
Abstract
Introduction:
Flexible ureterorenoscopy (fURS) is one of the best solutions for treatment of renal calculi <2 cm and for upper urinary tract urothelial carcinoma conservative treatment. An adequate quality of vision is mandatory to help surgeon get better outcomes. No studies have been done, to our knowledge, about what fURS in the market has the best quality of vision.
Materials and Methods:
Seven different fURS were used to compare the image quality (Lithovue, Olympus V, Olympus V2, Storz Flex XC—in White Light and in Clara+Chroma mode—Wolf Cobra Vision, Olympus P6, and Storx Flex X2). Two standardized grids to evaluate contrast and image definition and three stones of different composition were filmed in four standardized different scenarios. These videos were shown to 103 subjects (51 urologists and 52 nonurologists) who had to evaluate them with a rating scale from 1 (very bad) to 5 (very good).
Results:
No difference in terms of scores was observed for sex of the participants. Digital (D) ureterorenoscopes were rated better than fiber optics (FOs) ureterorenoscopes. Overall, Flex XC White Light and XC Clara+Chroma image quality resulted steadily better than other fURS (p < 0.0001). Olympus V generally provided a vision better than Lithovue. Cobra Vision and Olympus V2 had superimposable values that were significantly lower than Lithovue's ones. Olympus P6 and Storz X2 offered a low quality of vision compared to the others. In the medium simulating bleeding, Olympus V and V2 significantly improved their scores of 12% and 8.1%, contrary to rest of the ureterorenoscopes.
Conclusion:
D ureterorenoscopes have a better image quality than FO ones. The only disposable ureterorenoscope tested was comparable to the majority of other D ureterorenoscopes. The best image quality was provided by Storz D ureterorenoscopes, being Clara Chroma the favorite Spies Mode, according to literature.
Introduction
F
Materials and Methods
Seven different FUs [P6 (FO) (Olympus®); V (D) (Olympus); V2 (D) (Olympus); Flex XC (D) (Storz®); Flex X2 (FO) (Storz); Cobra Vision (D) (Wolf®); and LithoVue (D) (Boston Scientific)] were used to record eight different standardized videos of 3 seconds each. The Storz Flex XC was used with white light (WL) vision and using the Clara+Chroma (CC) modality, which has been reported to be the light mode offering best image quality in the Spies™ system. 6 Apart from the LithoVue, the FUs were not brand new. The selection of these FUs was made on purpose to simulate daily practice, where surgeons usually do not employ brand new ureterorenoscopes for fURS. All these ureterorenoscopes were assessed before the study and checked to be functioning and operating properly according to hospital standards. Two standardized grids (USAF 1951 and ColorChecker; Edmund Optics, Barrington, NJ) and three stones of different composition (monohydrate calcium oxalate, dehydrate calcium oxalate, and uric acid) were used to evaluate color contrast and definition of the images. All videos were taken at 3 cm from the FC camera. Images of the grids and stones were acquired in four standardized scenarios using the K-Box (Coloplast®) simulation model. The mediums used were as follows: 110 mL of saline solution, 110 mL of sterile water, 110 mL of saline solution mixed with 3 mL of iodine solution 0.3% (Betadine®) to simulate bleeding, and 80 mL of saline solution mixed with 30 mL of contrast. Betadine was used since it was not possible to use real human blood to simulate bleeding. In fact, multiple use FUs used for the study were the same used on daily practice on patients. Therefore, use of real blood on a bench model was not acceptable by our ethical committee. In total 96 videos were made. Twelve slides, each containing eight videos of the same scenario, were acquired to simultaneously compare all the devices. The position of the different videos was changed randomly in each slide. The angles of the squared D images were cut to give the same circular shape to all videos (Fig. 1). These videos were shown to 103 subjects (51 urologists and 52 nonurologists), of whom 33 were women and 70 men, with a mean age of 36 years (range 25–59). Each slide containing eight videos was shown for 15 seconds to the audience. Each 3 seconds single video inside the slide was played in loop. The subjects evaluated each video on a scale from 1 (very bad) to 5 (very good). The total score for every FU was calculated as the mean of each scenario.

