
Abstract
Introduction:
Arterioureteral fistula (AUF) is a rare but potentially life-threatening disease that primarily arises as a long-term complication in oncological patients who have permanent ureteral stenting. The incidence is rising. The objective of this study was to outline the risk factors for management and outcome of AUF in a large individual case series.
Patients and Methods:
Twenty-six AUF cases in 24 patients from six German tertiary referral centers occurring between 2008 and 2016 were identified retrospectively and entered into a dedicated database by using patient notes and out-patient visits.
Results:
Of 24 patients, 23 had a history of abdominopelvic surgery for oncological disease, 21/24 had undergone radiotherapy, and 23/24 had long-term ureteral stenting. All cases presented with visible hematuria, 11/26 at the time of a stent exchange. Blood transfusions were required in 92.3%, and intravenous inotropes were needed in 46.2%. Of 26 patients, 11 had flank pain. CT angiogram was positive in 35.7%. Angiography and endovascular fistula repair was performed in 88.5%, and the rest received open surgical repair. Mortality was 7.7%. Endovascular treatment was technically successful in 91.3%, and open surgery was successful in 3/4 cases. Recurrent AUF developed in 3/24 patients. Stent-related complications occurred in 15%. Vascular complications were common. Long-term survival was limited due to progression of the underlying malignant disease.
Conclusion:
AUF results in major hemorrhage and warrants time-efficient diagnosis and treatment. Awareness is key. When AUF is considered, interventional angiography should promptly be performed. Fistula detection can be improved by guidewire manipulation. Pre-interventional CT angiogram may be omitted due to low sensitivity. Endovascular repair with stenting and/or coiling is effective and safe.
Introduction
S
AUF is a rare condition that leads to extensive hemorrhage from the urinary tract. This typically occurs at the iliac crossing of the ureter. The most common location is close to the iliac bifurcation. 2 There is a primary form linked to arterial aneurysm or arteriovenous malformation that accounts for roughly 15% of cases. 3 The remaining 85% are the more common secondary or iatrogenic form.
Some risk factors have been described in the literature: prior pelvic surgery, radiotherapy, chronic ureteral stenting, vascular disease, and prior vascular intervention in the pelvic region. AUF seems to affect women more commonly than men with a ratio of 3:2 to 3:1. 4,5
Surgery and radiation therapy harvest ischemia and fibrosis with fixation of the ureter to the arteries. Ureteral stents can enhance the damage by increasing pressure and facilitating necrosis and, eventually, fistula formation. 6
AUF was first described in 1899 as an effect of X-rays. Moschcowitz published the first successful treatment in 1908 by ligating the external iliac artery in a patient where fistula resulted from kidney stone surgery. 7,8 Open surgery remained the primary treatment option with vascular ligation and/or repair as well as nephrectomy. 3 It is only over the past decade that there has been a definitive shift toward endovascular treatment. 9 –12
The mortality remains high; however, it has fallen from 60% around 1980 toward 10% to 38% at present. 4,13 The available literature on the entity is still scarce with only small case series and few substantial review articles. 3,4,6,13 –16 As the incidence of AUF is increasing, there is a vital need for awareness to ensure the best possible outcome for affected patients. 13
Here, we report—to our knowledge—the largest individual case series of AUF in the literature so far.
Patients and Methods
AUF cases from six tertiary referral centers in Germany were collected retrospectively and entered into a dedicated database. Departmental hospital episode statistics were screened for the ICD-10 diagnosis code N28.8 (“ureteral fistula”), and the results were filtered for confirmed AUF cases.
Twenty-six cases in 24 patients (13 female, 11 male) were identified and diagnosed between April 2008 and November 2016. The mean age at diagnosis was 67.9 years (range 35–88).
Patient characteristics, comorbidities, presentation, and details of diagnosis and treatment were collected. Additional information on follow-up was gathered from out-patient visits.
Results
Risk factors
All but one patient had a history of oncological disease with prior major abdominopelvic surgery. The distribution of underlying tumor diseases is shown in Figure 1. One patient had a history of endometrial cancer and developed vaginal cancer as a secondary malignancy 15 years later. The non-oncological patient had a long-standing ureteric stricture with long-term stenting.
