
Abstract
Introduction:
Urethral strictures are a common urologic problem that could require complex reconstructive procedures. Urethral dilatation represents a frequent practiced intervention associated with high recurrence rates. Drug-coated percutaneous angioplasty balloons (DCBs) with cytostatic drugs have been effectively used for the prevention of vascular restenosis after balloon dilatation. To reduce restenosis rates of urethral dilatation, these balloons could be used in the urethra. Nevertheless, the urothelium is different than the endothelium and these drugs may not be distributed to the outer layers of the urethra. Thus, an experiment was performed to evaluate the distribution of paclitaxel (PTX) in the rabbit urethra after the inflation of a PTX-coated balloon (PCB).
Materials and Methods:
Eleven rabbits underwent dilatation of the posterior urethra with common endoscopic balloons after urethrography. Nine of these rabbits were additionally treated with PCB. The urethras of the two control animals were removed along with three more dilated with PCB urethras immediately after the dilatation. The remaining of the urethras were removed after 24 (n = 3) and 48 hours (n = 3). The posterior segments of the urethras were evaluated with hematoxylin and eosin staining as well as with immunohistochemistry with polyclonal anti-PTX antibody.
Results:
The two control specimens showed denudation of the urothelium after balloon dilatations and no PTX was observed. All specimens from dilated PCB urethras showed distribution of PTX to all layers of the urethra. The specimens that were immediately removed exhibited denudation of the urothelium without any inflammation. The specimens removed at 24 and 48 hours showed mild acute inflammation.
Conclusion:
PTX was distributed to the urothelial, submucosal, and smooth muscle layers of the normal rabbit urethra immediately after dilatation with a DCB. PTX and mild inflammation were present at the site 24 and 48 hours after the dilatation.
Introduction
A
Drug-coated percutaneous angioplasty balloons (DCBs) have been used effectively for dilatation of vascular stenosis. 6,7 The advantage of DCBs over the conventional percutaneous angioplasty balloons (CBs) is that they have the ability of releasing antiproliferative agents to the narrowed vessels, resulting in the reduction of local inflammation and restenosis rates. 8,9
The restenosis of previously treated urethral strictures is a common and challenging problem for urologists. 10 –12 Various studies indicate that restenosis has been associated with collagen-rich connective tissue with few fibroblasts and smooth muscle fibers in the scarred area. 13,14 The increase in type 3 collagen in comparison with type 1 collagen represents a tissue response and the result is urethral fibrosis and stenosis of the lumen. 15 Smooth muscle cells (SMCs) are the major collagen producers in the urethra. Paclitaxel (PTX) is an antineoplastic agent that stabilizes cellular microtubules and results in the inhibition of cell replication. 16 –18
PTX causes a dose-dependent inhibition of ureteral SMCs and urothelial cell proliferation. PTX reduces the production of type 3 collagen by SMCs. This antiproliferative nature of PTX prevents tissue response that leads to the development of ureteral strictures. 19 An effect on the urethral stricture formation has also been proposed for another Taxol, docetaxel. 20
Considering the mentioned, the concept of using DCBs with PTX in the treatment of urethral strictures seems quite interesting and promising. Nevertheless, the urothelium represents the most effective endothelial barrier for substances in the human body and may pose a significant obstacle for the distribution of PTX to the muscular layer of the urethra where PTX is expected to exert its effect on the SMCs. 21,22 PTX can also be distributed through the layers of the ureter, 23 which are shielded by urothelium, so we can expect that it can also penetrate the urothelium of the urethra. Nevertheless, it should be considered that the urothelium of the urethra gradually changes as it lines the urethra during its course from the bladder neck to the urethral meatus. The urothelium in the prostatic urethra is transitional, in the membranous and spongy urethra is pseudostratified and changes to stratified squamous at the fossa navicularis and meatus. 24 Thus, the distribution of PTX after balloon dilatation at the posterior urethra where most of the urethral strictures take place is questionable.
In this study, we investigate the distribution of PTX released by a DCB in the rabbit urethra.
