
Abstract
Objective:
To evaluate the outcomes of laparoendoscopic single-site nephrolithotomy (LESS-NL) for symptomatic caliceal diverticular calculi.
Patients and Methods:
From November 2009 to March 2014, 11 cases of LESS-NL with a homemade single-port device for caliceal diverticular calculi were performed by a single experienced laparoscopic surgeon. All patients were assessed at postoperative 1 month, 1 year, and 3 years for symptom-free status and by CT for stone-free and caliceal diverticular obliteration status. All complications were categorized by the Clavien–Dindo classification. Demographic parameters and postoperative outcomes were retrospectively analyzed.
Results:
All procedures were effectively performed without conversion to open or conventional laparoscopic surgery. Median patient age was 53 years (range 22–73), and median diverticular size was 26 mm (range 15–58). Six patients (54.5%) had multiple stones, and five patients (45.5%) had a single stone; median stone size was 20.6 mm (range 12.1–66.4). The transperitoneal approach was used in seven patients (63.6%) and retroperitoneal approach in four patients (36.4%). Median operative time was 161 minutes (range 110–250), median estimated blood loss was 50 mL (range 20–400), and median hospital stay was 4 days (range 3–6). An additional needlescopic instrument was used in five cases (45.5%). There were three cases (27.3%) of grade I complications (two postoperative fever, one ileus), and no intraoperative or major complications. Median visual analog scale score significantly improved by discharge day (from 4.9 preoperatively to 1.4; p = 0.003). After a median follow-up of 38 months (range 36–41), all patients were symptom free with no evidence of stone or caliceal diverticulum on imaging.
Conclusions:
LESS-NL is a safe, feasible, and definitive treatment option for symptomatic caliceal diverticular calculi.
Introduction
C
There are multiple treatment options for symptomatic caliceal diverticular calculi, including percutaneous nephrolithotomy (PCNL), ureteroscopy (URS), and shockwave lithotripsy (SWL). In the past few years, conventional laparoscopic management has been reported to be an effective procedure, with high stone-free rates and low morbidities. 4 –10 With advancements in surgical instruments and trends toward minimal invasiveness, the laparoendoscopic single-site (LESS) procedure has been introduced as a novel surgical procedure. LESS surgery is defined as laparoscopic surgery through a single skin incision or a single incision plus one extrapuncture for a small (2–3 mm)-diameter instrument. 11 LESS surgery is known to provide better cosmetic outcome, less postoperative pain, and fewer port-site-related complications than conventional laparoscopic surgery. 12
To our knowledge, no studies have reported the outcomes of LESS management for caliceal diverticular calculi. In this study, we describe our experience with laparoendoscopic single-site nephrolithotomy (LESS-NL) performed by a single operator using a homemade single-port device to evaluate the safety and feasibility of LESS-NL as a definitive treatment for caliceal diverticular calculi.
Patients and Methods
Patients
This retrospective study was approved by the Institutional Review Board of Samsung Medical Center. A total of 11 cases of LESS-NL performed for caliceal diverticular calculi by a single, experienced laparoscopic surgeon between November 2009 and March 2014 were included in this study. The surgeon had clinical practice for 5 years with an experience of >200 cases of laparoscopic surgeries, including >30 cases of LESS before the first case of LESS-NL for caliceal diverticular calculi.
Informed consent was obtained from all patients. All patients presented with flank pain and/or urinary tract infection and underwent preoperative CT urography showing the location of the caliceal diverticula and the presence of calculi. There were no other urinary calculi in these patients. Two (18.2%) of the 11 patients had previously undergone ineffective SWL and 1 patient (9.1%) had failed a previous attempt at flexible URS. The indications for LESS-NL were symptomatic caliceal diverticular calculi with thin overlying renal parenchyma or caliceal diverticulum with a large stone burden.
Surgical technique
Under general anesthesia, the patient was placed in the lateral decubitus position. For transperitoneal LESS-NL for caliceal diverticular calculi, we used a homemade single-port device as previously described. 13 A wound retractor (Alexis; Applied Medical, Rancho Santa Margarita, CA) was inserted through a 2- to 2.5-cm incision site at the umbilicus. The homemade single-port device was constructed by cutting off the tips of the first, third, and fifth fingers of a size 6½ surgical glove. A 10-mm trocar was placed in each of the third and fifth finger openings, and a 5-mm trocar was placed in the first finger opening.