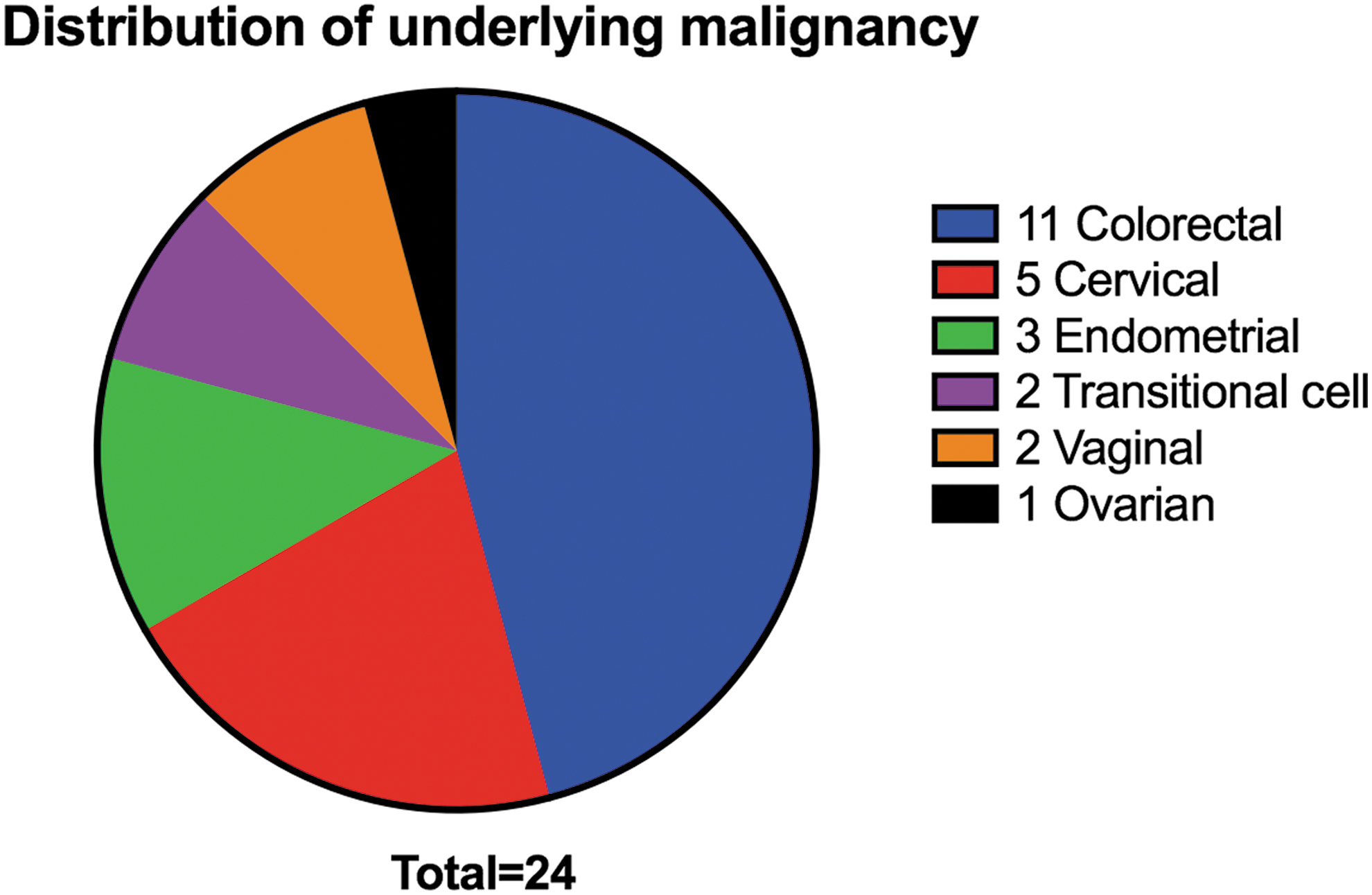
Twenty-four patients had a history of malignant disease. Here, the distribution of the primary histological entities is shown.
Out of 23 patients, 21 had received radiation therapy. All but one patient had long-term ureteral stents on the side involved in fistula formation, either after urinary diversion or due to ureteric stricture. The only patient without a stent had extensive metastatic vaginal cancer with a giant retroperitoneal metastasis directly involving the ureter and iliac artery and thus resulting in erosion and consecutive fistula.
Vascular disease was diagnosed in only two patients, one of them with an extensive history of interventions and complications.
Individual patient data are summarized in Table 1.
Surgical procedures and radiation therapy for tumor disease are given with the time span until diagnosis of AUF. Total duration of ureteral stenting before AUF diagnosis is shown.
APR = abdominoperineal resection; AUF = arterioureteral fistula; LAR = lower anterior resection of the rectum.