Materials and Methods
Animals
Eleven domestic male rabbits weighing 2–2.5 kg were included in the experiment. The study protocol was approved by the responsible public services.
Materials
Nine percutaneous angioplasty balloons (IN Pact Admiral; Medtronic, Inc., Minneapolis, MN) containing the PTX (DCBs) and 11 CBs (Admiral Xtreme; Medtronic, Inc.) were used. PTX was released during the inflation phase of the balloon. All balloons were commercially available with indication for use in the vascular system. The dimensions of the balloons were 40 mm length and 6 mm diameter.
Anesthesia
Anesthesia was given to all rabbits for the experiment. Specifically, a mixture of the anesthetic drugs ketamine and xylazine was administered to ensure that the experiment is carried out without the agony and suffering of the animal. Also, antibiotic and analgesic treatment was given to all laboratory animals during the follow-up period.
Intervention
Each rabbit was placed in the supine position. Urethrography was performed before dilatation, and a 0.035-inch hydrophilic guidewire was inserted into the urethra under fluoroscopic guidance. A 7F urethral catheter was inserted over the hydrophilic guidewire and was exchanged for a stiff guidewire. The balloons were inserted over the stiff guidewire, inflated to their maximal diameter for at least 2 minutes, and then removed. The dilatation was always performed in the posterior urethra with CBs and immediately after with drug-eluting balloon. The CB was always the first to be inflated to avoid contamination of the control urethra with PTX.
Specimen removal
To study the distribution of the substance in the urethral wall, the 11 rabbits were divided into 4 groups.
Group A (n = 2): the urethras of the control rabbit population were obtained after the dilatation with balloon (sham).
Group B (n = 3): the urethras of the control rabbit population were removed immediately after dilatation with a DCB.
Group C (n = 3): the urethras were removed immediately 24 hours after dilatation with a DCB.
Group D (n = 3): the urethras were removed 48 hours after dilatation with a DCB.
Sample Examination
Pathology—immunohistochemistry
Samples from each urethra of groups A, B C, and D were isolated so that PTX can be detected by immunohistochemistry (IHC). The pathologist was blinded regarding the specimen groups. For pathology evaluation, the histology specimens were fixed in formalin and underwent a standard embedding process with paraffin. The 4-mm-thick hematoxylin- and eosin-stained (H&E) sections were mounted on gelatin-coated glass slides.
IHC allowed the study of the distribution of the substance in the various layers of the urethral wall. For the purpose, a special polyclonal anti-PTX antibody was used. IHC was performed on 4-mm-thick tissue sections, which were fixed with formalin, embedded with paraffin, and mounted on gelatin-coated glass slides. An electric pressure cooker with Trilogy retrieval solution (Cell Marque, Hot Springs, AR) was used for the deparaffinization, rehydration, and antigen retrieval for 30 minutes. Polyclonal antibody against Taxol (NBP1-05003; Novus Medical, Cambridge, UK) was used for the primary antibody, in a dilution of 1:3000. The sections were brooded with the primary antibody at room temperature for 1 hour, followed by a sequential 30-minute incubation with Dako EnVision Labelled Polymer (Dako North America, Inc., Carpinteria, CA). Diaminobenzidine (Dako North America, Inc.) was used as chromogen. Sections were counterstained with Harris hematoxylin (Vector, Burlingame, CA). In negative control slides, the same process was followed, with the differentiation of substitution of the primary antibody with 1% TBS.
Evaluation of specimens
The slides were evaluated using a standard light microscope. The microscope was attached with a camera (Nikon ECLIPSE 50i and Nikon HD color camera head DS-Fi2; Nikon GmbH, Dusseldorf, Germany). Three slides were obtained from each specimen for histology and three specimens for IHC. The presence of morphologic alterations and inflammation was evaluated in the case of histology. The presence of PTX and the location of the agent in the investigated slides were evaluated with IHC.
