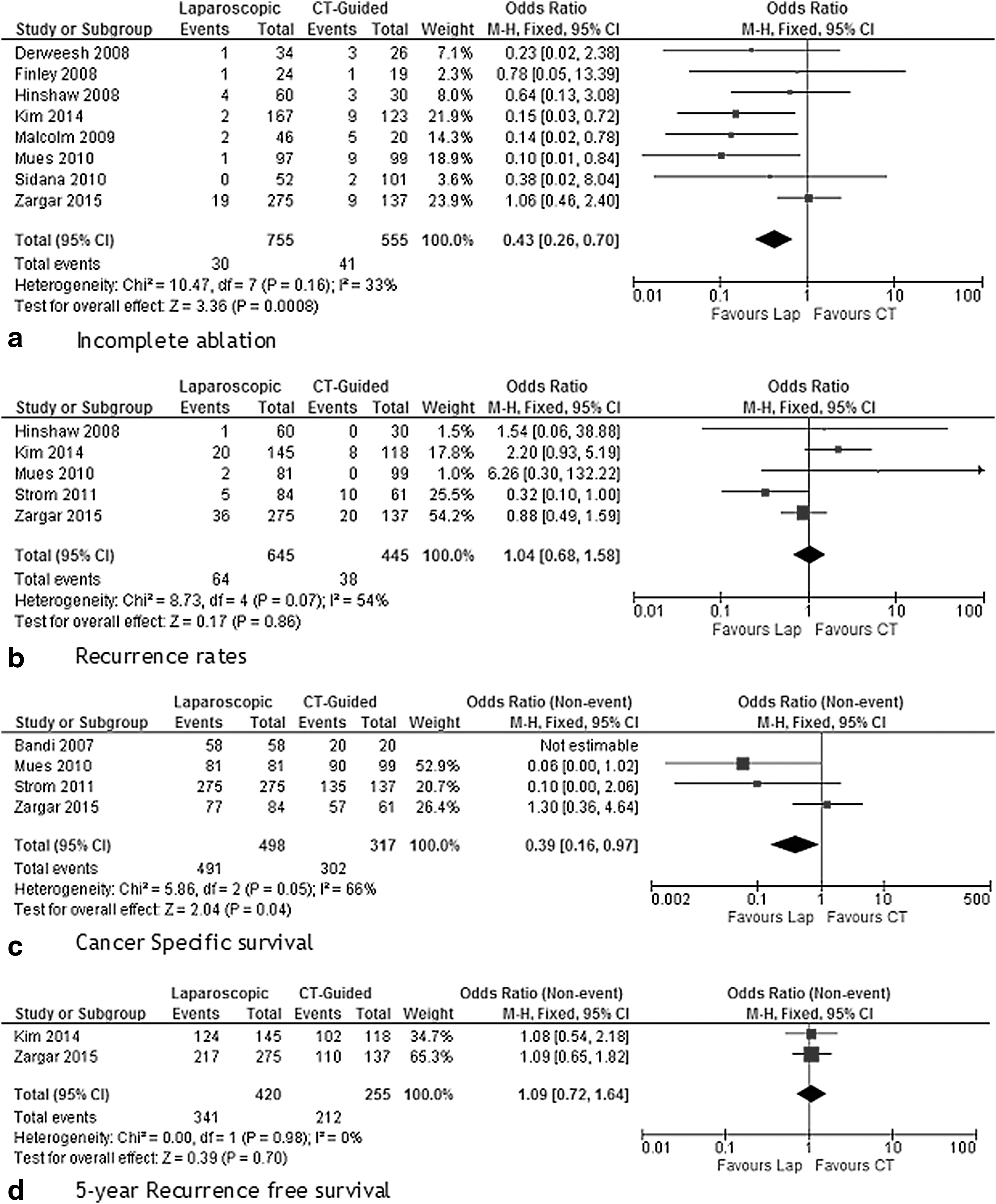
Oncologic outcomes.
All the studies reported on complications of the procedures; however, only six studies classified the complications into the Clavien–Dindo classification (Fig. 3). 14,16,19 –22

Comparison between LCT and PCT
Meta-analysis results
The patients' age ranged between 55 and 82 years with no difference between the two groups, furthermore, there was no difference between the two groups regarding age, sex, or tumor size. However, in the studies that report on BMI, there were higher BMI patients in the PCA group (p = 0.001 MD: −1.79, 95% CI: −2.86, −0.72).