A 10-mm rigid laparoscope with variable direction of view (EndoCAMeleon; Karl Storz, Tuttlingen, Germany) was introduced. We used a 5-mm articulating working instrument (Autonomy Laparo-Angle; Cambridge Endo, Framingham, MA) for most of the dissection and retraction maneuvers to overcome the lack of triangulation. Standard laparoscopic instruments such as hook cautery and ultrasonic scissors were also used. For effective traction and suturing, an ancillary needlescopic instrument without additional trocar placement was used if necessary.
After renal hilar dissection, the renal artery was recognized and dissected carefully. Gerota's fascia was incised to identify and mobilize the kidney. The perinephric fat was dissected from the kidney, and examination of the kidney surface was performed. The location of caliceal diverticulum was identified by a depression or bulge area on the surface of the kidney. If it was not apparent, we used intraoperative ultrasonography for stone localization. The thinnest area of renal parenchyma over the stone was incised by laparoscopic scissor or J-hook electrocautery (Fig. 1A). When the overlying parenchyma was thick and seemed to bleed much, the renal artery was clamped with a bulldog clamp before parenchymal incision.
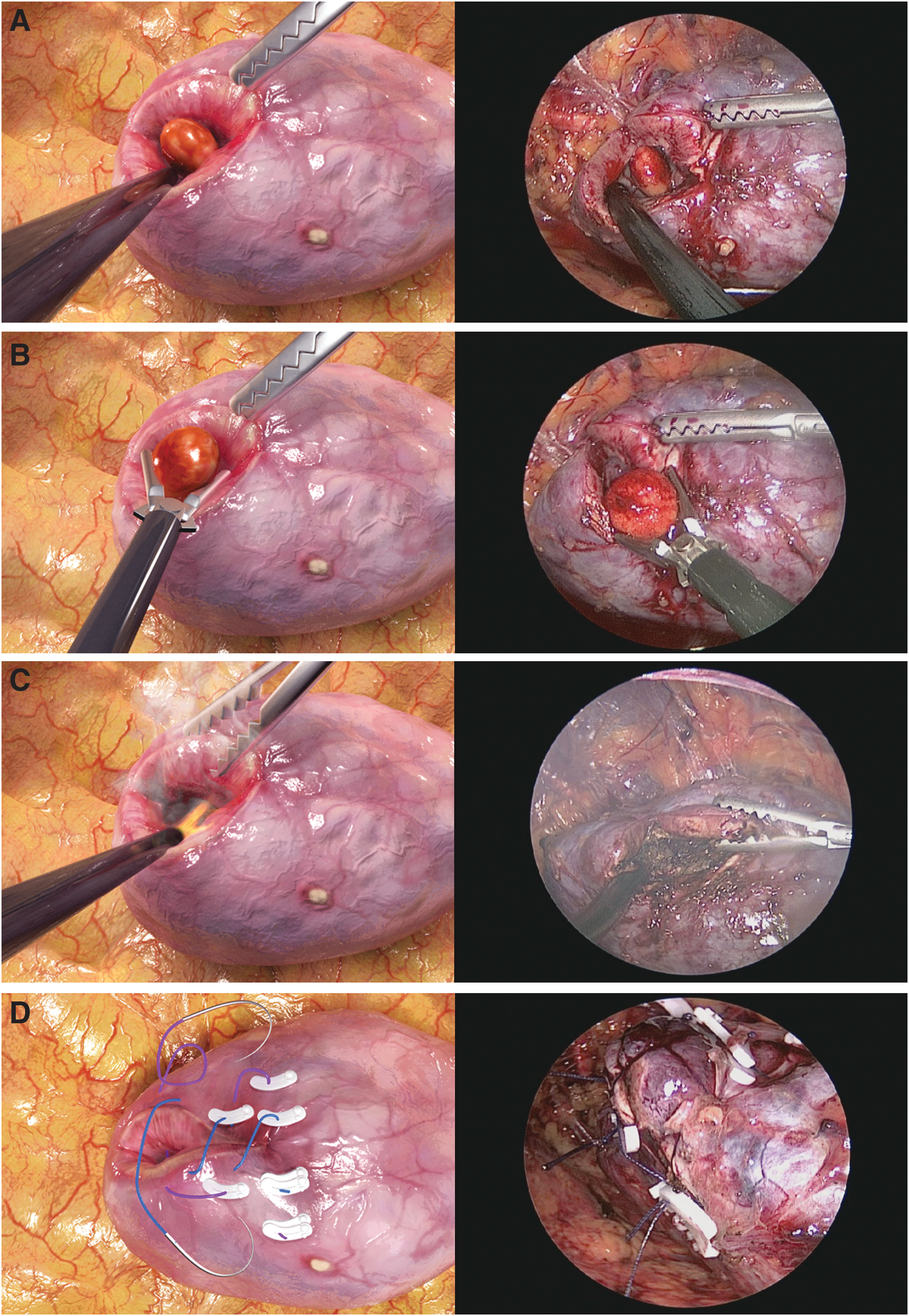
Laparoendoscopic single-site nephrolithotomy for caliceal diverticular calculi.