An example of four different templates. In each slide are eight videos of the same subject obtained with eight different FUs.
Statistical analysis was performed with GraphPad Prism version 5 (GraphPad Software, Inc., San Diego, CA). t-Tests were used for comparison between two groups. One-way analysis of variance and Tukey's test were deployed for multiple comparisons. Statistically significant differences were assumed for p-values of <0.05. Adequacy of the sample size for comparison of groups was calculated by testing the first 30 cases with G*Power v. 3.1.9.2 (α 0.05, Power 0.95). The minimum sample size required proved to be 24.
Results
No differences in scores were observed according to the sex of the participants. In general, urologists gave significantly higher scores than nonurologists (mean ± standard deviation 2.84 ± 0.31 vs 2.7 ± 0.33, p = 0.04). Olympus V/V2 and Cobra Vision had significantly lower mean values in the nonurologist group (p < 0.04) while the other FUs had comparable scores. Optical ureterorenoscopes were scored lower than D ones (1.3 ± 0.4 vs 3.26 ± 0.42, respectively; p < 0.0001). As shown in Table 1, Flex XCWL and XCCC image quality was consistently better than that of the other FUs (p < 0.0001). Olympus V generally provided better vision than LithoVue (3.35 ± 0.65 vs 2.76 ± 0.54, respectively; p < 0.0001). Cobra Vision and Olympus V2 had superimposable values that were significantly lower than those for LithoVue. Olympus P6 and Storz X2 offered a low quality of vision compared with the other FUs.
Range of score were 1 (very bad) to 5 (very good). Storz digital ureterorenoscopes were evaluated in WL and CC mode.
CC = Clara+Chroma; WL = white light.
Consideration of only the images of number grids yielded the same results. Upon consideration of the images of color grids, the LithoVue score was comparable to that of Olympus V (3.26 ± 0.63 vs 3.29 ± 0.78, p = 0.75) and both scored significantly higher than Olympus V2 and Cobra Vision (p < 0.0001). On the other hand, for stone images Olympus V2 (2.69 ± 0.59) received better scores than LithoVue (2.36 ± 0.67) and Cobra Vision (2.43 ± 0.58) (p < 0.0001) (Fig. 2). The results of FUs in saline solution and sterile water resembled the total scores, even if in the former medium the difference between LithoVue and Olympus V was not significant (2.94 ± 0.64 and 3.08 ± 0.66, respectively; p = 0.12). In contrast-medium solution, Olympus V (3.57 ± 0.78) provided a good quality of image, far better than Cobra Vision, LithoVue, and Olympus V2 (2.63 ± 0.71, 2.66 ± 0.74, and 2.6 ± 0.65, respectively; p < 0.0001), for which the values did not differ significantly (all p > 0.5). In Betadine solution, the Flex XCCC still had the best scores but Olympus V provided an image definition similar to Flex XCWL (3.45 ± 0.89 vs 3.67 ± 0.78, respectively; p = 0.07). The scores for Cobra Vision (2.34 ± 0.64) were lower than those for LithoVue and Olympus V2 (2.58 ± 0.68 and 2.62 ± 0.74, respectively; both p < 0.01) (Fig. 3A).

Histogram representing the mean evaluations of the FUs with different targets. 1 = very bad, 5 = very good.