Presentation
All patients presented with visible hematuria. In 11 cases, this occurred during ureteral stent exchange. Fifteen patients had significant hematuria without prior manipulation. Of the 26 patients, 24 required blood transfusions for major hemorrhage, and 12/26 required intravenous inotropes for hemorrhagic shock.
In 11/26 cases, patients complained of flank pain, usually from hydronephrosis secondary to blood clots in the ureter and collecting system. Four patients spiked a temperature around the time of diagnosis with AUF.
Diagnosis
In 14/26 cases, CT angiogram was performed, which could confirm AUF in five cases (35.7%). Of these five, three did not have an indwelling ureteral stent at the time of CT. Of the remaining patients with an indwelling stent, one required a repeat CT to confirm the fistula after an initial negative report.
In 23/26 cases, angiography was performed for diagnosis and therapy. In nine patients, conventional angiography was positive for AUF (39.1%). A provocation maneuver was performed in 12 cases by either pulling back the ureteral stent or trying to advance a guidewire through the fistula into the ureter. In all cases, this maneuver successfully revealed the fistula. When no fistula was seen, a covered stent graft was inserted at the site of the ureteric crossing. The right and left ureter were concerned in 13 cases each.
The most common localization of the fistula was the common iliac artery in 11 cases. The internal iliac artery was involved in nine cases, and the external iliac artery was involved in six cases. Figure 2A–D illustrates a typical angiographic scenario of AUF detection and treatment in a patient with long-term ureteral stenting after surgery and radiation therapy for colorectal cancer.

The aforementioned provocation maneuver by advancing a guidewire through the fistula is illustrated in Figure 3.
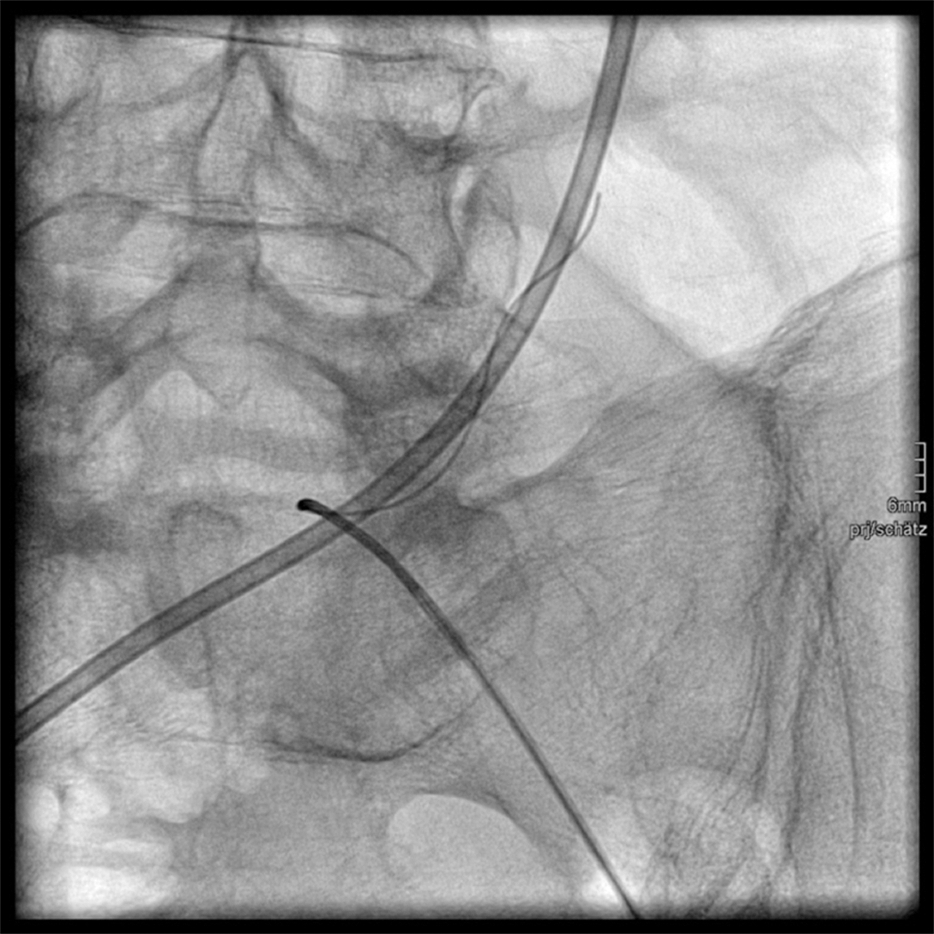
Digital subtraction angiographic run. Left ureter with ureteral stent close to the left CIA. Guidewire-based detection of an AUF between the left distal ureter and the CIA. The guidewire enters the ureter through the fistula and wraps around the indwelling ureteral stent.