Stones were extracted with a laparoscopic grasper (Fig. 1B). The argon beam coagulator was used for fulgurating most of the urothelial lining of the diverticular cavity and diverticular neck (Fig. 1C). Renal parenchymal approximation was performed using a 1-0 Vicryl preplaced 10 mm Hem-o-lok clip above a knot tied at the suture end that was sequentially placed through the parenchyma of the kidney and then through the base of the caliceal diverticulum and the opposite end of the renal parenchyma. Hem-o-lok clips were used to fix the entry and exit sites of the suture. Reinforced continuous sutures were performed using 1-0 Vicryl suture preplaced Hem-o-lok clips (Fig. 1D). After the renal artery was unclamped, the presence of bleeding or urine leakage was identified, and a Jackson-Pratt drain was placed.
Regarding retroperitoneal LESS-NL for caliceal diverticular calculi, a 2- to 2.5-cm transverse skin incision was made 2 cm caudal from the inferior border of the 12th rib in the midaxillary line for insertion of the wound retractor. The retroperitoneal working space was formed by a balloon dilator that was filled with 1 L of physiologic saline. Surgical procedures were the same as transperitoneal LESS-NL (Supplementary Video; Supplementary Data are available online at
Clinical parameters
Demographic data included body mass index (BMI), gender, age, stone size, the thinnest diverticular wall thickness, caliceal diverticulum size, location, and laterality (right or left). Various perioperative parameters were analyzed, including operative time, ancillary needlescopic instrument use, estimated blood loss, intraoperative ultrasound use, warm ischemic time, hospital stay, pain scores, stone-free status, symptom-free status, caliceal diverticular obliteration status, and postoperative complications.
Estimated glomerular filtration rate (eGFR) was checked within 3 months preoperatively and 1 month postoperatively. Caliceal diverticulum size was defined by calculating the longest axis on preoperative CT. Stone size was determined by calculating the longest diameter on preoperative CT; in the case of multiple calculi, it was defined as the summation of the longest axis of each calculus. Operative time was measured as the interval between skin incision and skin closure. Operation-related pain was evaluated with the visual analog scale (VAS) on the first day after surgery and at discharge. Complications were recorded according to a modified Clavien–Dindo classification. 14