There was statistical difference favoring the laparoscopic group with regard to having less incomplete ablation (p = 0.0008; OR: 0.43, 95% CI: 0.26, 0.7) and higher cancer-specific survival (p = 0.04; odds ratio [OR]: 0.39, 95% CI: 0.16, 0.97). However, there was no difference between the two groups with regard to late local recurrence rates (p = 0.86; OR: 1.04, 95% CI: 0.68, 1.58) and 5-year recurrence-free survival (p = 0.7; OR: 1.09, 95% CI: 0.72, 1.64).
Regarding the incomplete ablations: in total, 3.9% (30/755) of the LCA and 7.4% (41/555) of the PCA patients had incomplete tumor ablations. Of these, 37 of the 41 patients with incomplete PCA ablations had effective repeated PCA, 3 had radical nephrectomies, and 1 went on to active surveillance. One of the radical nephrectomy patients had the PCA repeated before his nephrectomy and the tumor remained incompletely ablated, leading to a nephrectomy. In the LCA group, the 30 patients with incomplete ablation underwent a variety of procedures: 10 had effective PCA, 3 nephrectomies, 11 active surveillances, and 2 partial nephrectomies, while 1 patient died of an unrelated illness before any subsequent treatment.
There was no statistical difference between the two groups regarding overall complications (lap: 81/786 vs CT: 98/677) (p = 0.46; OR: 0.88, 95% CI: 0.63, 1.23), CD-II complications (lap: 26/647 vs CT: 16/558) (p = 0.16; OR: 1.6, 95% CI: 0.83, 3.08), or CD-IV complications (lap: 5/647 vs CT: 4/558) (p = 0.59; OR: 1.39, 95% CI: 0.42, 4.64). However, there were significantly more CD-I complications in the PCA group (lap: 3.3% [21/647] vs CT: 9.1% [51/558]) (p = 0.001; OR: 0.4, 95% CI: 0.23, 0.7) and more CD-III complications in the laparoscopy group (lap: 3.9% [25/647] vs CT: 1.1% [6/558]) (p = 0.001; OR: 3.99, 95% CI: 1.72, 9.28).
The studies that reported on metastasis found no difference between the two groups (lap: 0.9% [3/335] vs CT: 1.2% [2/167]) (p = 0.75; OR: 0.74, 95% CI: 0.12, 4.51). There was no difference regarding transfusion rates (lap: 2.3% [6/258] vs CT: 2.6% [5/192]) (p = 0.94; OR: 0.1.04, 95% CI: 0.32, 3.41), however, there was shorter length of hospital stay in the PCA group (PCA mean stay: 1 vs LCA mean stay 3) (p < 0.00001; MD: 1.06, 95% CI: 0.8, 1.32).
Methodologic quality assessment
All the studies were nonrandomized retrospective studies comparing between LCA and PCA. 11 –22 The majority of the studies were single-center studies, with only three involving more than one center. 13,18,20 Only Finley and colleagues did not clearly describe their statistical methods. 14 Only Sidana and colleagues did not mention their procedural techniques for LCA and PCA. 19 Six studies had multiple publications of varying aspects of their study and did not mention whether or not these patients were the same patients in each publication or a different cohort. 11 –13,15,17,20
There was specific patient selection bias in three of eight studies, from which patient data were extracted into the meta-analysis. 15,16,22 Hinshaw and colleagues had larger tumors in the LCA group. 15 Zargar and colleagues had patients with higher BMI and more comorbidity in the PCA group. 22 Kim and colleagues had older patients, higher BMI, and larger tumors in the PCA group and more patients with multiple tumors in the LCA group. 16 Finley and colleagues and Sidana and colleagues did not mention a comparison between their basic patient demographic parameters. 14,19 Three studies reported no difference regarding patient characteristic between the groups. 18,20,21 Otherwise, all the studies mentioned their results with no publication or reporting bias, no missing data were identified, and no other risk of bias was found.
Discussion
Summary of the main results
Oncologic outcomes: there were significantly fewer tumors that were incompletely ablated and a higher cancer-specific survival rate in the LCA group. There was no difference between the two groups regarding late local recurrence rates. No difference in the 5-year recurrence-free survival was found.