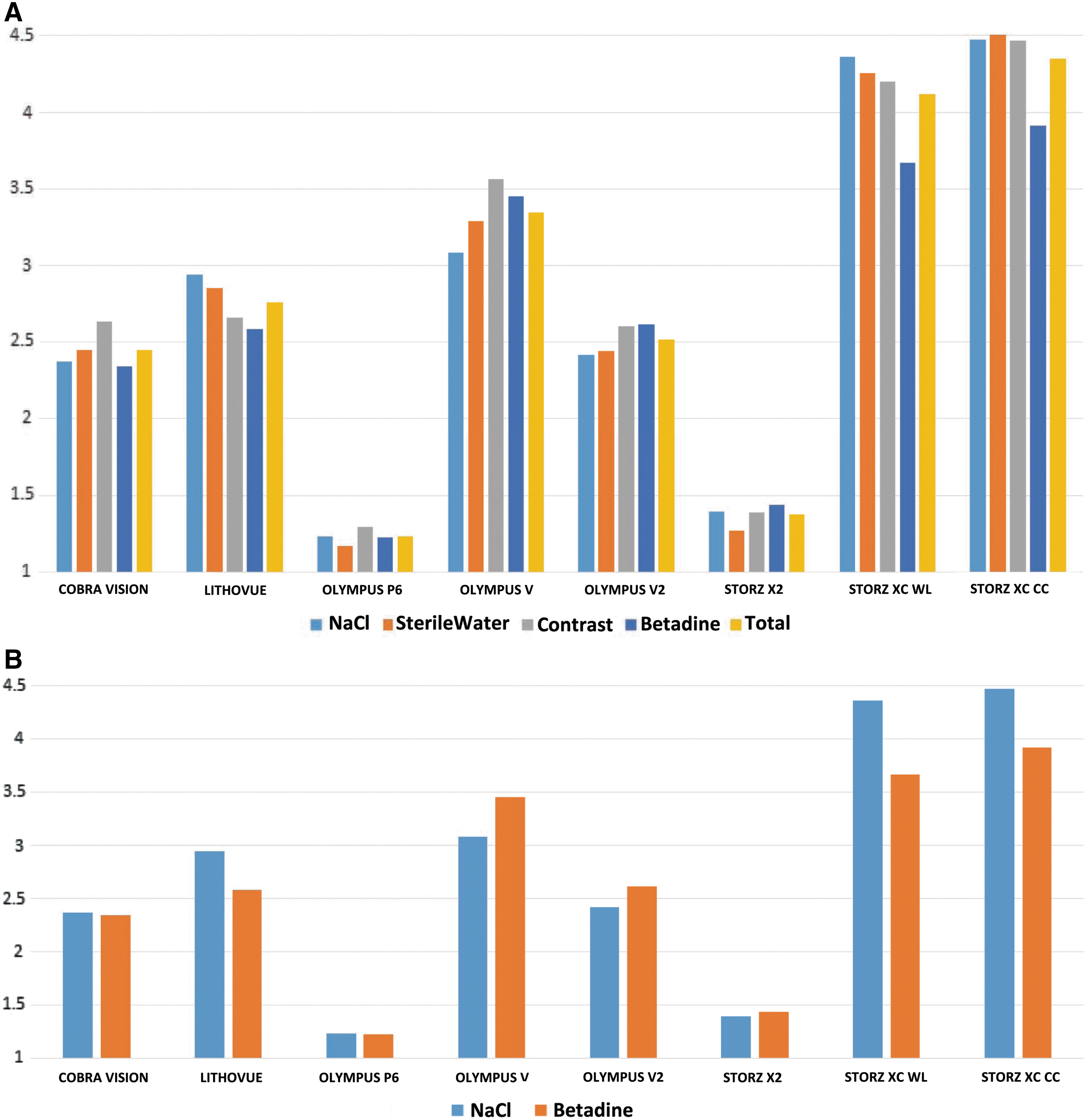
To evaluate the difference in image quality between saline and Betadine solution for all FUs, we calculated the difference in scores in the two mediums and analyzed the groups (Table 2). Olympus P6, Storz X2, and Cobra Vision provided a comparable resolution in the two mediums. The image quality scores for Storz XCWL and XCCC were, respectively, 15.9% and 12.4% lower in the Betadine solution, and a lower image quality in this medium was also observed for LithoVue (12%). By contrast, scores for Olympus V and V2 improved significantly in Betadine solution, by 12% and 8.1%, respectively (Tables 3 and 4; Fig. 3B).
To objectify the difference of image quality between saline and iodine solution for all fURS the difference of scores was calculated in the two mediums and the groups analyzed. Where the difference is negative, it means that iodine solution was better evaluated.
fURS = flexible ureterorenoscopy.
Storz XC was evaluated in WL and in CC modality.
Storz XC was evaluated in WL and in CC modality.