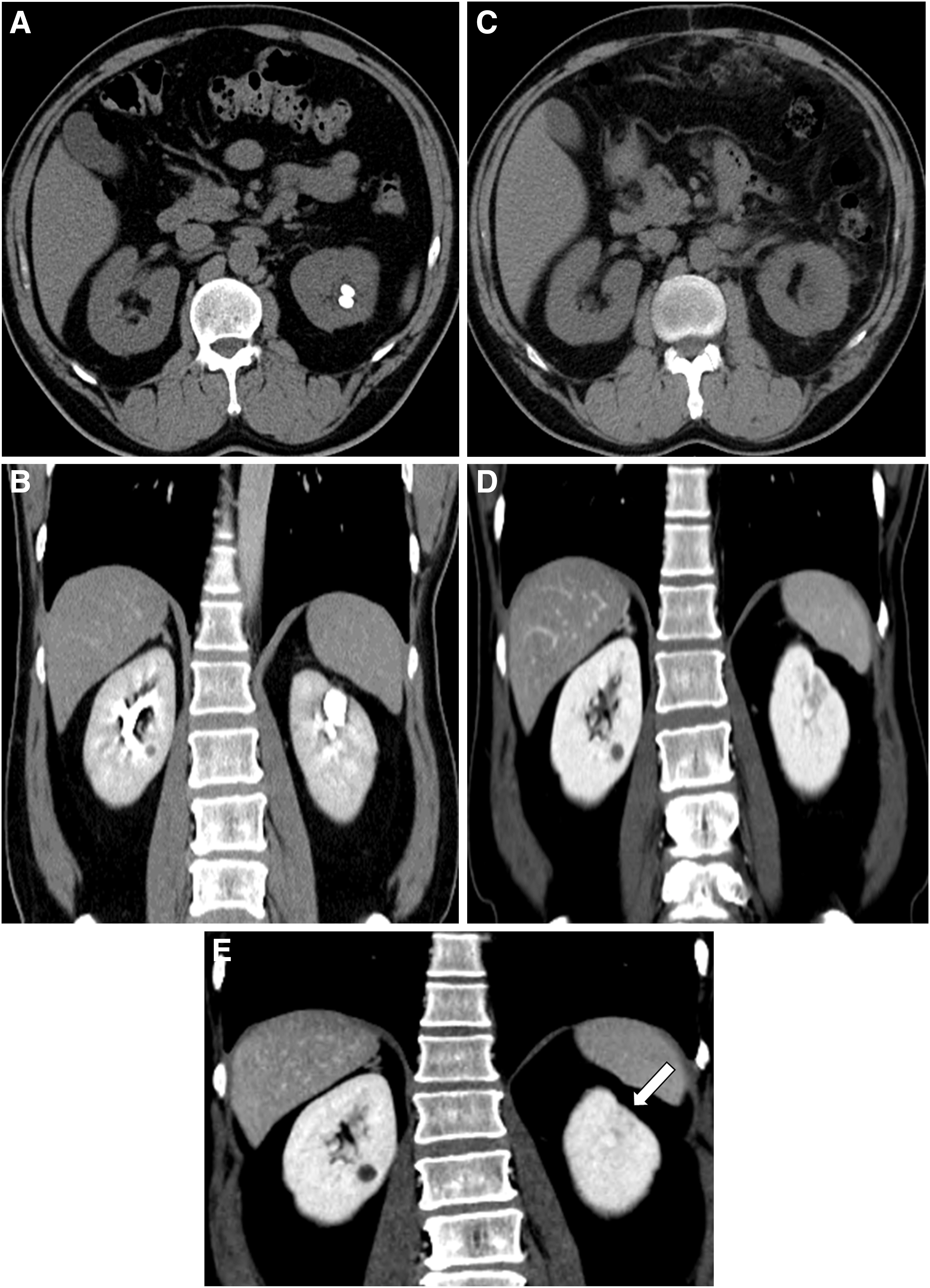
Symptom-free status was assessed at 1 month, 1 year, and 3 years postoperatively. All patients were evaluated with CT at postoperative 1 month, 1 year, and 3 years for stone-free and caliceal diverticular obliteration status.
Statistical analyses
Continuous variables are shown as median (interquartile range or IQR), and categorical variables are shown as absolute value (percentage). A paired t-test or Wilcoxon signed-rank test was used to analyze the differences in VAS scores. All statistical analyses were performed using SPSS, version 13.0 (SPSS, Inc., Chicago, IL). Statistical significance was considered a value of p < 0.05.
Results
Table 1 shows the preoperative characteristics of the 11 patients who underwent LESS-NL for caliceal diverticular calculi. The median age was 53 years (IQR 35–63), and the median BMI was 24.2 kg/m2 (IQR 21.9–25.4). The median diverticulum size was 26.0 mm (IQR 18.0–34.5). Caliceal diverticula were located in the upper calix in five (45.4%), interpolar calix in four (36.4%), and lower calix in two (18.2%) patients. The thickness of the thinnest diverticular wall was 3.2 mm (IQR 1.8–5.4). Six patients (54.5%) had multiple stones, and five patients (45.5%) had a single stone. The median stone size was 20.6 mm (IQR 14.8–21.3).
BMI = body mass index; IQR = interquartile range; VAS = visual analog scale.
Perioperative and postoperative data are shown in Table 2. All surgical procedures were effectively completed without conversion to open or conventional laparoscopic surgery. Seven patients (63.6%) underwent transperitoneal LESS-NL for caliceal diverticular calculi, and four patients (36.4%) underwent retroperitoneal LESS-NL for caliceal diverticular calculi.
Renal hilar control was performed in five patients.
LESS-NL = laparoendoscopic single-site nephrolithotomy.