Results
Pathology
The evaluation of the specimens showed the existence of ruptures across the urethras of all the animals. These ruptures indicated that dilatation of the urethra using a balloon had mechanical effects on the urothelium of the specimens that were recognized in the pathologic evaluation (H&E staining). Acute inflammation was present in all specimens of groups C and D. Specimens of groups A and B hardly showed any inflammation.
IHC examination
PTX was detected in the urothelium and submucosal layer in the specimens of group A (sham). The substance was present almost in all layers of the specimens of groups B, C, and D. The result of the histologic alterations and the distribution of PTX are summarized in Table 1.
PTX = paclitaxel.
Figures 1 –4 show images of H&E staining and IHC of urethras treated by DCB and CB from all groups of this study.
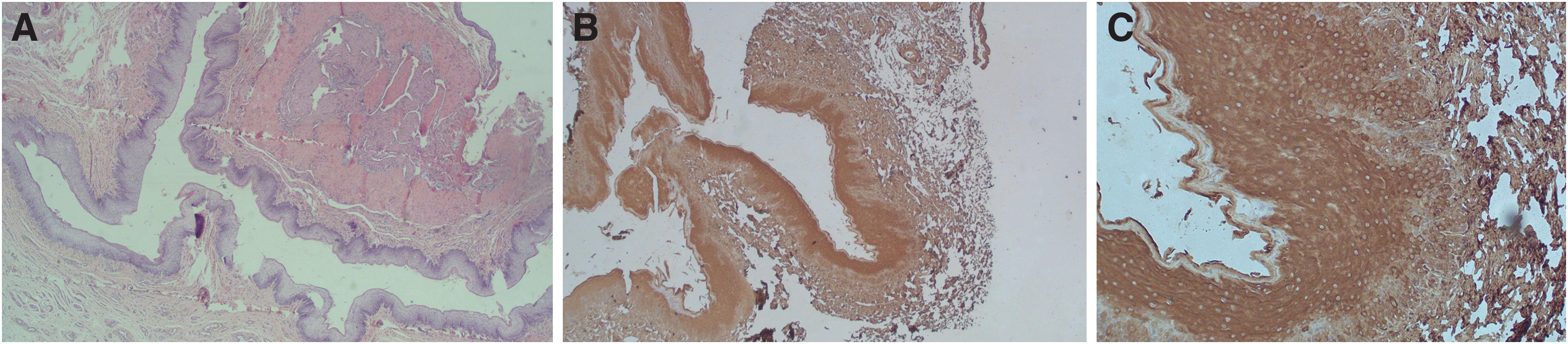
Histologic images of urethra removed immediately after dilatation.

Histologic images of urethra removed 12 hours after dilatation.

Histologic images of urethra removed 24 hours after dilatation.

Histologic images of urethra removed 24 hours after dilatation. There is significant inflammation in mucosa and extends to the submucosal layer (H&E, 2.5 × ).
Discussion
The objective of this experiment was to study the penetration of PTX through the urothelium to the different layers of the urethral wall after inflation of a DCB with PTX. Specifically, the muscular layer should be reached by PTX. The reduction of any restenosis is directly related to the reduction of collagen production by the SMCs that are located in the muscular layer. Since the urothelium represents the most impermeable barrier for substances in the human body, the penetration of PTX through it and the distribution of the drug to the muscular layer would provide clues for an effective use of DCBs in the urethra. 8,25 It should be noted that PTX was chosen because of the antiproliferative effect that exerts on the SMCs and the potential to reduce the production of collagen by these cells. 19
The examination of the specimens by IHC showed that the agent penetrated the urothelium, the submucosal layer, and reached the muscular layer of the urethra. PTX was distributed at all the layers immediately after the dilatation (group B, Fig. 1). This phenomenon could be attributed to the mechanical damage caused by the balloon to the urothelium and is documented by the denudation of the urothelium at all the specimens. Furthermore, alterations did not exist in the deeper layers and could be assumed that the low diameter of the balloons was the reason for that. It should be noted that the selection of the balloon sizes was aimed to reduce the mechanical damage to the ureteral wall. Significant mechanical damage could result in shedding of the substance in the ureteral wall and probably outside of the ureter. Thus, the substance would not be detected during the scheduled time periods and related tissue inflammation may have changed in severity. The histology did not show rupture of the deeper urethral layers and weakening of the urethral wall, and it could be concluded that the diffusion of the substance was in some extent related to the lipophilic nature of the drug. 26,27
These mechanical effects from balloon dilatation could be associated with the development of acute inflammation, which appeared in specimens of groups C and D. Specimens of group A and B hardly had acute inflammation probably due to the inadequate time between the dilation and harvesting of the uretras (immediate groups). Nevertheless, mild inflammation developed and was clearly present during the first 24 hours (group C) and was also present at the 48 hours specimens (group D).