Treatment and treatment success
All 23 patients undergoing angiography received endovascular treatment. Seventeen patients were treated with a covered stent graft alone. This was successful in 14 cases. In one case, the fistula could not be detected, so a stent was inserted to cover the ureteric crossing. As further hematuria occurred, angiography was repeated and revealed a fistula that was then successfully treated by further stent insertion and coiling of the internal iliac artery. The other two patients with ongoing hemorrhage were considered for surgery but did not consent. Both died from recurrent bleeding and progression of the underlying diseases after 2 and 5 months, respectively.
Three patients were treated with stent graft in combination with vascular coiling. In all cases, this was technically successful; however, one patient did not survive due to the acute morbidity. Coiling alone was sufficient in two cases where the site of the fistula was at the internal iliac artery.
All patients who underwent stent grafting were started on a lifelong antiplatelet therapy with acetylsalicylic acid 100 mg once daily. Two patients received additional treatment with clopidogrel 75 mg once daily for 3 months. Long-term antibiotic prophylaxis was not applied.
Four patients did not receive endovascular treatment but underwent emergency surgery. In three cases, nephrectomy and vascular repair was performed. This was successful in two patients, and one patient died from exsanguination during the procedure.
In one patient, an ileal conduit had to be resected in addition to vascular repair.
Overall, 24/26 patients (92.3%) survived the acute situation.
Follow-up
Two patients did not survive the acute occurrence of AUF (acute mortality 7.7%). One patient was lost to follow-up after successful treatment.
Of the remaining 21 patients, 12 are alive as of January 2017 after a median follow-up time of 8 months (mean 17.5 months, range 1–80).
Nine patients died during follow-up with a median follow-up time of 4 months (mean 8.25 months, range 0.25–34). The cause of death could in most cases be attributed to the underlying tumor disease and/or to ongoing AUF-related morbidity: Three patients died from tumor recurrence or progression; three patients died from hemorrhage secondary to rectoconduital fistula, enterovesical fistula, and arterioenteric fistula respectively. Two of these patients also showed signs of tumor progression. One patient died from ongoing AUF bleeding and refused further therapy due to his limited overall prognosis. Another patient died from lower gastrointestinal bleeding. In one case, the cause of death was not reported.
Recurrence
In three cases, AUF recurrence was observed (twice on the ipsilateral side, once on the contralateral side). Two of these patients underwent successful stent grafting. The third patient received endovascular coiling and developed a further recurrence that was then treated with a vascular ligation and cross-over bypass.
Specific complications after interventional therapy
Two patients developed stent occlusion and required repeat angiography. One patient who was treated with ciprofloxacin for a urinary tract infection (UTI) at the time of AUF diagnosis later developed an infection of the stent graft.
One patient developed pyonephrosis, which could be managed with antibiotic treatment and continued ureteral stenting.
After coiling of the internal iliac artery and stent insertion, one patient developed ischemic pain in his ipsilateral hip and leg that spontaneously resolved. Another patient developed ipsilateral calve ischemia.
Specific complications after surgical therapy
One patient required a repeat laparotomy after nephrectomy and vascular repair for wound dehiscence.
Non-specific complications
Three patients developed gastric ulcers with upper gastrointestinal bleeding. Paralytic ileus occurred in two cases. One patient showed Leriche syndrome (before AUF treatment). One patient had to be resuscitated for pulseless electrical activity, which was successful.
One patient with underlying vascular disease later developed an arterioenteric fistula arising from the iliac arteries.
Discussion
The incidence of AUF is increasing. 13 This is mainly a consequence of the improved survival of cancer patients who are prone to develop complications of radical surgical treatment and radiation therapy. The diagnosis is rarely seen among non-oncological patients. However, the underlying disease and its management may be related to a number of different specialties (Urology, Gynecology, Gastrointestinal Surgery, Radiation Oncology). Still, most patients will first be diagnosed by the urologist who needs to be aware of the typical clinical presentation and be competent in the management. The “classical” AUF patient will match a trifecta of risk factors in their history: major abdominopelvic surgery, radiation therapy, and long-term ureteral stenting. They will most likely present with a history of recurrent visible hematuria and then develop sudden hemodynamically relevant hematuria during a stent exchange. The need for transfusions and/or inotropic therapy is common. Flank pain and fever may occur as well. In any case, a ureteral stent should be reinserted as it helps to control the bleeding by covering the fistula. Stent-related hematuria (by irritation) is usually much less severe than hematuria from AUF, so one can usually distinguish between the two.