The median operative time was 161 minutes (IQR 150–195), and ancillary needlescopic instrument was used in five cases (45.5%) of LESS-NL for caliceal diverticular calculi for suturing or liver or bowel traction. Intraoperative ultrasound was used for stone localization in six cases (54.5%). Renal hilar control using a laparoscopic bulldog clamp was performed in five cases (45.5%). The median warm ischemic time was 21 minutes (IQR 20–25). The median VAS score on postoperative day 1 was 4.6 (IQR 4.0–5.4) and it was decreased to 1.4 (IQR 0–1.7) at discharge (p = 0.003). A Jackson-Pratt drain remained indwelling a median of 2 days (IQR 1.5–3), and the median hospital stay was 4 days (IQR 3–4).
No intraoperative or major postoperative complication was observed. There were three cases (27.3%) of grade I complications (two postoperative fever, one ileus), and all were conservatively managed. There was no statistical difference between the median preoperative and postoperative eGFR [preoperative eGFR vs postoperative eGFR, 92.4 mL/min (IQR 82.6–94.3) vs 80.4 mL/min (IQR 77.2–96.1), p = 0.092].
The median follow-up was 38.0 months (IQR 37.0–38.5). All patients were asymptomatic postoperatively, with no reported symptom recurrence during follow-up. Stone-free status and obliteration of the caliceal diverticular cavity were achieved in all cases on CT images at postoperative 1 month, 1 year, and 3 years (Fig. 2).
Discussion
In the present study of patients who underwent LESS-NL for symptomatic caliceal diverticular calculi, we observed symptom-free, stone-free, and diverticular obliteration rates of 100% without major complications at a mean follow-up of 38.6 months.
The management of caliceal diverticular calculi has changed from open procedure to minimally invasive methods, including SWL, URS, PCNL, and laparoscopic approach.
The success rate of SWL in the treatment of caliceal diverticular calculi is generally low because of remaining underlying pathology and inadequate stone passage. Published studies reported poor outcomes with symptom-free rates of 36%–75% and stone-free rates of only 8%–40%. 3
URS demonstrated symptom-free rates ranging from 35% to 100%, stone-free rates ranging from 19% to 94%, and diverticular obliteration rates ranging from 7% to 18%. 3 Although the ureteroscopic approach is less invasive, there could be substantial difficulty in locating the diverticular ostia and ablation of the caliceal diverticular lining. Ureteroscopic management was usually indicated for small calculi in upper or interpolar caliceal diverticula. 15
Percutaneous treatment of caliceal diverticular calculi was associated with a higher success rate with dilation of the diverticular ostium at time of operation, with 77%–100% symptom-free rate, 69%–100% stone-free rate, and 8%–100% diverticular obliteration rate. 3 Although a percutaneous approach allowed directed management of the underlying pathology, complication rates as high as 54% were noted. 16 The difficulty in managing anteriorly located caliceal diverticulum, tract loss during management of small caliceal diverticulum, and difficulty in obliterating large caliceal diverticulum were possible drawbacks.
Anterior or posterior thin-walled caliceal diverticulum, caliceal diverticulum containing large calculi, and caliceal diverticulum with a narrow neck inaccessible by retrograde access were reported to be suitable for a laparoscopic approach. 8,10,15 The goal of treatment should be complete obliteration of the caliceal diverticulum for removal of the potential cavity for stagnant urine and calculi formation. 17 The laparoscopic approach revealed the highest success rates for caliceal diverticular obliteration (50%–100%). 5,8 –10 Table 3 summarizes previous studies on conventional laparoscopic management of caliceal diverticular calculi.
CRN = conventional retroperitoneal laparoscopic nephrolithotomy; CTN = conventional transperitoneal laparoscopic nephrolithotomy; LESS-TN/RN = laparoendoscopic single-site nephrolithotomy—transperitoneal nephrolithotomy/retroperitoneal nephrolithotomy; NR = not reported.
A transperitoneal or retroperitoneal approach has been used for conventional laparoscopic management depending on the diverticular location and the preference of the surgeon. Laparoscopic surgery traditionally uses three to six ports according to a given procedure, with each port increasing the potential morbidity from internal organ damage, bleeding, and port-site hernia and decreasing the cosmetic results. 18,19 As there has been a surge in the demand for less invasive alternatives, LESS surgery has been introduced as an evolutionary procedure beyond conventional laparoscopic surgery and has been increasingly performed for various urologic diseases.