Limitations of this study include the use of DCBs designed for the treatment of vascular diseases. The arterial strictures are different from the urethra in terms of histology and mechanism of restenosis. In case of atheromatosis, the atherosclerotic lesions and the arterial stenosis develop with the progression of the disease. 28 The main reason of restenosis after balloon dilatation is the inflammation that is caused by the mechanical action of the balloon on the endothelium, which leads to proliferation and migration of vascular SMCs. 29 PTX has an inhibitory role in this phenomenon. On the contrary, the restenosis of the urethra is related to the proliferation of SMCs and the production of connective tissue with an increase of collagen type I over collagen type III. In fact, the normal urethral spongiosum is composed of 75.1% collagen I and 24.9% collagen III. When this ratio is altered in favor of collagen I, as in the case of urethral stricture, the tissue becomes more fibrotic and less compliant. 13,14,30
Another limitation is that the distribution of PTX was only evaluated in the posterior urethra. The posterior urethra consists of transitional epithelial cells, whereas the anterior urethra is covered with pseudostratified columnar epithelium. 24 This study focused on the posterior strictures because of the higher incidence of these strictures. 2,24,31 Follow-up of the rabbits extended over a period of 48 hours. Progression of the inflammation and presence of PTX for longer periods of time were not evaluated. A longer period of observation would probably provide more information. It is important to note that the urethras were normal before the dilatation, and the distribution of PTX could be different in the strictured urethras.
The success of the DCBs in the cardiovascular field could hold a promise for the management of urinary tract strictures. Nevertheless, the different histology of the urothelium in comparison with the endothelium may pose a significant obstacle for the effective use of these devices in the urinary tract. A question that could define the use of DCBs in the urethra is whether the drug could reach the site of interest to exert its action, namely the smooth muscle layer of the urethra. Thus, this study was designed to provide a clear answer to this question. It would have been inappropriate to consider any possible use of DCBs in the urethra without even knowing whether the drug penetrates the urothelium and spreads in the underlining layers. Yet, several questions remain unanswered regarding the use of DCBs in the urethra. The concentration of the substance at the treatment site, the quantity of the substance that is released from the DCB, the time that it remains at the site remain questions to be answered. In addition, there is no specific evidence on the correlation of the substance concentration and the reduction of inflammation as well as the reduction of SMC proliferation at the site. Even technical issues such as the time that the balloon remains inflated and the possible correlation with the mentioned parameters have not been answered. Thus, only further investigation could provide the background for the use of DCBs in the urethra.
Considering the above, this study clearly showed that PTX was distributed in all the layers of the posterior urethral wall of the normal rabbit urethra and eventually reached the SMCs immediately after dilatation of a DCB carrying the substance. Mild inflammation was developed at the site for the 48 hours follow-up period and PTX was still detected during this period. PTX is known to be effective on the SMCs that are responsible for the production of collagen and as a result restenosis of the urethra. Thus, the restenosis rate after dilatation of the urethra with a DCB could be reduced. Further investigation is needed to draw conclusions on an effective therapeutic strategy.
Conclusion
PTX was distributed to the urothelial, submucosal, and smooth muscle layers of the normal rabbit urethra immediately after dilatation with a DCB. PTX and mild inflammation were present at the site 24 and 48 hours after dilatation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.