If a patient at risk for AUF develops visible hematuria without undergoing a stent exchange, a point-of-care sonography may help to identify the laterality of the fistula by showing hydronephrosis and/or clots in the renal collecting system.
In the therapeutic management of AUF, there has been a paradigm shift in recent years from a surgical approach, which was still the standard of care in 2004, toward interventional angiography. 3,6,17 In most cases, angiography has proved itself more effective with reduced mortality and morbidity rates. The relevant patient cohort bears high surgical risk: Previous extensive surgery and radiation therapy lead to difficult operating conditions with adhesions, fibrosis, and frail tissue. Thus, laparotomy should be avoided if possible.
Alternative management techniques have been suggested, such as occluding the ureteric plain by coiling and injection of gelatinous sponges via a nephrostomy, but this will only be relevant and helpful in individual cases and not in an emergency situation. 18
Interventional angiography is the crucial step in both diagnosis and therapy. Our figures confirm that CT angiogram is only positive in 25% to 42% of cases. 13,19 It has been advocated to administer a contrast agent retrogradely into the ureter to improve the sensitivity. 13 We advocate the omission of a CT scan. It is not a sufficient diagnostic test for AUF and the patient will have to undergo angiography anyway. The sensitivity of conventional angiography alone is 39% to 69%. 13,20 The use of a provocation maneuver by pulling back the ureteral stent or trying to negotiate the fistula angiographically can improve sensitivity dramatically (in our cohort toward 100%), but may result in further hemorrhage, so it should only be performed when the interventionalist is prepared to stent and/or coil at once. We found that the use of a soft hydrophilic guidewire to negotiate the fistula while keeping the ureteral stent in place is very effective for localization and rarely causes complications.
Communication between the specialists involved in the case is crucial. Mortality from AUF is much lower when the interventional radiologist is aware of the suspected diagnosis before commencing angiography. 2 Most of the time, the fistula will form at the site of the iliac bifurcation but atypical localizations must be considered. Fistulae from the aorta have been described. 4 In our cohort, the internal iliac artery was involved in 34.6% of cases. In this case, arterial coiling may be employed to occlude the fistula as most patients will form collateral vascularization from the external iliac line of flow. Multiple oblique projections during angiography can help to identify pseudo-aneurysms as an indirect sign of fistula. 21
After stent placement, lifelong anti-platelet therapy with acetylsalicylic acid is essential. In most cases, further anticoagulation with clopidogrel or comparable drugs can be avoided. Long-term antibiotic therapy was recommended in the past. We advocate the policy of single-shot prophylaxis. If UTI is detected on urine culture, adequate antibiotic therapy needs to be administered. In our cohort, only one patient developed an infection of the vascular stent, which is in keeping with figures from centers where long-term antibiotic prophylaxis is the standard, so we believe this may be omitted. 5 However, every patient must receive some degree of antibiotic treatment as a majority will have a UTI on urine culture and a significant group will have positive blood cultures. 19
The mortality from AUF has fallen drastically over the past 40 years, especially since the advent of endovascular therapy. In our cohort, the acute mortality was 7.7%, which is at the lower end of the spectrum of what is being reported in current publications. 3,4,13 Still, most patients with AUF have a limited overall prognosis due to their oncological co-morbidity. AUF may be an expression of limited resources of the body to repair damaged tissue. There remains a relatively high risk for fistula recurrence.
Vascular disease has previously been described as a risk factor for AUF. 4 In our cohort, very few patients had underlying vascular disease. It may not be a risk factor per se, but if present, it can potentially harvest further complications such as ischemia after arterial coiling that cannot be compensated or formation of further arterial fistulae.
Our study is limited by its retrospective nature and, despite it being the largest case series to be published so far by our knowledge, by the small number of cases. The timeframe for follow-up was quite heterogeneous. It is difficult to obtain reliable findings on this rare disease, but the key features are well established.
Table 2 gives a short summary of the most important aspects in the diagnosis and management of AUF.
KUB = kidney, ureter, and bladder radiograph.
In conclusion, our data demonstrate that AUF is gaining relevance for the clinical practice of urologists. There is a well-defined interdisciplinary diagnostic and therapeutic pathway that results in acceptable acute mortality and morbidity if the diagnosis is considered in a timely manner.
Footnotes
Acknowledgment
This study is the result of a multi-institutional collaboration enabled by GeSRU Academics, a network of academic urologists-in-training within the German Society of Residents in Urology.
Author Disclosure Statement
No competing financial interests exist.