To the best of our knowledge, the current study is the first to provide evidence on the long-term outcome of LESS surgery for caliceal diverticular calculi and the largest case series for laparoscopic management of the caliceal diverticular calculi by a single operator at a single institution.
LESS can lead to the loss of triangulation and distance, clashing of instruments, difficulty in overall procedure performance, and consequently a presumably longer operative time. 12 However, in the current study, the mean operative time was 170.7 minutes, which was consistent with that reported for conventional laparoscopic surgery (80.0–215.0 minutes). 5 –9 We assume that the use of an additional needlescopic instrument for effective suturing and liver or bowel traction and a sliding-clip technique for the renal parenchymal approximation contributed to our decreased operation time. The mean hospital stay was 3.8 days, which is similar to or shorter than previous studies of conventional laparoscopic management (1.5–9.5 days). 4 –9
As reported by other LESS studies, we observed a statistically significant improvement in VAS score after LESS-NL for caliceal diverticular calculi. The median VAS score before surgery and on postoperative day 1 was 4.9 (3.8–5.9) and 4.6 (4.0–5.4), respectively, and the median VAS score at discharge was 1.4 (0–1.7). Our diverticular obliteration rate (100%) was comparable with or better than other studies with results of 50%–100%. 4 –10 The reason for this outcome is presumed to be inclusion of the base of the caliceal diverticulum with renal parenchyma in a stitch during the renal parenchymal approximation. Our stone-free rate and symptom free-rate were both 100%, which are comparable with rates reported in published studies (Table 3).
Additional needlescopic instrument was used in five cases (45.5%) of LESS-NL for caliceal diverticular calculi in our study. The main advantage of needlescopic instrument use in LESS-NL is that it decreases loss of instrument triangulation, which is one of the limitations of LESS surgery. Liatsikos et al. 20 noted that ancillary instruments were necessary in >40% of all their LESS surgeries and concluded that needlescopic assistance in upper urinary tract LESS does not compromise any of the benefits of single-port surgery. Cosmetic outcome in laparoscopic surgery can be influenced by the number of port scars and the port insertion sites. 21 The most noticeable advantage of LESS-NL for caliceal diverticular calculi is that only one incision is required during the procedure, which can improve the cosmetic outcome (Fig. 3).

Representative postoperative wound of transperitoneal LESS nephrolithotomy. Only a small invisible scar remained at the umbilicus of the patient. LESS = laparoendoscopic single site.
All patients in our study effectively underwent LESS-NL for caliceal diverticular calculi, and there was no conversion to conventional laparoscopy or open surgery. There were only three cases (27.3%) of grade I complication, which were postoperative fever and ileus. There was no major complication after LESS-NL for caliceal diverticular calculi.
Our study on LESS-NL for caliceal diverticular calculi had several limitations. First, the current study represented a retrospective analysis. Second, we did not compare LESS-NL with conventional laparoscopic nephrolithotomy for caliceal diverticular calculi, but only assessed the feasibility and safety. Third, because of the laparoscopic expertise of the involved centers, the less experienced surgeons could potentially produce different outcomes for LESS approach. Fourth, no objective measurement was used to evaluate postoperative symptom relief. Symptom free was decided according to patient's subjective expression during the follow-up. Finally, the sample size was relatively small. Nevertheless, our study is valuable because it is the largest case series for laparoscopic management of the caliceal diverticular calculi and provides long-term data for LESS-NL for caliceal diverticular calculi.
Conclusions
LESS-NL provides surgical outcomes comparable with those of conventional laparoscopic literature with regard to success rate, hospital stay, and operative time in the surgical management of caliceal diverticular calculi. Although LESS-NL for caliceal diverticular calculi is still a challenging procedure, with the use of an ancillary needlescopic instrument and sliding-clip technique for renal parenchymal approximation, we demonstrated that LESS-NL for caliceal diverticular calculi can produce a high long-term success rate and a low complication rate. Therefore, LESS-NL appears to be a safe, feasible, and definitive treatment option with minimal scar formation for symptomatic caliceal diverticular calculi. Proof of safety, outcomes, and standardization of our LESS-NL technique for caliceal diverticular calculi should be investigated in a prospective comparative study with adequate statistical power.
Footnotes
Acknowledgment
The authors thank Min Hwan Kim, Department of Medical Information and Media Services, Samsung Medical Center, Seoul, South Korea, for assistance with digital illustrations.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.