Discussion
Nowadays, fURS are widely performed. The introduction of D ureteroscopy has offered diverse advantages for diagnostic and treatment procedures, with a significant reduction in operative times when treating stones. 7 Due to the cost of instruments, not all urological centers own both D and FO FUs. In an era in which there is a free market and it is possible to choose between brands, it is useful to know the characteristics of instruments. To our knowledge, however, no studies have yet been done on the comparative image quality delivered by different FUs. It can be difficult for surgeons to decide what instrument to buy for their unit. Moreover, more than one company offers more than one FO and D model. While there is not a specific indication for use of a D or FO ureterorenoscope during stone treatment, D ureterorenoscopes appear to be the right choice in the case of UTUC. In fact, a D ureterorenoscope is the most valuable instrument for evaluation of the intrarenal collecting system and ureter under direct vision to allow complete tumor ablation. 8 New D disposable ureterorenoscopes relevant to this scenario are coming onto the market. The most similar to reusable ureterorenoscopes in terms of shape, images, and manipulation is the LithoVue (Boston Scientific). 5,9
In our study, as demonstrated previously, 10 D ureterorenoscopes resulted in better evaluation than FO ureterorenoscopes. Image quality is a characteristic that does not strictly need to be evaluated only by medical doctors. For this reason we decided to show images also to nonurologists, who appeared to prefer the Olympus V and V2 and Wolf Cobra Vision to the other FUs. The FU that had the best evaluation overall, with a statistically significant difference, was the D ureterorenoscope from Storz (Flex XC) in the WL and CC modalities, where CC had the best rate, as previously demonstrated. 6 The first-generation FU from Olympus (V) appear to offer better vision quality than the newer Olympus V2, probably owing to its larger dimensions. Overall, LithoVue had a better evaluation than Wolf CobraVision and Olympus V2, apparently gaining points with color grids and losing quality on stone images. The latter were well evaluated using the Olympus V2. No differences were found when images were recorded in saline and sterile water, while evaluations using contrast-medium solution revealed that Storz Flex XCCC remained the ureterorenoscope with the highest evaluation, followed by Storz XCWL and Olympus V. With both Olympus D ureterorenoscopes image quality improved significantly in Betadine solution, although worsening of image quality was observed for the remaining D ureterorenoscopes. No significant difference in quality was seen for FO ureterorenoscopes in saline and Betadine solutions. We did not analyze Olympus ureterorenoscopes in the narrow band imaging modality because this modality is specifically indicated for detection of urothelial tumors, whereas Spies modalities are not recommended by the company for any specific situation. 11 Certainly, vision is not the only parameter we have to consider while choosing what ureterorenoscope should be used for an operation. Also diameter and maneuverability should be taken into account. Dragos et al. 12 demonstrated that D FUs are less effective in accessing the sharp angled calix and they have lesser end-tip deflection compared with the fiber-optic counterparts.
The strengths of this study is the size of the group who evaluated the videos and the fact that this is the first study to compare the image quality offered by the most frequently used FUs on the market. Limitations are the in vitro setting and the impossibility of using real human blood for the experiment, since we used ureterorenoscopes intended for application in daily practice. Finally, not all the ureterorenoscopes available in the market were tested. This preliminary study is not intended to promote one ureterorenoscope over another; rather, it provides information for further in vivo assessments. All ureterorenoscopes analyzed are used commonly in many centers, and each of them has its own pros and cons. The aim of the study was to provide a general idea of the image quality. Beside image quality, maneuverability, ureterorenoscope body mass index, 13 and costs have to be take into consideration before buying an FU.
Conclusion
In this in vitro study, Storz Flex XCCC was ranked as the best FU in terms of image quality. Olympus V was evaluated to be better than V2. Overall, Boston Scientific LithoVue resulted having a better evaluation than Olympus V2 and Wolf Cobra Vision that were comparable. D ureterorenoscopes had better evaluations than FO ones.
Footnotes
Author Disclosure Statement
At the time of the study, Prof. Olivier Traxer was a consultant for Boston Scientific, Coloplast, Olympus, and Rocamed. Dr. Guido Giusti was a consultant for Boston Scientific, Coloplast, Cook, Lumenis, Olympus, and Rocamed.