Safety outcomes: there was no difference between the two groups regarding overall complications, however, subdividing the complications into the Clavien–Dindo classification, we found that there was more CD-I complications in the PCA group and more CD-III complications in the LCA group, implying that LCA is associated with a higher risk of significant complications. No difference between the two regarding CD-II or CD-IV complications, and no deaths were reported related to the procedures.
There was no difference between the two groups regarding transfusion rates; however, the PCA group had shorter length of hospital stay. There was no difference between the two groups regarding distant metastasis.
Incomplete ablation
There were strikingly different management strategies for the two treatments following incomplete ablation. The majority of patients in the LCA group who had incomplete ablation went on to have either PCA or opted for observation, while nearly all of those with incomplete ablation in the PCA group were managed by repeat PCA.
Cost analysis
Of the included studies, only one had a cost comparison analysis between the two groups. Hinshaw and colleagues found that the PCA group was significantly cheaper per patient by nearly half ($23,618 vs 14,175). 15
Two other published studies also found similar results favoring PCA to be the cheaper procedure. 23,24 Both studies took into consideration multiple variants such as fees, consumables, theatre costs, hospital stays, and pathology costs, while Link and colleagues used a modular approach to take into consideration impact of postoperative imaging and recurrence rates with subsequent treatments to predict a cost model. 23,24 All predictions and direct comparisons found PCA to be the cheaper of the two procedures. 24 Furthermore, Link and colleagues also found that both PCA and LCA were cheaper than laparoscopic or open partial nephrectomies. 24
Strengths and limitations of review
This is the first systematic review and meta-analysis comparison between LCA and PCA and was conducted to the highest standards using Cochrane and Prisma guidelines with an impartial look into the resulting data analysis. 8,9 The main limitation of the review is the fact that there is limited comparative studies (8) with even more limiting numbers in some of the subgroup analyses. Furthermore, all the studies were retrospective in nature with varying degrees of risks of bias. Although there was no difference between the two groups with regard to their ages or tumor sizes, the results indicate that the patients undergoing PCA had higher BMIs. Furthermore, it is plausible that many patients underwent PCA rather than LCA due to their comorbidities and lack of fitness, which would increase case ascertainment bias between the two groups. However, all these studies were set up not to be randomized and do declare the fault of a retrospective look on their results. A further risk of bias is with the mentioning of the incomplete ablation outcomes, specifically no mention of outcomes of subsequent management results after the initial incomplete ablation. However, those studies did not mention that they would present this specific data set. Most of the studies were conducted in single centers. However, despite these limitations, this represents the reported literature and gives a detailed understanding and overview of the difference between the two procedures. The total number of procedures reported was considerable and roughly equally divided between the two groups.
Future direction
The studies included in this review demonstrate the shortcomings of retrospective comparative studies. The only randomized controlled trial of needle ablation vs partial nephrectomy (CONSERVE) to date failed to recruit in its feasibility phase and so was not completed. 25 EuRECA (European Renal CryoAblation), a prospective, multicenter registry, including both laparoscopic and image-guided cryoablation, is currently accruing patients according to a strict protocol that includes comorbidities and nephrometry scores. The results of this registry should shed further light and provide more robust evidence for LCA and PCA results.
An interesting point regarding the two procedures is the increasing skill set of radiologists to perform these procedures in more complex cases. Furthermore, patients undergoing cryoablation tend to have more comorbidity and might not be good surgical candidates from the offset. In addition, with the advent of robotic partial nephrectomy, many laparoscopic surgeons have moved away from laparoscopic partials. Furthermore, more complex partial nephrectomy is being conducted with the robotic system, as an alternative to previously cryoablation. These points increase the likelihood that PCA use will continue for a selected patient cohort, while LCA might be replaced by robotic CA or even robotic partial nephrectomy. Only time will tell.
Conclusion
LCA had less incomplete tumor ablation rates and higher cancer-specific survival rates. PCA was effective as second line treatment for failed LCA or PCA. The advantages of percutaneous image-guided cryoablation over LCA are short hospitalization and reduced cost. There were more CD-I complications in the PCA group and more CD-III complications in the LCA group. Otherwise, there was no difference between the two procedures in any other parameters.
Footnotes
Acknowledgment
Dr. O.M.A. thanks Dr. Isra Ashi for her support.
Author Disclosure Statement
D.J.B., M.V.S., J.G., B.L., T.K.N., and F.X.K. Jr. are members of the Steering Committee for EuRECA, a European Renal Cryoablation Registry funded by a grant from Galil Medical.